-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3345-3348
doi:10.5923/j.ajmms.20251510.14
Received: May 3, 2025; Accepted: Jun. 2, 2025; Published: Oct. 11, 2025

Surgical Correction of Ventral Hernias in Patients with Morbid Obesity
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbduraxmanov Diyor Shukurullayevich, Esirgapov Sardor Nursalimovich
Samarkand State Medical University, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This paper presents the results of a clinical substantiation for a combined approach to treating patients with ventral hernias and morbid obesity. The implementation of a preoperative preparation algorithm, including adaptation of intra-abdominal pressure, and advanced hernioplasty and abdominoplasty techniques has significantly reduced the incidence of postoperative complications, improved functional and aesthetic outcomes, and enhanced patients' quality of life. Special attention was given to the combination of onlay+sublay and abdominoplasty methods, which ensured reliable repair of the hernia defect and minimized the risk of recurrence.
Keywords: Ventral hernias, Morbid obesity, Hernioplasty, Abdominoplasty, Preoperative preparation
Cite this paper: Abduraxmanov Diyor Shukurullayevich, Esirgapov Sardor Nursalimovich, Surgical Correction of Ventral Hernias in Patients with Morbid Obesity, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3345-3348. doi: 10.5923/j.ajmms.20251510.14.
Article Outline
1. Relevance of the Topic
- Morbid obesity is one of the key factors that worsen the prognosis and increase the frequency of postoperative complications in patients suffering from ventral hernias [1]. According to the World Health Organization (WHO), morbid obesity is a disease characterized by a body mass index (BMI) ≥ 40 kg/m2, and its prevalence continues to increase worldwide [2]. In patients with obesity, the likelihood of developing various complications, such as infectious diseases, thromboembolic disorders, and respiratory failure, increases significantly [3]. Additionally, the healing process of postoperative wounds is impaired. These features create difficulties both in diagnosis and in choosing the optimal surgical approach for ventral hernia correction [4].Ventral hernias, including both primary and recurrent abdominal wall defects, represent a common problem in surgical practice [5]. According to modern research, ventral hernias account for about 20% of all abdominal wall hernias, and among patients with obesity, this figure increases significantly [6]. At the same time, traditional open surgical interventions in this group of patients are associated with an increased risk of complications such as wound infection, impaired tissue healing, hernia recurrence, and a prolonged recovery period [7].In recent years, laparoscopic hernioplasty techniques have established themselves as a safe and effective alternative to traditional open interventions, ensuring minimal tissue trauma, rapid recovery, reduced pain syndrome, and shorter hospital stays [8]. However, when treating patients with morbid obesity, laparoscopic surgery also faces a number of challenges, such as technical difficulties due to excess adipose tissue, which requires additional consideration in choosing implant fixation methods and intervention strategies [9].Thus, despite significant advancements in ventral hernia surgery, the need to optimize surgical approaches for patients with morbid obesity remains a pressing issue. Further research is needed to improve surgical treatment techniques, reduce the risk of postoperative complications, and enhance the effectiveness of surgical correction in this category of patients [10].
2. Materials and Methods of Research
- The study is based on the results of examination and treatment of 121 patients with ventral hernias and morbid obesity who underwent surgery in the surgical department of the 1st clinic of Samarkand State Medical University between 2015 and 2024. All patients underwent planned surgery, and depending on the chosen treatment approach, the patients were divided into two groups. The first group, the comparison group, consisted of 54 patients with ventral hernias and morbid obesity who underwent hernioplasty alone. The second, main group consisted of 67 patients who underwent hernioplasty combined with abdominoplasty.Of the 121 patients, 37 (30.6%) were men and 84 (69.4%) were women. Age distribution: up to 45 years - 22 (18.2%), 46-59 years - 67 (55.4%), 60-74 years - 29 (23.9%), 75-80 years - 3 (2.5%).All patients underwent anthropometry to determine their body weight. All patients had morbid obesity - alimentary in nature, due to dietary habits, combined with low physical activity. Excess body weight was assessed according to the WHO experts' classification. Patients were classified according to the A. Matarasso (1989) classification based on the degree of anterior abdominal wall ptosis. Minimal and moderate ptosis (I-II degree) was observed in 34 and 42 patients with obesity of the III-IV degree, respectively, in the studied groups. Moderate and severe ptosis (III-IV degree) was observed in 20 and 25 patients with III-IV degree obesity.Out of 121 patients with ventral hernias and morbid obesity, 90 (74.4%) had comorbid diseases. Among these, 49 patients had 1 additional pathology, 29 had 2, and 12 had 3 concomitant diseases of other organs and systems. Among comorbidities, cardiovascular diseases were the most common, occurring in 82.6% of cases, followed by respiratory system pathology in 9 (7.4%) patients, varicose veins of the lower extremities in 20 (16.5%) patients, and diabetes mellitus in 32 (26.4%) patients.According to the classification by Chervel J.P. and Rath A.M. (1999), the vast majority of patients (85 - 70.2%) had supraumbilical (M1) and periumbilical (M2) hernias. The lowest number of patients had lateral (L) 9 (7.4%) and combined (M+L) 3 (2.5%) ventral hernias. 46 (38.0%) patients had large (W3) and giant (W4) hernias. Out of 121 patients, 40 (33.0%) had primary ventral hernias, 50 (41.3%) had postoperative ventral hernias (R0), and 31 (25.6%) had recurrent ventral hernias (Rn).Among the instrumental research methods, computed tomography hernia abdominometry (CTHA) performed on 58 patients in the main group proved to be the most informative. CTHA made it possible to identify defects in the topography of the anterior abdominal wall, determine the relative volume of the hernia in relation to the abdominal cavity volume, plan adequate preoperative preparation, and choose the optimal method of repair. According to our studies, with a relative volume of the hernial protrusion up to 14.0% of the abdominal cavity volume, it is possible to use tension methods of hernioalloplasty - implantation of an "onlay" endoprosthesis with suturing of the defect.With a volume greater than 14.1%, preference was given to tension-free repair methods. In 46 (68.6%) patients of the main group with ventral hernias and morbid obesity at the preoperative stage, we conducted adaptive training to increase intra-abdominal pressure using the proposed improved pneumatic belt-bandage. The use of this technique in patients with ventral hernias W3-W4 and morbid obesity allowed for a reduction in the risk of developing compartment syndrome.In the comparison group (n=54), hernioalloplasty was performed using tension methods in 37 (68.5%) patients and tension-free methods in 17 (31.5%) patients.In the main group, the choice of hernia alloplasty was differentiated and supplemented with abdominoplasty according to our proposed program (certificate of state registration of the computer program No. DGU 10983, Intellectual Property Agency of the Republic of Uzbekistan - 2021). The patients in the main group were divided into 4 subgroups based on the program results.Patients in the 1st subgroup with a total score of up to 5, as well as with a hernia protrusion volume of up to 14% of the abdominal cavity volume according to CT hernia abdominometry data, underwent "onlay" mesh implantation with suturing of the hernia defect. This group consisted of 24 (35.8%) patients with morbid obesity and grade III-IV abdominoptosis, for whom hernia alloplasty was supplemented with abdominoplasty.In the 2nd subgroup, with a score of 6 to 10 and taking into account CT hernia abdominometry data showing a hernial protrusion volume greater than 14.1% of the abdominal cavity volume, we performed tension-free repair. To increase the volume of the abdominal cavity and prevent the development of abdominal compartment syndrome, after delimiting the abdominal cavity with a flap of the hernia sac, abdominal wall repair was performed by placing a mesh on the aponeurosis without suturing it. Mesh fixation was carried out using pre-placed U-shaped sutures encompassing all layers of the musculo-aponeurotic wall up to the peritoneum.In 12 (17.9%) patients of the 3rd subgroup of the main group with hernia defect sizes greater than 10 cm and hernia protrusion volumes exceeding 18% of the abdominal cavity volume, as determined by CT hernioabdominometry, a combined tension-free hernioplasty "onlay + sublay" was performed. This involved placing one implant behind the musculoaponeurotic layer after delimiting the abdominal cavity with a flap of the hernia sac, and positioning the second implant above the aponeurosis (Fig. 1).
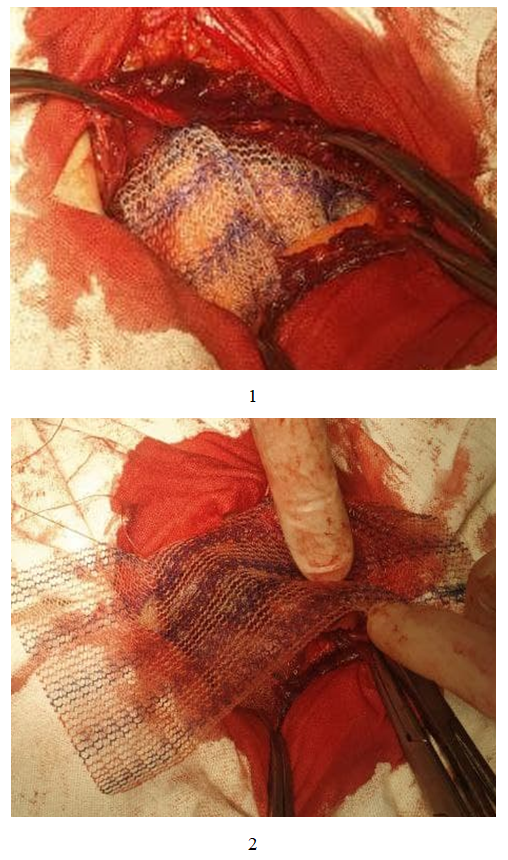 | Figure 1. Stages of endoprosthesis fixation"sublay" (1) and "onlay" (2) using pre-placed U-shaped sutures |
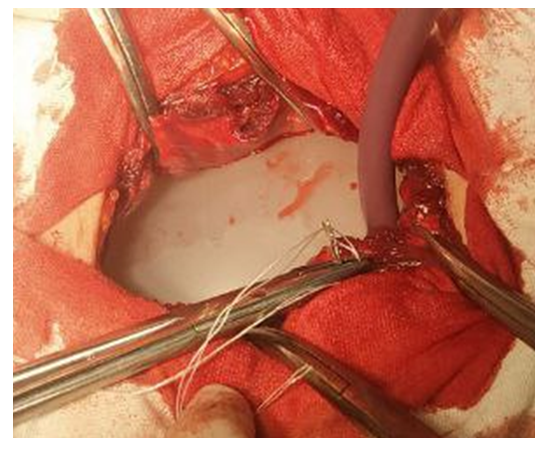 | Figure 2. Pneumatic device for preventing intraoperative injuries to abdominal organs |
3. Research Results
- It should be noted that on average, each patient in the comparison group had 2-3 complications in the form of a combination of bronchopulmonary or (and) cardiovascular complications with wound complications. Overall, in the comparison group, there were 8 (14.8% of 54) patients with various complications, of which 6 (11.1%) had wound complications and 4 (7.4%) had general extra-abdominal complications. In the main group, 6 (8.9% of 67) patients had various complications, 3 (4.5%) had wound complications, and another 3 (4.5%) had general complications. In terms of the comparative feature regarding the number of complications, a significant improvement was obtained in the main group (Criterion χ2 =4.043; Df=1; p=0.045).Furthermore, long-term results were analyzed in 93 (76.8%) of the 121 operated patients, with ventral hernia recurrence observed in 5 (12.5%) patients in the comparison group. It was determined that the main cause of hernia recurrence was the retention of a significant skin-fat apron after hernioalloplasty, which, due to intra-abdominal pressure and gravitational force, shifts the implant downward, exposing weak points of the abdominal wall in the upper part of the prosthesis. Additionally, wound suppuration with implant rejection in patients with pronounced grade III-IV abdominoptosis contributed to recurrence. Improvement of technical aspects in performing tension-free hernioalloplasty methods with endoprosthesis implantation using the combined "onlay+sublay" technique in conjunction with abdominoplasty allowed for the elimination of disease recurrence.All patients who underwent abdominoplasty achieved a positive aesthetic effect, as they were freed from the skin-subcutaneous fold, resulting in a flat and taut abdomen. The suture line runs along the line connecting the iliac spine processes and is practically invisible. All patients were satisfied with the achieved aesthetic result.In terms of functional effect, due to the optimal preoperative preparation scheme and abdominoplasty, improvement in external respiration indicators was observed, and cardiovascular complications were minimized. Spirometry indicators improved compared to pre- and post-operative measurements, i.e., a steady increase in respiratory volume and vital lung capacity was noted in all patients.According to the developed program for assessing patients' quality of life, 87 (93.5%) out of 93 patients observed in the long-term postoperative period were evaluated. Of these, 36 patients were from the comparison group and 51 patients from the main group. In the comparison group, excellent results were obtained in 11 (30.5%) patients, good in 17 (47.2%), satisfactory in 5 (13.9%) patients, and unsatisfactory in 3 (8.3%) cases. In the main group, excellent results were obtained in 28 out of 51 (54.9%) patients, good in 19 (37.2%), satisfactory in 3 (5.9%) patients, and unsatisfactory in only 1 (1.9%) case.
4. Conclusions
- 1. Computed tomographic hernioabdominometry allows for the detection of defects in the topography of the anterior abdominal wall, determination of the relative volume of the hernia to the abdominal cavity volume, planning of adequate preoperative preparation, and selection of the optimal method of plastic surgery.2. Preoperative adaptation of intra-abdominal pressure using a pneumatic bandage in patients with ventral hernias W3-W4 and morbid obesity allows for a reduction in the risk of developing compartment syndrome and a decrease in the frequency of postoperative extra-abdominal complications from 7.4% to 4.5%.3. Improvement of the technical aspects of performing tension-free hernioplasty methods with endoprosthesis implantation using the combined "onlay+sublay" technique in combination with abdominoplasty has eliminated disease recurrence (in the comparison group, recurrence was 12.5%).4. The proposed algorithm for adequate preoperative preparation and selection of the hernioplasty and abdominoplasty method in patients with abdominal hernias and abdominoptosis has reduced the frequency of postoperative complications from 14.8% to 8.9% (p=0.045), including wound complications from 11.5% to 4.5%.5. Combining hernioplasty with abdominoplasty in patients with ventral hernias and morbid obesity with grade III-IV abdominoptosis significantly improved the aesthetic and functional state of patients, enhanced quality of life with an increase in the proportion of excellent and good long-term results from 77.7% to 92.1%, and decreased unsatisfactory outcomes from 8.3% to 1.9% (p=0.030).