-
Paper Information
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3349-3353
doi:10.5923/j.ajmms.20251510.15
Received: Apr. 30, 2025; Accepted: May 20, 2025; Published: Oct. 13, 2025

Optimization of Therapeutic Nutrition for Patients with Chronic Gastrointestinal Diseases in Hot Climate Regions: A Cross-Sectional Study in Surkhandarya, Uzbekistan
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShaykhova Guli Islamovna1, Shoymardonov Bakhtiyor Kholnazarovich2, Avezova Guloyim Sattarovna3
1Head of the Department of Pediatrics, Adolescent Medicine, and Nutrition Hygiene at the Tashkent Medical Academy, Doctor of Medical Sciences, Professor Tashkent, Uzbekistan
2Assistant at the Department of Microbiology, Public Health, Hygiene, and Management of the Termez Branch of the Tashkent Medical Academy Tashkent, Uzbekistan
3Department of Propaedeutics of Children’s Diseases, Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Avezova Guloyim Sattarovna, Department of Propaedeutics of Children’s Diseases, Tashkent Medical Academy, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Objective: This research focused on evaluating the nutritional habits and shortcomings in patients with chronic gastrointestinal illnesses (CGIDs) living under the high-temperature conditions of Surkhandarya, Uzbekistan. The aim was to design a dietary intervention that accommodates local traditions, seasonal availability, and cultural acceptability. Methods: From January 2022 through December 2023, a survey was carried out on 330 individuals suffering from ailments like chronic gastritis, duodenitis, peptic ulcers, and gallbladder disorders. A 24-hour dietary recall method was used repeatedly throughout all four seasons. Nutritional intake was compared to national dietary guidelines and the Recommended Dietary Allowances (RDA). Quality of life assessments utilized the SF-36 questionnaire. Results: Most patients showed inadequate consumption of calories, proteins, vitamin C, calcium, fiber, and fluids. Their average daily energy intake was 1750 kcal, and protein intake was 58 grams both notably under the RDA. Although seasonal food variety slightly improved diets, deficiencies persisted. Inadequate water intake and high sodium consumption were common. Patients with better nutritional scores reported higher SF-36 health outcomes. Conclusion: Individuals with CGIDs in warm climates are prone to nutritional deficits that negatively impact their well-being. There’s a pressing need for cost-effective, season-sensitive diet plans tailored to the regional lifestyle. The study introduces a model approach to improving gastrointestinal health through localized nutritional strategies.
Keywords: Chronic gastrointestinal diseases, Clinical nutrition, Hot climate challenges, Dietary insufficiencies, Seasonal adaptation, Uzbekistan health, SF-36 metrics, Public nutrition strategy
Cite this paper: Shaykhova Guli Islamovna, Shoymardonov Bakhtiyor Kholnazarovich, Avezova Guloyim Sattarovna, Optimization of Therapeutic Nutrition for Patients with Chronic Gastrointestinal Diseases in Hot Climate Regions: A Cross-Sectional Study in Surkhandarya, Uzbekistan, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3349-3353. doi: 10.5923/j.ajmms.20251510.15.
1. Introduction
- Chronic gastrointestinal diseases (CGIDs) are widespread non-communicable conditions that deeply affect individuals’ daily functioning and overall life satisfaction. In regions with high temperatures, like Surkhandarya in Uzbekistan, these illnesses are more problematic due to the combined impacts of environmental, nutritional, and social factors [12]. The development and course of diseases like chronic gastritis, duodenitis, and peptic ulcers are particularly influenced by dietary habits and climate conditions.A wide range of epidemiological research indicates that poor nutrition is a leading contributor to the emergence and worsening of CGIDs [5,6,7]. Inadequate intake of vital nutrients—especially protein, vitamins C and A, calcium, and iron—is associated with weakened mucosal integrity, higher vulnerability to Helicobacter pylori infection, and slower tissue repair. Additionally, the availability of food and hydration practices fluctuate with the seasons in hot areas, which can trigger more frequent or severe disease episodes [2,3,4].Although the significance of diet in maintaining gastrointestinal health is widely acknowledged, there remains a scarcity of data on the actual dietary habits of CGID patients in Uzbekistan, especially in areas facing extreme weather changes. This lack of tailored dietary advice has resulted in broad, unspecialized nutritional guidance. Considering the variety in regional food traditions, there’s a strong need to establish therapeutic diets that are both adaptable and seasonally aligned.This research aims to analyze the everyday dietary patterns of CGID patients living in hot climates and to formulate a refined dietary model that reflects their cultural food preferences, seasonal changes, and medical requirements. These insights are intended to enhance both clinical practices and broader public health nutrition strategies across the region.
2. Materials and Methods
- The research was carried out between January 2022 and December 2023 in the Surkhandarya region, targeting adult patients diagnosed with chronic gastrointestinal disorders (CGIDs), such as chronic gastritis, duodenitis, peptic ulcers, and gallbladder dysfunction. Participants were selected through purposive sampling from outpatient services and gastroenterology units within regional medical centers. Eligible participants were over 18 years of age, had a CGID diagnosis confirmed via endoscopy or ultrasound, and provided informed consent for participation in the dietary study.A mixed-methods design was employed to collect data, combining structured interviews with detailed quantitative assessments of nutritional intake. Participants' actual food consumption was documented using a seasonally segmented 24-hour dietary recall method, applied repeatedly across all four seasons—winter, spring, summer, and autumn. Food intake for each month was recorded over ten days: three at the beginning, four in the middle, and three at the end. This schedule ensured a comprehensive reflection of regular eating patterns.Nutrient composition was determined based on standardized national food composition tables. These were then compared with Recommended Dietary Allowances (RDA) approved by Uzbekistan’s Ministry of Health (Order No. 0007-20, 2020) [11]. The analysis specifically focused on daily intake levels of calories, proteins, fats, carbohydrates, dietary fiber, water, vitamins A and C, iron, calcium, and sodium.Dietary adequacy was evaluated by calculating the percentage of nutritional requirements fulfilled for each nutrient. Both deficiencies and surpluses were classified according to World Health Organization (WHO) nutritional standards. Additionally, information on eating frequency, portion sizes, food preparation techniques, and the use of enriched or traditional foods was gathered.To assess participants’ quality of life, the SF-36 health survey was administered, evaluating domains such as physical functioning, general health, vitality, emotional wellness, and social interactions. These scores were then compared with those from a control group of healthy individuals matched for age and gender, allowing for analysis of the relationship between nutrition quality and perceived health. All statistical analyses were performed using Microsoft Excel 2019. Descriptive statistics were used to summarize the nutritional intake data, and t-tests were conducted to determine significant seasonal and demographic differences, with statistical significance set at p<0.05. Ethical approval was granted by the Institutional Bioethics Committee of the Tashkent Medical Academy, Termiz Branch. All participants signed informed consent prior to their involvement in the study.
3. Results
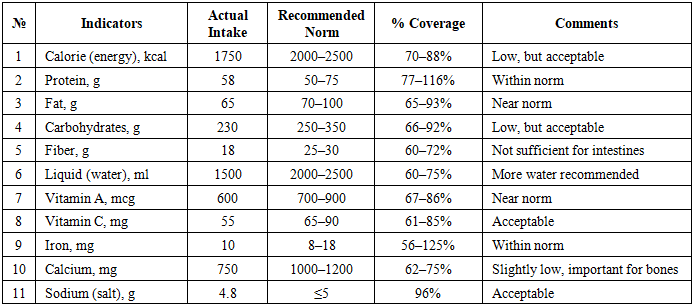
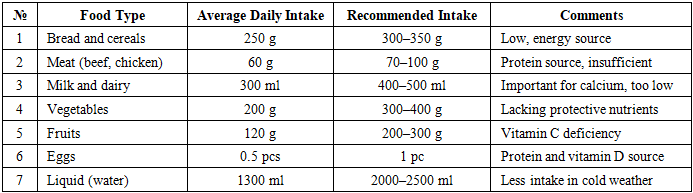
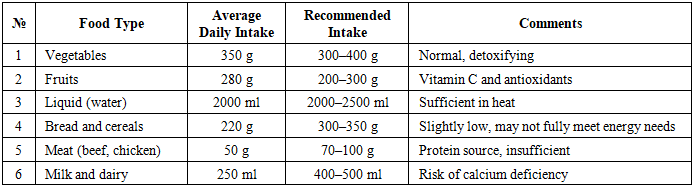
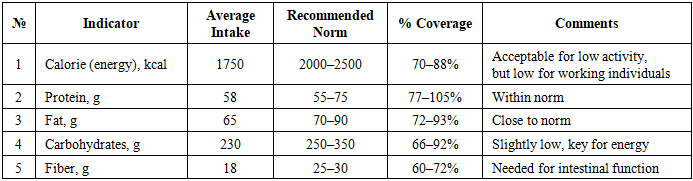
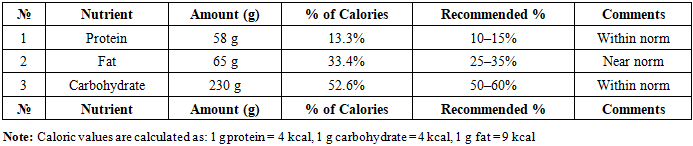
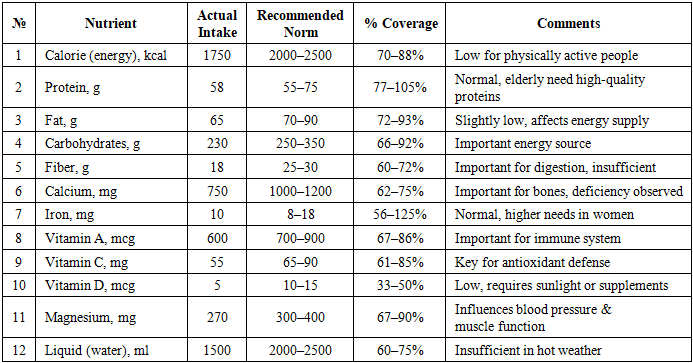
- The study included 330 confirmed CGID patients, with 58% being women and 42% men, ranging in age from 21 to 74 years. Analysis of the seasonal food consumption data revealed a consistent shortfall in caloric intake, protein, dietary fiber, calcium, and vitamin C across various age and gender groups.On average, participants consumed 1750 kcal per day, representing roughly 70–88% of the recommended dietary amount. Protein consumption averaged 58 grams daily, with 67% of individuals not meeting the standard requirements. Nutritional gaps were more significant among women and patients over 50. Additionally, carbohydrate and fat consumption leaned heavily toward refined foods, lacking both fiber and complex carbs. The analysis revealed the following: calorie deficiency or excess intake, protein deficiency, vitamin or mineral deficiency, excessive fat and sugar consumption. Patients often have deficiencies in energy, protein, and vitamins (table 1). To support recovery, it is recommended to design a proper diet, increase meal frequency, and raise fluid intake.
|
|
|
|
|
|
4. Discussion
- The outcomes of this research clearly illustrate the connection between inadequate dietary intake and poorer health conditions in individuals living with chronic gastrointestinal diseases (CGIDs) in high-temperature environments. The widespread lack of energy, protein, calcium, vitamin C, and water intake among the majority of patients points to serious nutritional deficiencies that could intensify the progression of gastrointestinal disorders and slow down recovery [7,8,9,13,14].The hot weather in Surkhandarya adds to the problem through increased fluid loss, heightened metabolic needs, and decreased appetite—all of which contribute to malnutrition among CGID patients. Compounding this issue, the seasonal availability of fresh foods, particularly in winter and early spring, restricts nutritional intake further. These challenges emphasize the necessity for continuous access to affordable and nutrient-rich foods throughout the year.Regular observations of low fiber consumption alongside high sodium intake suggest a diet overly dependent on processed grains and salty foods. Such habits can disrupt gut motility, damage the balance of intestinal microbiota, and elevate the risks of hypertension and metabolic complications. Therefore, nutrition education promoting varied diets and reduced salt usage is critically important for this population.Additionally, the positive link between adequate nutrition and improved SF-36 quality of life scores underlines the comprehensive impact that proper diet has on both physical and psychological well-being. Patients who received enough essential nutrients experienced significantly greater physical ability and overall life satisfaction. This supports the integration of personalized dietary guidance into standard CGID treatment, especially in outpatient and primary care settings.Comparable studies from other warm climate regions, including rural India and sub-Saharan Africa, have similarly pointed out the importance of diet modification in managing gastrointestinal illnesses. These current findings are consistent with global data and strengthen the argument for localized dietary plans that consider environmental, social, and economic realities.
5. Conclusions
- The research highlighted significant nutritional shortfalls in caloric and essential nutrient intake among individuals suffering from chronic gastrointestinal diseases in the hot-climate region of Surkhandarya, Uzbekistan. Most participants consumed less than the advised amounts of energy, protein, vitamin C, calcium, fiber, and water. These dietary insufficiencies were found to be linked with a decline in quality of life and possibly contributed to worsening disease conditions.To address these issues, the following measures are proposed:Design and distribution of seasonal therapeutic meal plans that incorporate culturally accepted and locally accessible foods.Launch of public health initiatives aimed at promoting proper hydration and reducing high salt consumption.Incorporation of personalized nutritional assessments and dietary counseling into standard treatment protocols for CGID patients.Support for year-round availability of fresh produce through community gardening projects or food support services.Improving nutritional intake in hot climate regions is more than just treating disease—it forms the basis of proactive health management and long-term wellness. This study lays the groundwork for policy reforms, clinical advancements, and future research focused on refining therapeutic nutrition in environmentally demanding areas.