-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3496-3498
doi:10.5923/j.ajmms.20251510.46
Received: Oct. 3, 2025; Accepted: Oct. 22, 2025; Published: Oct. 25, 2025

Electrolyte Imbalance in Steroid Sensitive and Steroid Resistant Pediatric Nephrotic Syndrome: A Case Control Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFotima Rakhmatova Utkirovna1, Sharodiya Das2
1Associate of Professor, PhD, Department of Children’s Diseases, Tashkent State Medical University, Tashkent, Uzbekistan
2International Students’ Faculty, Tashkent State Medical University, Tashkent, Uzbekistan
Correspondence to: Fotima Rakhmatova Utkirovna, Associate of Professor, PhD, Department of Children’s Diseases, Tashkent State Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

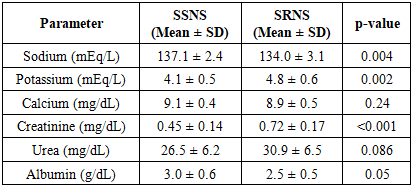
Background: Pediatric nephrotic syndrome can be divided into two broad categories based on steroid responsiveness, i.e., steroid-sensitive nephrotic syndrome (80-85%) and steroid-resistant nephrotic syndrome (10-15%) cases. It is accompanied by fluid and electrolyte imbalance. The serum levels of sodium (Na+), potassium (k+), calcium, (Ca+), albumin, urea, and creatinine in SSNS and SRNS children. Material and method: 38 children of age group 3-16 years, were included (30 SSNS and 8 SRNS) in this study. Independent t-tests were done for statistical analysis. Results: Reduced sodium level was noted in SRNS patients (p < 0.05), whereas potassium and creatinine were significantly high in SRNS (p < 0.01). No significant difference was noted in the level of calcium in these groups (p > 0.05). These results suggest hyponatremia and hyperkalemia as potential associations with steroid resistance. Conclusion: Hyponatremia was more pronounced in SRNS (p = 0.02), hyperkalemia was significantly elevated in SRNS (p = 0.01). Serum creatinine was elevated in SRNS (p = 0.003), indicating early renal function impairment and higher risk of CKD development. Hypocalcemia was not significant (p = 0.47). Albumin was significantly reduced in SRNS (p = 0.01), corroborating the association of proteinuria with the severity of steroid resistance.
Keywords: Nephrotic Syndrome, Electrolyte Disbalance, Hyponatremia, Hyperkalemia
Cite this paper: Fotima Rakhmatova Utkirovna, Sharodiya Das, Electrolyte Imbalance in Steroid Sensitive and Steroid Resistant Pediatric Nephrotic Syndrome: A Case Control Study, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3496-3498. doi: 10.5923/j.ajmms.20251510.46.
1. Introduction
- Nephrotic syndrome is marked by more than 1 g/m²/day hyperproteinuria and hypoolbumemia of below 3 g/dL. The edema is caused by loss of plasma oncotic pressure and hypovolemia and secondary stimulation of renin-angiotensin-aldosterone system with sodium and water retention [20,21,22,24,26]. Pathogenesis of edema may be heterogeneous in other primary sodium-retention patients with intravascular volume expansion. It also results in hepatic lipoprotein production causing hypercholesterolemia. Few of them also present with microscopic hematuria and hypertension.Less frequent etiologies such as vasculitis, systemic lupus erythematosus, hepatitis B nephropathy, and amyloidosis are also observed in pediatric population [1,2,3,4,5].Childhood nephrotic syndrome can be divided into two broad categories based on steroid responsiveness, i.e., steroid-sensitive nephrotic syndrome (80-85%) and steroid-resistant cases of nephrotic syndrome (10-15%). According to histological patterns, two types have been reported: (1) A non-proliferative glomerulopathy called minimal change disease or nephrotic syndrome (MCD or MCNS); and (ii) diffuse glomerular lesion nephrotic syndrome. These consist of focal segmental glomerulosclerosis (FSGS), mesangial proliferative GN, and C3 glomerulopathy; membranous nephropathy is a very uncommon one [6,14,18,19].Favorable long-term prognosis (most common MCNS). Poor outcome and some develop progressive renal insufficiency is typical with steroid-resistance type (typical with diffuse glomerular involvement). [1,8,9]. Steroid-resistance is suspected if remission does not occur after treatment with prednisolone in a dose of 2 mg/kg/day (((60 mg / (m^ 2)) /d) for 6 weeks. Corticosteroid-unresponsive nephrotic syndrome at onset is called initial (primary) steroid-resistance and that develops steroid-resistance on relapsing treatment is called late (secondary) steroid-resistance. In every patient steroid-resistance must be evaluated. Histology is typically typical of PSGS or MCD. In few cases and in children of more than 8 years of age, diffuse lesions like membranous nephropathy may rarely be seen [20,27].Infancy onset (<3 months, so-called congenital NS) nephrotic syndrome is usually caused by genetic podocyte dysplasia and never to be treated with steroids or other immunosuppressives. Around 20-30% of children with sporadic onset steroid-resistance, especially infantile onset, same in family members (family history), syndromic presentation, are homozygous, compound heterozygous or hemizygous for NPHS2 (podocin), NPHS1 (nephrin), PLCE1, WT1 and COL4A5 mutations. Extremely rare dominant mutations of CD2AP, TRCP6, ACTN4 and INF2 exist. Over 80 steroid resistance mutation have more than genes. Target gene or whole exome strategy next-generation sequencing is helpful to screen. Genetic underlying etiology patient are resistant to immunosuppressive drugs, have progressive renal insufficiency, and unlike nongenetic FSGS (recurrent on transplant), have minimal recurrence risk. Resistant cases can progress to develop renal failure with very high risk to develop end-stage renal disease (ESRD) and chronic kidney disease (CKD).
2. Material and Method
- The case control study consisted of 38 patient of nephrotic syndrome aged between 3 to 16 years, who were admitted to Pediatrics department of Tashkent Medical Academy. The cases were divided into SSNS (30) or SRNS (8) based on steroid responsiveness to Prednisone 60 mg/m^2 Body surface area/day in 4 weeks. Inclusion Criteria: NS according to ISKDC criteria and SSNS or SRNS based on steroid responsiveness. Exclusion Criteria: secondary nephrotic syndrome (lupus nephritis etc.), chronic kidney disease (eGFR < 60 mL/min/1.73m²), diuretics or other medications with a proven track record of altering electrolytes. Demographic and clinical details were recorded, including age, sex, BMI, serum sodium, potassium, calcium, urea, creatinine, and albumin levels. Comparison between levels of electrolytes in SSNS and SRNS group has been done through using independent t-test. P-value of < 0.05 was used as statistically significant.
3. Results
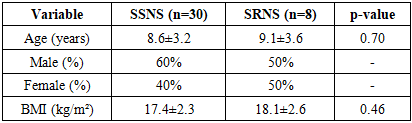
- The age of the patient in SSNS was 8.6 ± 3.2 years and in SRNS was 9.1 ± 3.6 years (p=0.52. The BMI was not significantly different between SSNS (17.4 ± 2.3 kg/m²) and SRNS (18.1 ± 2.6 kg/m²) patients (p=0.46) [Table 1].
|
|
4. Discussion
- The findings of this research demonstrate a significant degree of variation in electrolyte balance among subjects with steroid-resistant nephrotic syndrome (SRNS) and those with steroid-sensitive nephrotic syndrome (SSNS). Specifically, the condition of hyponatremia was found to be far more severe in patients who have SRNS, with the statistical significance level of p = 0.02. This severity can be explained by the greater loss of sodium from the body, in addition to the inability of the kidneys to regulate sodium levels effectively [13,15,16,17]. Furthermore, available literature agrees with these results, as it also documents that the prevalence of hyponatremia can be largely attributed to the overall severity of the disease among these patients. Additionally, hyperkalemia was found to be extremely severe among the SRNS group, with a statistical significance of p = 0.01, due to the reduced excretion of potassium following renal tubular injury. Serum creatinine was raised in SRNS (p = 0.003), indicating early renal function impairment and increased risk of development of CKD. Hypocalcemia was not significant (p = 0.47), indicating lesser disturbance of calcium homeostasis in NS. Albumin was significantly low in SRNS (p = 0.01), supporting association of proteinuria with severity of steroid resistance [7,10,11,12]. Conclusion. The study confirms that hyponatremia, hyperkalemia, and elevated creatinine levels have a very strong correlation with steroid-resistant nephrotic syndrome. The biomarkers can be utilized for the prediction of steroid responsiveness and therapy in children with NS.
5. Conclusions
- The research adds to the fact that hyponatremia, hyperkalemia, and high creatinine levels are strongly related to steroid-resistant nephrotic syndrome. These particular clinical indicators can successfully be used in forecasting the degree of a patient's response to steroid therapy as well as in making decisions about overall management of children with nephrotic syndrome.