-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3466-3469
doi:10.5923/j.ajmms.20251510.39
Received: Sep. 15, 2025; Accepted: Oct. 12, 2025; Published: Oct. 23, 2025

Diagnostic Significance of Platelet Aggregation Activity in Patients with Resistance to Antiplatelet Agents in Patients with Coronary Heart Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKhodjanova Shakhnoza Iskandarovna1, Alavi Anis Lutfullayevich2, Kodirova Shoira Abdurahmanovna1
1Tashkent Medical Academy, Uzbekistan
2Republican Specialized Scientific and Practical Medical Center for Therapy and Medical Rehabilitation, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

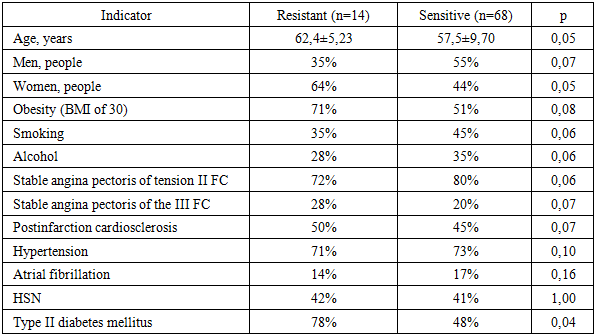
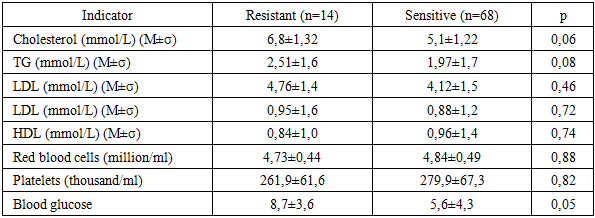
The goal. To determine the incidence of aspirin resistance in patients with coronary heart disease and to identify risk factors for the development of resistance to acetylsalicylic acid in patients with coronary heart disease. Materials and methods. The study included: 80 patients with stable forms of coronary heart disease with stable angina pectoris who received a standard dose of aspirin 75 mg/day for a long time. Platelet aggregation (AT) was measured using a laser analyzer, which was used as an inductor with final concentrations of 0.1, 1.0, and 5.0 mmol. Resistance criterion: ADP ≥72% at 5.0 mmol. Results. 17% of patients taking aspirin at a standard dose of 75 mg/day were resistant to aspirin, and a third of them had been taking aspirin for more than 5 years. Inadequate response to aspirin intake was significantly often observed in women and the elderly (70% and 80%). When analyzing the results of routine laboratory tests in patients with aspirin resistance, there was a tendency to higher cholesterol and glucose levels (p 0.05). Possible risk factors for the development of ASA resistance are hypercholesterolemia and hyperglycemia, since aspirin resistance was more common in patients with diabetes (11 out of 14, respectively) and obesity (10 out of 14, respectively). Conclusion. Given the high rates of ADP-induced platelet aggregation in one quarter of patients with coronary artery disease who have been taking aspirin for more than 5 years, as well as with concomitant diabetes mellitus and obesity, it is necessary to conduct a study of this aggregatogram indicator in order to determine the adequacy of drug correction in order to control antithrombotic therapy in this category of patients.
Keywords: Acetylsalicylic acid, Aspirin resistance, Coronary artery disease, Platelet aggregation
Cite this paper: Khodjanova Shakhnoza Iskandarovna, Alavi Anis Lutfullayevich, Kodirova Shoira Abdurahmanovna, Diagnostic Significance of Platelet Aggregation Activity in Patients with Resistance to Antiplatelet Agents in Patients with Coronary Heart Disease, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3466-3469. doi: 10.5923/j.ajmms.20251510.39.
1. Relevance
- Coronary heart disease (CHD) has been a leader in the list of the most significant social problems in terms of prevalence and risk of complications for more than half a century. According to the recommendations of the European Society of Cardiology for the treatment of coronary Heart Disease (2013), drug therapy includes nitrates, beta-blockers, calcium antagonists, and lipid-lowering agents. Also, an important condition for reducing mortality in this category of patients is adequate lifelong secondary cardiovascular prophylaxis, based on antiplatelet therapy [1].Among the main etiopathogenetic factors of coronary artery disease, coronary atherosclerotic thrombosis is considered as the main factor in the progressive course of the disease, the development of acute coronary syndrome (ACS), as well as sudden fatal events. Over the past 20 years, the mechanisms of this process and the regulation of hemostasis have been actively studied, and it has been proven that, along with other factors (endothelial dysfunction, tissue factor), platelets play a fundamental role. It is known that platelets are the first to react to the rupture of atherosclerotic plaque and form the basis for the formation of an arterial thrombus. Platelets come into contact with the subendothelial layer, in particular with the main stimulator of adhesion — collagen, form processes with the formation of platelet conglomerates (aggregation) and adhere (adhesion) in these areas, creating a white thrombus. Platelet activation is carried out by catecholamines, thrombin, ADP, serotonin, collagen, and thromboxane A2, a metabolic product of arachidonic acid. Therefore, it is the stabilization of hemostasis processes that occupies one of the leading places in the treatment and prevention of diseases of the cardiovascular system [2,3]. In the last decade, there has been a growing trend towards increasing interest in assessing the functional activity of platelets due to their key role in atherothrombosis and the progressively expanding use of disaggregants in the prevention of vascular disasters. Acetylsalicylic acid (ASA) is one of the most widely used medicines in the world, which by its characteristics meets the basic requirements for antiplatelet drugs used to treat and prevent acute manifestations of atherothrombosis, long-term ischemic effects of atherosclerosis and related deaths. And also, aspirin has the largest evidence base among all antiplatelet drugs. [1,4,5,6,7,8,9]. Candidates for primary prevention are patients over 50 years of age who have several risk factors for ischemic heart disease, such as diabetes mellitus, smoking, hypercholesterolemia, and arterial hypertension [10]. However, recently there have been more and more studies showing that 15-30% of patients develop resistance to aspirin, especially in patients who take it in low doses for a long time. Therefore, the problem of so-called "aspirin resistance", which has become one of the most discussed topics of antiplatelet therapy, attracts close attention. Aspirin resistance is the inability of ASA to prevent the development of thrombotic complications, which is based on the inability to inhibit ThA2 synthesis, as well as reduce platelet aggregation, detected by various laboratory tests [11,12]. Such patients retain increased platelet activity, despite ongoing antiplatelet therapy, which is associated with the risk of recurrent cardiovascular events. Moreover, the occurrence of such situations during aspirin therapy is a prognostically unfavorable factor and is accompanied by a higher risk of complications [13]. Aspirin resistance is a multifactorial phenomenon, as sensitivity to aspirin can change under the influence of different mechanisms. Currently, the most likely clinical causes of aspirin resistance are: female sex, old age, the prevalence of atherosclerosis, hypertension, diabetes mellitus, obesity, infections/inflammation, heart failure, smoking, obstructive pulmonary disease, hyperuricemia, heavy physical activity and stress [14,15,16,17,18]. Therefore, the problem of so-called "aspirin resistance", which has become one of the most discussed topics of antiplatelet therapy, attracts close attention. This fact indicates the need to monitor the individual sensitivity of patients to aspirin in patients with coronary heart disease (CHD) for timely correction of antiplatelet therapy.The purpose of the study. Assessment of platelet aggregation activity in patients with coronary artery disease and determination of risk factors for the development of ASA resistance.
2. Materials and Methods
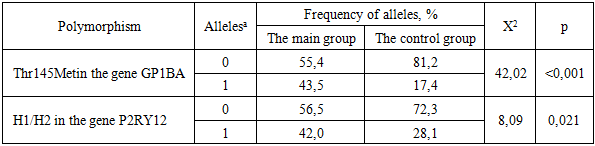
- The study included 82 patients with stable forms of coronary heart disease with stable angina pectoris (SSN) FC II 62 (77.5%) people, FC III — 10 (12.1%). The average age was 68.4 ±9.3 years. The number of patients with hypertension (GB) was 60 (73.1%), and 46 (56.0%) with postinfarction cardiosclerosis. Patients with HF were divided into 4 groups according to the prescription of ASA. Group 1 consisted of patients who did not receive aspirin, the second group consisted of patients taking aspirin for up to 1 year, the third group consisted of patients taking aspirin from 1 year to 5 years, and the fourth group included patients taking aspirin for over 5 years. According to the results of the determination of aspirin resistance, patients were divided into 2 groups based on the presence of aspirin resistance. The follow-up period was 12 months. The degree of spontaneous and ADP-induced platelet aggregation was studied on a Biola LA230 two-channel laser platelet aggregation analyzer. The method is based on the analysis of fluctuations in light transmission of a platelet- and plasma-enriched sample with the addition of an adenosine diphosphate (ADP) inducer at final concentrations of 0.1, 1.0, and 5.0 micrograms/ml, followed by computer processing using the AGGR program. The normal activity limits of the platelet aggregation process with the addition of 5.0 mmol of ADP are 25-72%. The level of platelet aggregation with 5.0 mmol of ADP ≥72% was used as a criterion of resistance. The molecular genetic research included: DNA isolation, determination of DNA quality and concentration, electrophoresis in 1-1.5% agarose gel for qualitative DNA analysis, primer design, polymerase chain reaction - PCR. The result was evaluated as a normal homozygote (0), heterozygote (1), and mutant homozygote (3). Genetic studies were performed to determine the polymorphism of the alpha subunit GP1BA and mutation of the platelet ADP receptor P2RY12. Statistical processing of the research results was carried out using the Statistica 6.0 statistical software package.
3. The Results of the Study
- According to the results of the study of platelet aggregation activity, 14 (17.1% and the average degree of platelet aggregation with 5.0 mmol of ADP was 82.1%) patients with no reaction to aspirin were identified. The clinical and anamnestic characteristics of patients with aspirin-sensitive and resistant Hf are presented in Table 1.
|
|
|
4. Conclusions
- Given the high rates of ADP-induced platelet aggregation in one quarter of patients with coronary heart disease who have been taking aspirin for more than 5 years, it is necessary to conduct a study of this aggregatogram indicator in order to determine the adequacy of drug correction in order to control antithrombotic therapy in this category of patients. Possible risk factors for the development of ASA resistance are hypercholesterolemia and hyperglycemia, since aspirin resistance was more common in patients with diabetes and obesity.