-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3336-3340
doi:10.5923/j.ajmms.20251510.12
Received: Aug. 21, 2025; Accepted: Sep. 19, 2025; Published: Oct. 11, 2025

Comprehensive Measures to Treat and Prevent Dead-End Diseases in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSattarov J. B.1, Khaidarov N. S.2
1Tashkent Pediatric Medical Institute, Uzbekistan
2Fergana Medical Institute of Public Health, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article provides detailed information on current methods of clutch diagnosis in childhood. A brief description of the methods of ultrasound, and radiopaque examination is given, as well as the possibilities of using spiral computed tomography in the connective genesis of the intestine are considered. Methods of conservative and surgical treatment of the clutch are described in detail.
Keywords: In children, Clutch disease, Diagnosis, Treatment
Cite this paper: Sattarov J. B., Khaidarov N. S., Comprehensive Measures to Treat and Prevent Dead-End Diseases in Children, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3336-3340. doi: 10.5923/j.ajmms.20251510.12.
Article Outline
1. Relevance
- Due to the constant increase in the number and volume of surgical interventions performed on the abdominal areas, the value of the concomitant process also increases [3,12]. From this point of view, we consider it expedient to take actions aimed at improving diagnostic methods, as well as to develop new methods that will help to identify concomitant intestinal capture as soon as possible [6-7]. In recent years, thanks to scientific and technological progress, a large group of new technologies for radiation diagnostics, such as ultratavush, MRI, CT, and others, has become widely used in practice. Radiological methods of examination of the gastrointestinal tract are the most frequently used research methods [5-6,13]. However, even in stationary conditions, diagnostic errors are 16-34% [1,4,9]. Ultrasound diagnosis, when identifying the accompanying intestinal tract, is a good additional method. However, the cause of obstruction with ultrasound can be established extremely rarely, so this method does not replace CT when examining patients with suspected obstruction [6,12]. Patients undergoing surgery for acute adhesion intestinal obstruction (AAIO) have a much higher risk of repeated surgery compared to laparotomy for acute intestinal obstruction of a different etiology [2,10]. Mortality from complications of adhesive disease (CD) (acute adhesive and suffocating intestinal cramps) has persisted for many years, according to researchers, at the level of 16-21% [7-8], and according to some foreign data reaches 26.5% and has no downward trend [8]. The frequency of complications occurring in early and late intestinal attacks ranges from 12 to 64% [6-7].Conservative treatment of concomitant disease is ineffective [1], and its recurrence after surgical interventions is 32-71% [13]. The literature shows that after endoscopic interventions in the abdominal cavity, fibrous-dystrophic changes develop in the abdominal cavity, which, in turn, require repeated endoscopic or anal intervention. In addition, many acute surgical diseases complicated by abdominal infection (which are the main cause of the development of complications in the abdominal cavity) today require conventional surgical treatment [3,7-8]. Despite numerous experimental studies and clinical studies, effective methods for the prevention of comorbidities developing after surgery have not yet been developed [11,12]. The purpose of the study: to improve the results of treatment and optimize measures to prevent concomitant diseases of the abdominal organs in children.
2. Research Materials and Methods
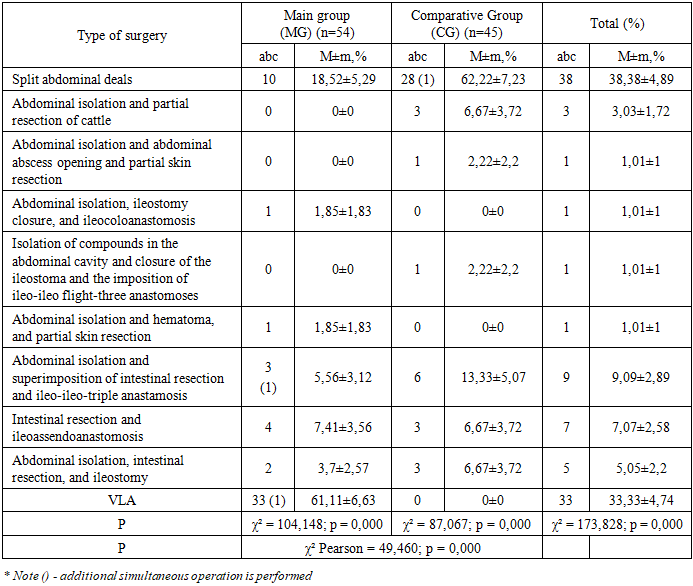
- During 2018-2023, the results of the treatment of 2681 patients with acute surgical diseases of the abdominal cavity were studied. The results of the treatment of 231 (8.6%) patients with complications of concomitant disease (СD) in the abdominal cavity after surgery were also examined and analyzed. The age of patients is from 3 months to 18 years, of which 94 are girls (40.69%) and 137 are boys (59.31%). All examined patients were divided into two groups: Comparative group (CG) – 97 patients (42%) (2018-2020). They used the usual treatment tactics. If conservative treatment failed, an emergency laparotomy was performed to cut and separate the compounds. Main group (MG) – 134 patients (58%) (2021-2023). In this group, therapeutic and preventive measures were carried out based on the algorithm and methodology developed in the clinic. Adhesiolysis is performed by the traditional (laparotomic) or videolaparoscopic method. Also, for the prevention of concomitant disease (СD), barrier agents were used - vobenzyme, longidase, and drugs against “Mesogel.” Of the 54 patients in the main group, 33 (61.1%) underwent early programmable video laparoscopic operations.When children with concomitant diseases (СD) were hospitalized in the surgical department, the following examinations were carried out: general examination, physical examination, gastric tube decompression, abdominal and chest X-rays, Ultrasound examination, laboratory tests of blood and urine, and monitoring of acid-base state. This inspection program was applied to all children.
3. Study Results and Discussion
- According to the results of the study, 99 (42.9%) patients had acute, 97 (42.0%) - chronic, and 35 (15.1%) - chronically recurrent. According to the information received, relatively digital radiography to identify concomitant diseases in children, ultrasound of the abdominal cavity, gastrointestinal tract, MCT (Multimodal computed tomography), and the effectiveness of CT (Computed tomography) methods and Doppler imaging of intestinal blood vessels were also calculated (Tables 1,2). The highest rates of concomitant disease (CD) were noted in MCT and CT (83.33% and 80.00%, respectively). When diagnosing the acute intestinal tract, the MCT and CT showed the greatest accuracy (92.31% and 84.62%, respectively). Ultrasound examination of abdominal organs (65.15% and 86.00%, respectively) in the case of articular disease and acute articular intestinal obstruction. Barium passage along the gastrointestinal tract in the ratio of concomitant diseases and acute intestinal obstruction (77.78% and 81.82%, respectively). At the same time, intestinal vascular dopplerography was the most ineffective in detecting adhesion (40.00%, respectively). The main method of diagnosing these diseases is MCT, which showed 83.33% of cases.
|

|

|
|
|
|
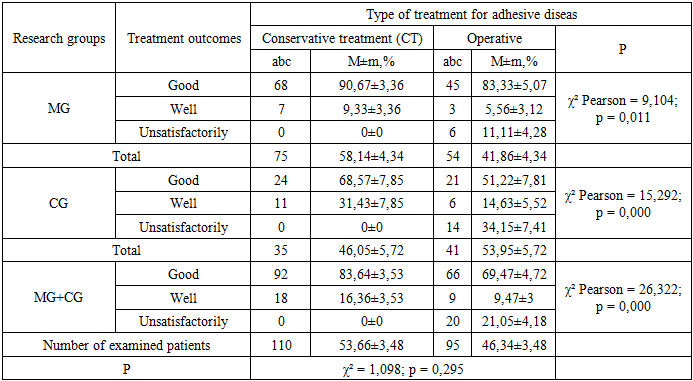
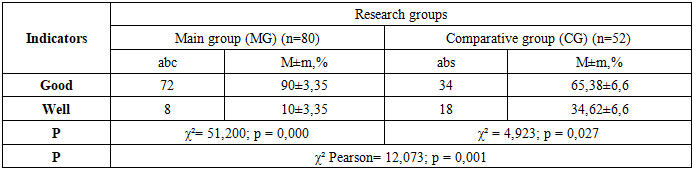
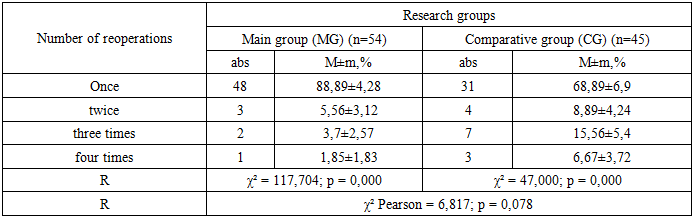
4. Conclusions
- Adhesive disease accounts for 8.6% of acute surgical pathologies of the abdominal cavity in children, developing based on anatomical and functional changes. It manifests clinically in acute (42.9%), chronic (42%), and recurrent (15.1%) forms. These different forms are of significant importance in timely diagnosis and selecting an effective treatment strategy.According to the diagnostic algorithm developed within the study, the most informative method for diagnosing adhesive disease was Multispiral computed tomography, which provided 81.82% accuracy. It also showed high accuracy (88.46%) in diagnosing acute adhesive intestinal obstruction. Ultrasound examination of abdominal organs provided 59.85% accuracy in adhesive disease and 80.81% accuracy in acute adhesive intestinal obstruction. Barium passage analysis recorded 71.11% accuracy in adhesive disease and 78.26% accuracy in acute adhesive intestinal obstruction. Doppler ultrasound examination showed only 50% accuracy in diagnosing adhesive disease. Preventive use of “Wobenzyme”, “Longidase”, and “Mesogel”, as well as 3 annual observations using videolaparoscopic methods, showed that the quality of life in the main group improved by 8.76% (8.06% ≤ 16.82%) and relapses decreased by 20.4%. The application of the proposed treatment and tactical approaches for adhesive disease, when compared between the main and comparative groups, increased good treatment outcomes by 27.1% (from 59.9% to 87%) and decreased unsatisfactory outcomes by 23.04% (from 34.15% to 11.11%).