-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3747-3752
doi:10.5923/j.ajmms.20251510.100
Received: Oct. 2, 2025; Accepted: Oct. 26, 2025; Published: Oct. 31, 2025

The Importance of a Comprehensive Ultrasonic Examination in the Diagnosis of Adenomyosis in Women in Perimenopause
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFayzullaeva Nilufar Avazovna, Askarova Zebo Zafarjonovna
Samarkand State Medical University, Uzbekistan
Correspondence to: Fayzullaeva Nilufar Avazovna, Samarkand State Medical University, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The study included 120 perimenopausal patients. Of these, 70 patients had adenomyosis and 50 perimenopausal women without gynecological conditions, who were examined and treated in the gynecology department of the multidisciplinary clinic of Samara State Medical University from 2023 to 2025. The study also included 45 case histories of perimenopausal women with adenomyosis, which were studied retrospectively. Thus, the combination of adenomyosis and uterine fibroids was significantly more common in the study group: 28 (40±5.9%) and 9 (20±6%) in the study and comparison groups, respectively (p<0.05). When compared with histological data from excised tissue and ultrasound elastography, the diagnostic accuracy of adenomyosis using elastography was 88.6%, sensitivity 94.1%, specificity 85%, positive predictive value 80%, and negative predictive value 95.8%. These results demonstrate the high effectiveness of comprehensive ultrasound examination in women with adenomyosis in establishing a diagnosis and determining the severity of adenomyosis.
Keywords: Adenomyosis, Ultrasound elastography
Cite this paper: Fayzullaeva Nilufar Avazovna, Askarova Zebo Zafarjonovna, The Importance of a Comprehensive Ultrasonic Examination in the Diagnosis of Adenomyosis in Women in Perimenopause, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3747-3752. doi: 10.5923/j.ajmms.20251510.100.
1. Introduction
- Perimenopause marks a turning point for adenomyosis, when hormonal and immunological shifts converge to shape its trajectory. Estrogen surges, unchecked by declining progesterone, can fuel lesion growth, increasing pain and bleeding [5]. Concurrently, age-related immune changes, such as increased inflammation, can exacerbate the underlying pathology of the condition, creating a feedback loop of worsening symptoms [6,8]. This dual influence makes perimenopause a period of heightened vulnerability, when adenomyosis can transition from a manageable problem to a dominant health issue. When combined with perimenopausal issues such as sleep disturbances or anxiety, adenomyosis can trigger a profound decline in well-being. Treatment options also create dilemmas: hormonal therapy may conflict with menopausal management, while hysterectomy, although curative, carries significant physical and emotional burden [11,12]. For women at this stage of life, the lack of individualized solutions compounds their burden, highlighting the critical need for innovative strategies. Adenomyosis emerges as a multifaceted disorder intersecting gynecological, hormonal, and immunological domains. Its definition as endometrial invasion of the myometrium only superficially captures its impact, which peaks in prevalence and severity among perimenopausal women. Affecting up to 30% of women, its epidemiology reveals a widespread but underrecognized problem [1,2]. Despite its high accuracy, histological examination is inherently invasive, limiting its use to cases where surgery is already planned or where fertility preservation is not an issue. Its reliance on postoperative tissue also makes it impractical for routine diagnosis, particularly in young women or those seeking conservative treatment. However, it remains a valuable tool in research settings or when imaging results are equivocal, providing definitive confirmation that noninvasive methods tend to approach [7,9]. Transvaginal ultrasound (TVUS) has become the cornerstone of adenomyosis diagnosis due to its widespread availability, affordability, and noninvasive nature [3,10]. This imaging modality allows physicians to visualize the uterus in real time, identifying features suggestive of adenomyosis, including:• Uterine asymmetry: A spherical or unevenly enlarged uterus.• Myometrial heterogeneity: Changes in echogenicity within the myometrium.• Subendometrial streaks: Echogenic lines indicating endometrial invasion.• Cystic spaces: Small anechoic areas representing dilated glands.Studies show that the sensitivity and specificity of TVUS for adenomyosis range from 50% to 87% and 74% to 98%, respectively [4]. However, these figures are highly dependent on operator skill and equipment quality. In experienced hands, TVUS can reliably detect adenomyosis, but its accuracy is reduced when leiomyomas or other uterine abnormalities obscure the visualization field [5]. Perimenopausal women face additional challenges due to age-related uterine changes, such as increased myometrial thickness or calcifications, which can mimic features of adenomyosis [6]. Despite these limitations, TVUS remains the preferred initial approach due to its practicality and ability to guide further diagnostic steps.In recent years, studies have emerged exploring the potential of elastography in the diagnosis of adenomyosis [1–8]. V. V. Mitkov [4] used shear wave elastography, a technique independent of the degree of tissue compression by the transducer, to assess myometrial stiffness in patients with adenomyosis. The data obtained were retrospectively compared with the results of a morphological examination of the surgical specimen and hysteroscopy data with separate diagnostic curettage.
2. The Aim of the Study
- Was to evaluate the effectiveness of a comprehensive ultrasound examination in women with adenomyosis during perimenopause.In light of these goals and objectives, we examined 120 perimenopausal patients. Of these, 70 patients with adenomyosis and 50 perimenopausal women without gynecological diseases were examined and treated in the gynecology department of the multidisciplinary clinic of the Samara State Medical University from 2023 to 2025. And 45 case histories of perimenopausal women with adenomyosis were retrospectively studied and treated in the gynecology department of the multidisciplinary clinic of the Samara State Medical University from 2020 to 2022.The examined women were divided into three groups: Group 1, 70 patients with a verified diagnosis of adenomyosis.Group 2, 50 perimenopausal women without gynecological diseases.Group 3, 45 retrospectively reviewed medical records of perimenopausal women with adenomyosis. The age of those examined ranged from 45 to 52 years, with an average of 48.6±1.6 years. The following data served as inclusion criteria for the study: perimenopausal age, morphologically confirmed diagnosis of adenomyosis, absence of antibacterial therapy for the past 3 months to objectively assess the infection status, and absence of hormonal therapy for the past 3-6 months. Informed consent was a prerequisite for participation in the study.
3. Exclusion Criteria
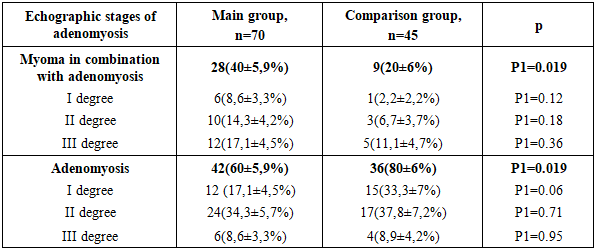
- Patients with coagulopathy and iatrogenic bleeding, as well as malignant diseases of any location, were not included in the study. Ultrasound examination of the pelvic organs was performed on days 5-7 of the menstrual cycle in patients with bleeding, and in patients with a delayed menstruation, regardless of the cycle, using the Voluson730-Expert (Japan) devices, which belong to contact scanning systems and operate in real time, with a transabdominal sensor RA 134-8-D and a transvaginal sensor RIC 6-12-D and "Aloka SSD 500" (Japan) with a transvaginal convex sensor with a frequency of 7-12 MHz. Echographically, the size, position, blood supply and structure of the cervix and body of the uterus, the presence of inclusions in the myometrium were determined, the thickness and structure of the endometrium (M-echo), the structure of the ovarian tissue, the presence and volume of fluid in the retro-uterine space were also assessed [1,4]. To make the method more objective, shear wave elastography (SWE) has recently been used. It allows for the quantitative determination of tissue stiffness (elasticity). SWE is a method for the objective quantitative determination of tissue stiffness (elasticity), characterizing the condition of the organs and tissues being examined. Quantitative indicators of the ultrasound elasticity of organs and tissues can include Young's modulus, shear (transverse) wave velocity, elasticity indices (SWE ratio), etc. It is possible to measure and express these indicators numerically as the velocity of a wave diverging from the zone of impact of a high-power acoustic pulse on the object being examined. The stiffer the object being examined, the higher the shear wave velocity. SWE technology is considered more objective and reproducible than CEG [12]. The rigidity of the myometrium in nodular and diffuse forms of its damage, in the presence of adenomyosis, benign myomatous nodes, malignant lesions, determined by elastometry data, differs significantly from that of the unchanged myometrium. The velocity of propagation of a transverse wave in the unchanged myometrium, according to the results of various researchers, can vary within the range from 1.20 to 3.63 m/s, rigidity - 5-114 kPa; in adenomyosis - 2.40-4.50 m/s, 31-180 kPa; in benign myomatous nodes - 0.92-3.97 m/s, 25-55 kPa. The sensitivity of elastometry in the diagnosis of adenomyosis is 76.9-92.2%, specificity - 71.1-88.8% [12]. Ultrasound examination and elastography of the uterus were performed at the Department of Medical Radiology of the Faculty of Postgraduate Education of the SamSU by the assistant of the department, Associate Professor A.S. Ametova.When examining the medical records of patients with adenomyosis, various types of uterine fibroids were detected sonographically in every fifth patient (9 patients, 20%) (Fig. 1). Given the high sensitivity and specificity of a comprehensive ultrasound examination, including Doppler ultrasound and ultrasound elastography, patients in the study group underwent a comprehensive ultrasound examination (Table 1). The following features were used to assign ultrasound signs to the stages of adenomyosis.
|

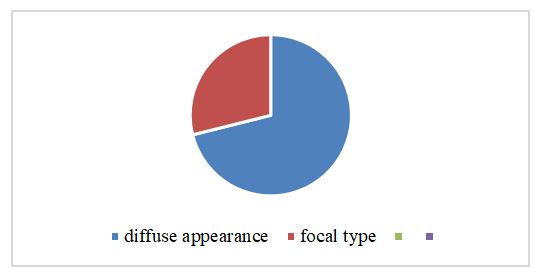 | Figure 1. Types of adenomyosis in the examined women of the comparison group (retrospective analysis) |
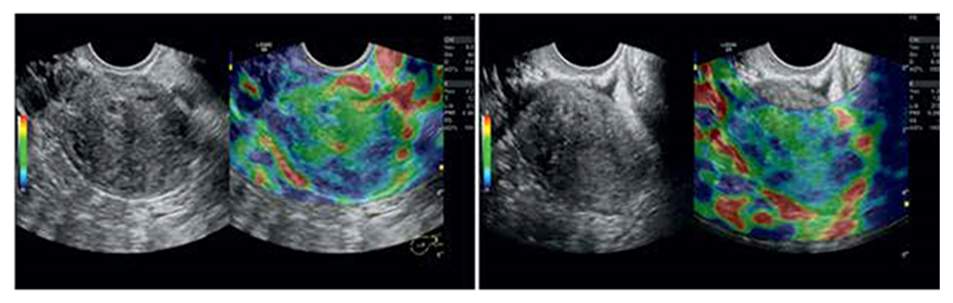 | Figure 2. Ultrasound elastography of the uterus, diffuse and nodular types of adenomyosis |
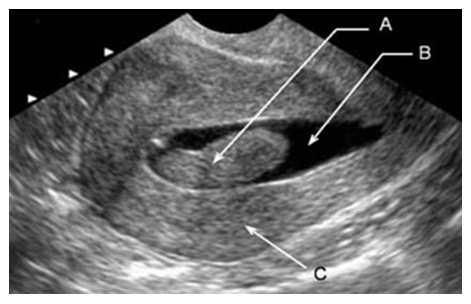
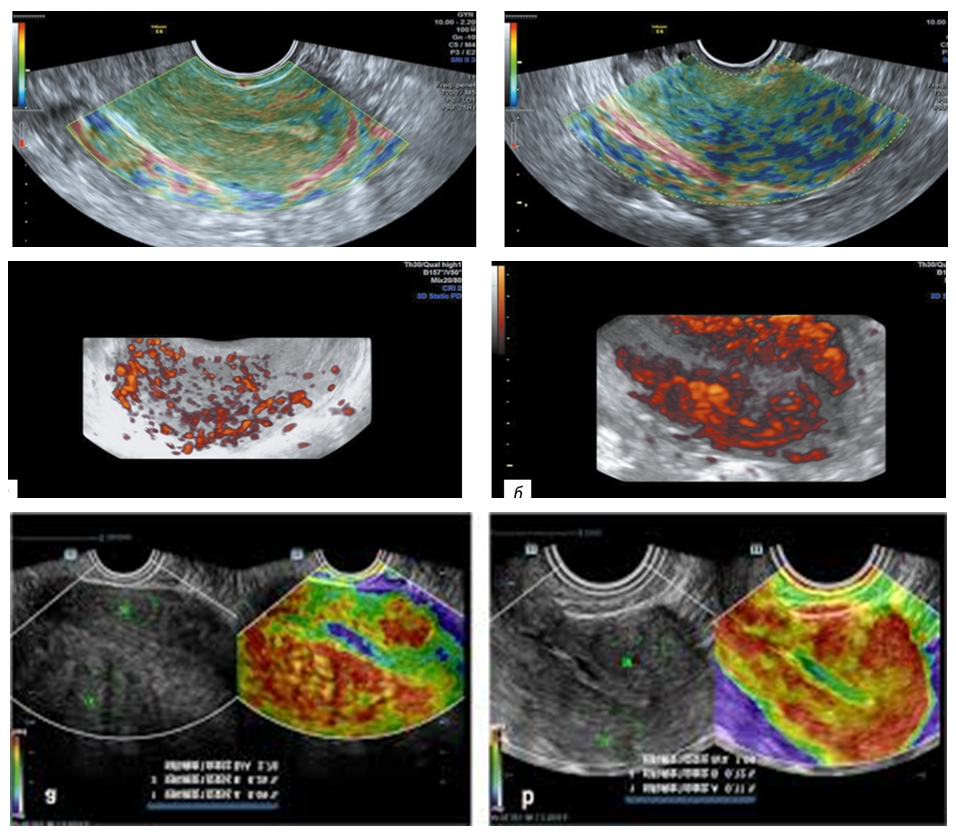 | Figure 3. Patient K-va, 49 years old, file number 5453. Ultrasound image of diffuse adenomyosis |
|
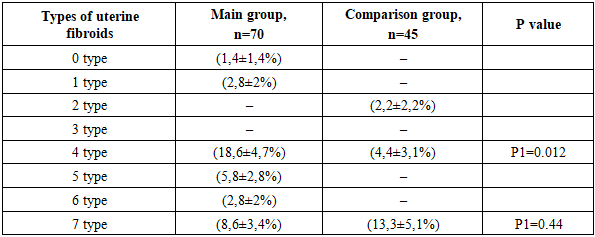
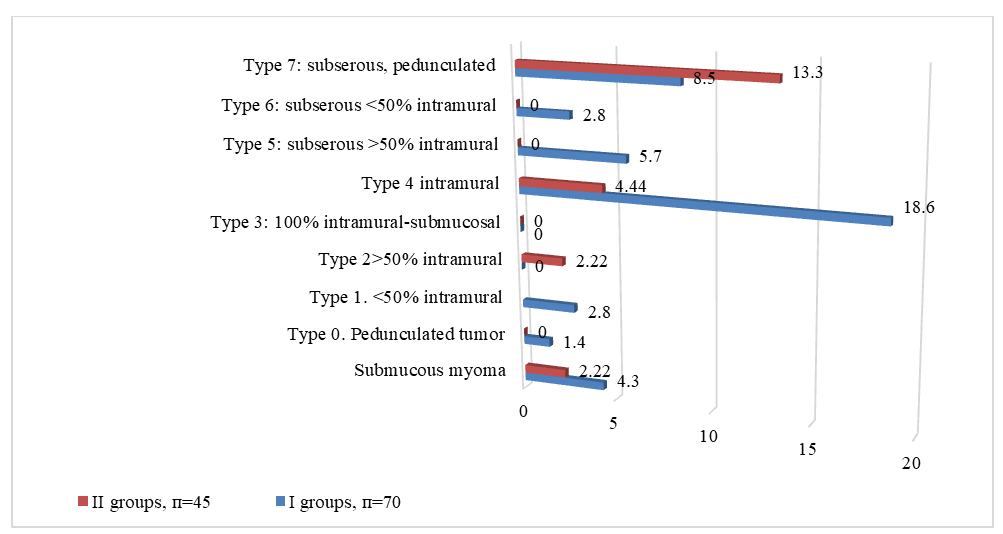 | Figure 4. Distribution of patients with fibroids according to the FIGO classification |
 | Figure 5. Patient Kh-va, 49 years old. Source No. 878. Ultrasound image of a submucous node and grade I adenomyosis |
 | Figure 6. Patient Kh-va, 49 years old, Record No. 879. Ultrasound revealed a submucous fibroid |
|
4. Conclusions
- Thus, the combination of adenomyosis and uterine myoma was significantly more common in the study group of patients - 28 (40±5.9%) and 9 (20±6%) in the study and comparison groups, respectively (p<0.05). Moreover, uterine myoma was detected during ultrasound examination in every third patient in both the study and comparison groups. Intramural myoma was significantly more common in patients in the study group (p<0.05).When compared with histological data from removed tissue and ultrasound elastography, the accuracy of adenomyosis diagnosis by elastography was 88.6%, sensitivity was 94.1%, specificity was 85%, the predictive value of a positive test was 80%, and that of a negative test was 95.8%. These results demonstrate the high effectiveness of a comprehensive ultrasound examination in women with adenomyosis in making a diagnosis and determining the severity of adenomyosis.