-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3517-3522
doi:10.5923/j.ajmms.20251510.51
Received: Sep. 26, 2025; Accepted: Oct. 22, 2025; Published: Oct. 28, 2025

Evaluation of the Result of an Optimized Method for the Prevention of Pleural Complications After Urgent Thoracotomy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLVakhidov Utkir Hakimovich, Boltaev Timur Shavkatovich
Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Vakhidov Utkir Hakimovich, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Urgent thoracotomy, as a form of surgical intervention, retains its clinical significance despite the development of minimally invasive technologies. The purpose of the study: improving the results of postoperative treatment of patients after urgent thoracotomy by developing and implementing a set of preventive measures aimed at reducing the frequency of pleural complications. Materials and methods: the data of examination and treatment of 98 patients who underwent urgent thoracotomy (UT) for various acute pathological processes in the organs of the thoracic cavity were analyzed. All patients, depending on the treatment method, were divided into 2 groups: control group I and main group II. The control group consisted of 48 patients who underwent traditional surgical tactics, including standard schemes for drainage of the pleural cavity, as well as an approach without using an algorithm to determine the timing of follow-up and drainage removal. The main group included 50 patients who underwent the proposed preventive model, including the author's method of targeted drainage (utility model UZ № FAP 2441 dated 03.19.2024) and an algorithm for postoperative management based on predicting the risk of a complicated course of the postoperative course. Results: the duration of drainage in the main group averaged 4,1±1,3 days, while in the control group it was 5,6±1,7 days. In general, the duration of drainage was reduced by 1,4 times, despite the fact that in the main group the proportion of patients with initial intra-pleural bleeding was higher. The average duration of hospitalization in the main group was 10,6±2,7 days, while in the control group it was 14,5±4,3 days. The difference reached almost 4 days, which confirms the clinical stability of the patients' condition at an earlier stage. Conclusion: the developed method of drainage of the pleural cavity with the targeted installation of a second drainage through the lumen of the main one provides complete sanitation of hard-to-reach areas with minimal invasiveness. The proposed technique has shown high clinical effectiveness and has become the basis for the formation of a comprehensive preventive approach to the management of patients after UT.
Keywords: Thoracotomy, Drainage of the pleural cavity, Hemothorax, Pneumothorax
Cite this paper: Vakhidov Utkir Hakimovich, Boltaev Timur Shavkatovich, Evaluation of the Result of an Optimized Method for the Prevention of Pleural Complications After Urgent Thoracotomy, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3517-3522. doi: 10.5923/j.ajmms.20251510.51.
Article Outline
1. Introduction
- Urgent thoracotomy remains a clinically recognized surgical intervention despite the development of minimally invasive technologies [4]. To date, a number of clear clinical indications have been established in the practice of emergency thoracic surgery. Among them, the main proportion is massive bleeding into the pleural cavity, violations of the tightness of the respiratory circuit and obstructive phenomena that cannot be conservatively corrected. In all these cases, delaying the intervention carries a high risk of fatal consequences, even if the patient has. However, it is important to emphasize that the formal formulations conceal nosologically diverse and anatomically complex situations, each of which requires a differentiated approach [2,4,9].Special attention in the literature is paid to patients with combined forms of pathology. Situations involving simultaneous rib fractures, open pneumothorax, and lung damage require complex solutions. One-step sanitation is not enough here. In this case, it becomes necessary to apply well-thought-out drainage routes, take into account the multiplaneity of the lesion and coordinate the volume of intervention with the patient's functional capabilities. It is this category of patients that demonstrates the most unstable postoperative course and the highest risk of complications [3,7,12].Against this background, the task of developing preventive measures that can not only reduce the incidence of complications, but also be adapted to a diverse and often vulnerable patient population becomes particularly relevant [1,5].The use of drainage in thoracic surgery makes it possible to solve the issues of diagnosis and treatment of patients who have undergone urgent thoracotomy in a new way, improve the results of surgical treatment, reduce postoperative complications and mortality to a minimum and shorten the duration of the patient's stay in the hospital. In surgery of postoperative complications, it has become the method of choice for the correction of pleural complications, which made it possible to significantly reduce the number of repeated interventions [6,8].The aim of this study is to improve the results of postoperative treatment of patients after urgent thoracotomy by developing and implementing a set of preventive measures aimed at reducing the frequency of pleural complications.
2. Material and Research Methods
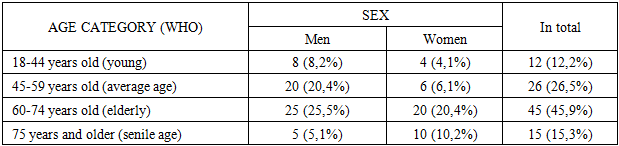
- The data of examination and treatment of 98 patients who underwent urgent thoracotomy (UT) for various acute pathological processes in the organs of the thoracic cavity were analyzed. All patients were treated at the Tashkent City Clinical Hospital № 7 from 2015 to 2025. Depending on the follow-up period and the postoperative management tactics used, the patients were divided into two groups of comparable volume.All patients, depending on the treatment method, were divided into 2 groups: control group I and main group II. The control group consisted of 48 patients who were treated from 2015 to 2019 inclusive. In this group, traditional surgical tactics were used, including standard schemes for drainage of the pleural cavity, as well as an approach without using an algorithm to determine the timing of follow-up and drainage removal. The main group included 50 patients who received treatment in 2020-2025. In this group, the proposed preventive model was implemented, including the author's method of targeted drainage (utility model UZ № FAP 2441 dated 03.19.2024) and an algorithm for postoperative management based on predicting the risk of a complicated course of the postoperative course.The analysis of the age and sex structure of the studied contingent, represented by 98 patients who underwent UT, showed the predominance of older age groups, as well as the dominance of the male sex, which reflects the epidemiological and clinical features of chest pathology (table 1).
|
|
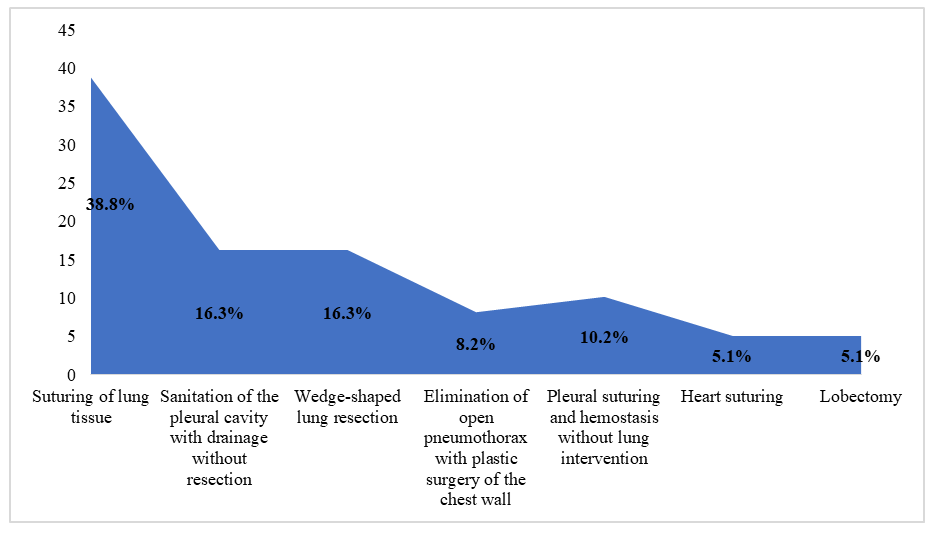 | Figure 1. The nature and volume of surgical interventions performed |
3. Results and Their Discussions
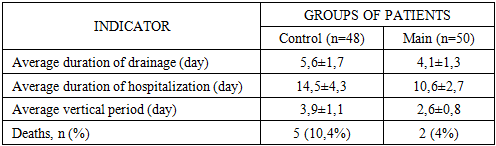
- Surgical tactics under the traditional approach were characterized by variability and lack of unified principles. In some cases, the intervention was limited to pleural cavity sanitation and drainage, while in other cases, lung tissue resections of various volumes, including lobectomies, were performed. Drainage support was also not standardized, as we installed one drainage for some patients, and two drainage tubes in the presence of a hemothorax. Decisions on drainage removal were usually made empirically, without using objective scales for assessing the dynamics of pleural discharge, X-ray picture, or clinical condition.In the postoperative period, almost all patients had a pronounced inflammatory response, especially in the first three days after the intervention, which was reflected in the dynamics of body temperature, leukocyte formula, C-reactive protein level and erythrocyte sedimentation rate. In patients with initial intrapleural bleeding, compared with patients without it, there was a higher incidence of complications, including clotted hemothorax (18,8%), EP (12,5%), infected pleurisy, recurrent pneumothorax, as well as the need for repeated interventions, both with drainage and retoracotomy. At the same time, the duration of drainage and hospitalization in this subgroup was statistically significantly higher, and the timing of verticalization and recovery turned out to be later.The revealed tendency to increase mortality in patients with initial bleeding deserves special attention. If in the group without hemothorax it was 6,3%, then in the presence of bleeding this indicator increased to 12,5%. The causes of death in some cases were directly correlated with pleural complications in the form of EP, sepsis, respiratory failure, which developed against the background of prolonged drainage, decreased activity of the patient and ineffective sanitation of the pleural cavity.A summary analysis of the data obtained suggests that the existing traditional management scheme for patients after UT is largely based on the individual experience of the surgeon and does not take into account a number of key risk factors. The existing algorithmization of the decision-making system regarding the choice of drainage volume, the timing of drainage removal, as well as the organization of postoperative follow-up in debilitated and elderly and senile patients leads to a high frequency of complicated course and difficult rehabilitation.Based on the above, it is obvious that there is a need to develop an integrated approach, including the improvement of drainage techniques adapted to the nature of the intervention and the risk zone, based on objective clinical, instrumental and functional criteria. Such a solution should not only increase the efficiency of pleural cavity sanitation, but also ensure timely and safe removal of drainage load, accelerate patient activation and reduce the risk of pleuropulmonary complications.Based on the identified shortcomings of traditional drainage schemes and in order to increase the efficiency of pleural cavity sanitation, we have developed a new drainage method that is protected as a useful model. The essence of the method is as follows: a basic silicone drain with a diameter of 0,8-1,0 cm and a length of 50 cm is inserted into the pleural cavity through a single access (VII or VIII intercostal space, between the middle and posterior submuscular lines). The drainage has four lateral openings and is carried out along the lateral wall of the chest with a direction to the dome of the pleura. After installing the main drain, a second, thinner silicone drain with a diameter of 6 mm is passed through its lumen, which is precisely positioned in the most critical areas of the pleural cavity, where accumulation of pathological contents is likely.These areas include: interlobular crevices; spaces between adhesions; stump of the lung after resection (with wedge-shaped resections, lobectomy, etc.).Thanks to this solution, adequate, targeted drainage is achieved without the need for additional punctures of the chest wall, which reduces invasiveness, improves cosmetic results and reduces pain. The use of a single skin access avoids injury to the intercostal neurovascular bundles and muscle structures, especially in the upper anterior chest.A comparative analysis of the postoperative period in patients of the control and main groups, presented in table 3, allowed an objective assessment of the clinical effectiveness of preventive tactics. The comparison was based on four key parameters reflecting the dynamics of recovery, the degree of functional impairment and outcomes. Among them, the duration of drainage, the duration of hospitalization, the timing of patient activation (verticalization) and the frequency of deaths were analyzed.
|
4. Conclusions
- The traditional approach to the management of patients after UT is accompanied by a high incidence of pleural complications (79,2%), repeated interventions (25%) and mortality (10,4%), especially in patients with initial intrapleural bleeding upon admission. In this subgroup, coagulated hemothorax, pleural empyema, recurrent pneumothorax, difficult rehabilitation of the pleural cavity and late activation were significantly more common. The data obtained indicate the insufficiency of the traditional tactics of drainage of the pleural cavity and the postoperative tactics of administration, which justifies the need for its improvement.The developed method of drainage of the pleural cavity with the targeted installation of a second drainage through the lumen of the main one provides complete sanitation of hard-to-reach areas with minimal invasiveness. The proposed technique has shown high clinical effectiveness and has become the basis for the formation of a comprehensive preventive approach to the management of patients after UT.