-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3456-3459
doi:10.5923/j.ajmms.20251510.37
Received: Aug. 28, 2025; Accepted: Sep. 21, 2025; Published: Oct. 16, 2025

Specificity of Morphological and Structural Changes in the Placental Papillae Under the Influence of Infections of Various Etiologies and Their Analysis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKh. A. Rasulov1, Kh. J. Beknazarov2, U. O. Mavlonov3, B. D. Eshonkulova1
1Tashkent Pediatric Medical Institute, Uzbekistan
2Republican Specialized Scientific and Practical Medical Center of Neurosurgery, Uzbekistan
3Zangiata Specialized Hospital No.1
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Relevance of the topic: One of the factors negatively affecting the morphological structures of the placenta is the inflammatory process. This process can cause various complications in the fetus and mother at any stage of pregnancy. Morphological analyses show that premature placental abruption due to inflammation is observed in 60-85% of cases. The study of pathomorphological changes under the influence of infectious factors is important for the prevention of pregnancy complications and the application of effective treatment measures. Materials and methods of research: In 2020-2022, at the Tashkent City Pathoanatomical Bureau and the Zangiata Special Hospital No. 1, the placental structures of a total of 39 pregnant women with ARVI (n=6), herpes (n=4), viral hepatitis (n=5), and PCR, as well as COVID-19 (n=15) with positive antigen tests, were studied by pathomorphological methods. The data were processed using Microsoft Excel and Statistica 6.0, and the correlation of morphological parameters was assessed using the Spearman correlation coefficient. Results of the study: The highest incidence of infectious factors was observed in women aged 25-35, and the same result was found for age indicators. The main pathomorphological changes in the placenta were manifested in the form of subchorionic fibrin foci in the perevillez area, vascularization of chorionic villi, atherosis, and microthrombosis. Early involuntary changes were observed in patients with COVID-19. Conclusion: in pregnant women with COVID-19, pathomorphological changes in the placenta are more often detected in the third trimester, which indicates a high risk in reproductive age. These changes indicate the onset of early involution.
Keywords: Placenta, Chorionic villi, Pregnancy, Viral infection, SARS-CoV-2
Cite this paper: Kh. A. Rasulov, Kh. J. Beknazarov, U. O. Mavlonov, B. D. Eshonkulova, Specificity of Morphological and Structural Changes in the Placental Papillae Under the Influence of Infections of Various Etiologies and Their Analysis, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3456-3459. doi: 10.5923/j.ajmms.20251510.37.
1. Relevance of the Topic
- The influence of any negative factors at any stage of pregnancy can lead to changes in the structures of the placenta, as a result of which dysfunction of functional subunits important for the life of the fetus and mother manifests itself with clinical and symptomatic manifestations. As a result of recent therapeutic, preventive, and scientific research work, we can notice a decrease in such unfavorable conditions as complications of childbirth, maternal and infant mortality. At the same time, the study of morphological changes in the structures of the placenta, which is a functional unit of pregnancy, under the influence of natural, experimental, and other factors, creates a basis for analyzing the expected positive and negative consequences in the future, developing the necessary treatment and preventive measures. One of the factors negatively affecting the morphological structures of the placenta is the inflammatory process, and as a result of the influence of this process, it is known from literature and practical work that at any time of pregnancy it can cause various complications in the fetus and mother. According to morphological analyses, as a result of inflammatory processes, premature placental abruption at different stages of pregnancy was observed in 60-85% of cases [1,8,9]. Despite the processes of compensatory replacement in the placenta, an increase in the parameters of the negative deviation of morphological changes in the dead structures is observed, which directly leads to fetal hypoxia. Among the etiological factors causing the inflammatory process, it has been established that the influence of viral, bacterial, and other infectious factors varies at different times, and changes in the structures of the placenta are diverse. Among the literary analyses conducted, Lutsenko M.T. describes the effects of herpes simplex virus and cytomegalovirus on changes in placental structures, particularly in the villi. According to him, the distance between syncytiotrophoblasts and blood vessels in the placental villi is increased, and fibrous structures have formed in this expanded area [2,3,6]. In the studies by Sherstyuk S.A., analysis of morphological changes in the placentas of pregnant women infected with HIV revealed that chronic placental insufficiency occurs with nonspecific involutional-dystrophic changes accompanied by acute circulatory system disorders. He directly associates these morphological changes with placentitis that develops against the background of deciduitis, villitis, and intervillitis [3,10,13]. In A.V. Yakimova’s studies on the effects of coronavirus infection, the main indicators of changes in placental structures were identified as the degree of necrosis observed in the syncytiotrophoblast and the manifestation of chronic histiocytic intervillitis [4,5,8,15].Information about the influence of various infectious factors on the origin of pathomorphological changes observed in the placental system is important for preventing arising complications and for the proper application of treatment measures during different stages of pregnancy. Studying pathomorphological changes in the placenta under infectious conditions is crucial for both the fetus and the mother, and it holds particular significance due to its relevance.Objective: To analyze morphological changes in placental structures under the influence of infectious factors of various etiologies.
2. Research Subjects and Methods
- Between 2020 and 2022, placental structures of pregnant women (total n=39) with histories of acute respiratory viral infections (ARVI, n=6), herpes (n=4), viral hepatitis (n=5), and COVID-19 positive PCR and antigen tests (n=15) were studied pathomorphologically in the Pathoanatomy Department of Tashkent City and Special Hospital No.1 in Zangiota. The placenta was macroscopically examined, and samples measuring approximately 1.0 x 1.0 cm, including membrane, were taken from central, paracentral, and peripheral regions. The samples were labeled and fixed in 10% formalin solution for 24 hours at 18-20°C. The next day, the samples underwent a stepwise process of washing, dehydration, embedding in histological blocks, following standard histological techniques. Sections of 5-7 microns thickness were cut from paraffin blocks using a Leica microtome (Germany). The obtained sections were stained by the classical hematoxylin-eosin method. For each sample, 6-7 fields were selected under light microscopy at magnifications of x100 and x400, and images were captured using the Image Scope program. The pathomorphological results were processed using Microsoft Excel and Statistica 6.0 software. Morphological parameters’ correlations were determined by Spearman’s rank correlation coefficient. Differences between samples were evaluated using the Kruskal-Wallis test. Main tendencies and quantitative characteristics were described using mean “M”, standard error “m”, median, and interquartile ranges depending on data distribution.
3. Results
- For pregnant women with ARVI (n=6), herpes (n=4), and viral hepatitis (n=5), the highest age range was 25-35 years, and the lowest was 40-45 years. The gestational age mostly ranged between 30-35 weeks, with some cases at 35-40 weeks. Pathomorphological changes observed included perivillous and subchorionic fibrin foci (35%), vascularization of large villi, atherosis, and microthrombosis (25-30%), infarction of villi (9-10%), inflammatory infiltrate in the subchorionic space, persistent ductus arteriosus (15%), fibrinoid necrosis (10%) (Figure 1), angiomatous changes and congestion in stem villi, hypertrophy of arteriolar walls (8-9%), and immature villi (5%) (Figure 2).Pathomorphological changes in the placentas of pregnant women with a history of herpes virus
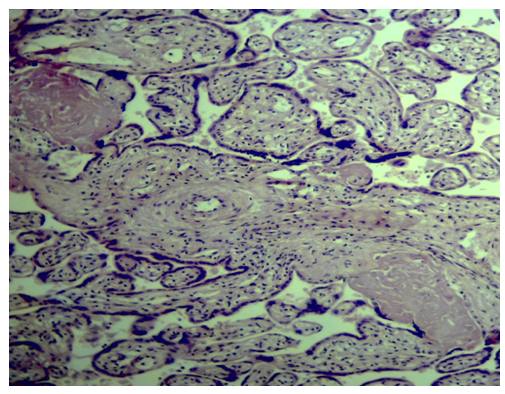 | Figure 1. Hematoxylin-eosin stain. Objective 10x, eyepiece 10x. Fibrinoid necrosis in the intervillous space between placental stem villi and villi. Angiomatosis in the terminal villi |
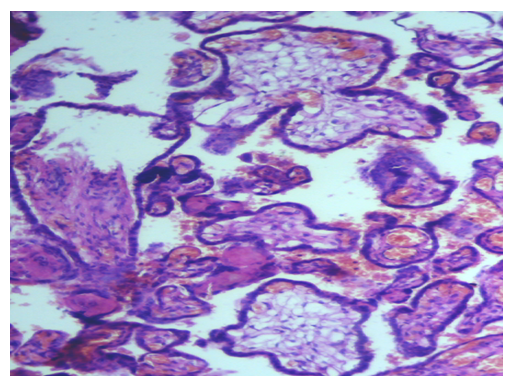 | Figure 2. Hematoxylin-eosin stain. Objective 10x, eyepiece 10x. Fibrinoid and erythrocyte diapedesis in the intervillous space between placental terminal villi and villi. Angiomatosis in small terminal villi, along with immature chorionic villi |
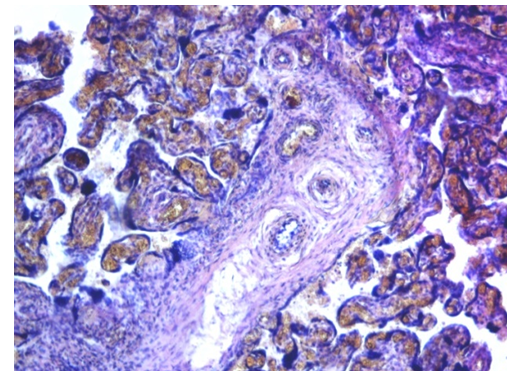 | Figure 3. Hematoxylin–eosin stain. Objective 10x, eyepiece 10x. Arteriopathy of placental stem villi and obliteration of blood vessels; angiomatosis of terminal villi |
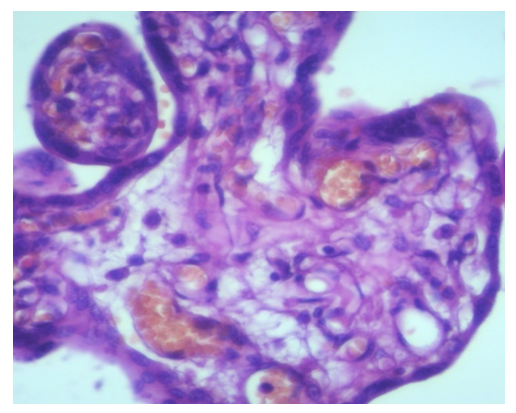 | Figure 4. Hematoxylin–eosin stain. Objective 10x, eyepiece 10x. Angiomatosis of placental terminal villi; developing fibrosis between the syncytiotrophoblast and blood vessels |
4. Conclusions
- - Among pregnant women infected with various infectious diseases, the age distribution showed that coronavirus infection was proportionally spread across age groups. In terms of gestational age, the most common infections occurred between 30 and 40 weeks of pregnancy.- The main structural changes in the placenta included: perivillous and subchorionic fibrin deposits, vascularization of chorionic villi, atherosis and microthrombosis, hypertrophy of arteriole walls, an increase in the number of immature intermediate villi, and vascularization of both stem and terminal villi. These placental changes associated with coronavirus infection indicate early onset of involutional processes in the placenta.