Sabirov Djura Marufbayevich, Usmanov Zayniddin Xalikovich, Batirov Ulugbek Beshimovich
Independent Researcher at the Department of Anesthesiology and Resuscitation, Center for the Development of Professional Qualifications of Medical Workers, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The methodological recommendation shows that one of the serious and dangerous complications of diabetes mellitus - hyperglycemic ketoacidosis coma, which is one of the urgent problems of medicine today, both in terms of the severity of its course and the possible complications that may occur, requires a modern new approach to this problem for specialists in the relevant field. Also, the issue of a systematic integrated assessment of the severity of the general condition in patients with hyperglycemic ketoacidosis coma and the development of an infusion program based on this integrated assessment is considered a necessary requirement of clinical medicine. This methodological recommendation is intended for resuscitators, endocrinologists, researchers, postgraduate residents, clinical interns.
Keywords:
Hyperglycemic ketoacidotic coma, Diabetes mellitus, Severe complications, Resuscitation, Endocrinology, Infusion therapy, Clinical assessment, Integrated approach, Emergency medical care, Modern treatment methods
Cite this paper: Sabirov Djura Marufbayevich, Usmanov Zayniddin Xalikovich, Batirov Ulugbek Beshimovich, Optimization of Intensive Treatment Tactics in Patients in Coma with Hyperglycemic Ketoacidosis, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3324-3331. doi: 10.5923/j.ajmms.20251510.10.
1. Introduction
Hyperglycemic ketoacidosis coma, one of the serious and dangerous complications of diabetes mellitus, is one of the most complex problems of clinical medicine today, both in terms of severity of the course and high mortality. This condition is a complex process that occurs in connection with insulin deficiency, tissue hypoxia, endogenous intoxication [4], water-electrolyte imbalance [14], metabolic changes, multiorgan dysfunctions [2,6,11].Adequate infusion therapy plays a leading role in the correction of hypovolemia. It is aimed at quickly filling the deficit of blood volume in motion, increasing the ability of the heart to pump blood, improving blood oxygen transport and oxygen uptake by body tissues. The most optimal way to do this, in combination with insulin therapy and other means of pharmacological coordination, allows to prevent the development of multiorgan failure in patients with hyperglycemic ketoacidosis coma [3,7,13,15].The addition of concomitant diseases of cardiovascular and inflammatory genesis, mainly against the background of diabetes mellitus, further worsens the estimated prognosis [2]. Despite the numerous scientific studies carried out and being developed today, a systematic integrated assessment that allows assessing the severity of the general condition of patients and predicting the possible serious consequences is not sufficiently used, methodological guidelines on the selection of differentiated tactics of infusion therapy have not been developed on a sound basis. The optimal ratio of the used infusion agents based on the qualitative and quantitative composition has not yet been determined. Indications for the use of these agents and their ratio according to the degree of organ dysfunction have not been established [4,6,11]. The lack of an algorithmic approach based on clear criteria, facilitating the professional activities of doctors working in medical practice, often reduces the effectiveness of intensive therapeutic measures, which, in turn, causes serious complications with irreversible consequences in organs and tissues [3]. Diabetes mellitus is one of the most unsolved problems of medicine to this day, the scale of which is constantly growing, affecting both the social and economic interests of people of all ages and in all countries of the world [1,10,14]. Hyperglycemic ketoacidosis coma is the most common acute and most severe complication of diabetes mellitus. This condition is characterized by severe tissue hypoxia, insulin deficiency, poisoning of organs and tissues with ketone bodies, impaired water-electrolyte balance, metabolic derangement, and the development of multiorgan failure.Research objective: to develop a systematic integrated assessment of the severity of the general condition of patients with hyperglycemic ketoacidosis and develop a scientifically based infusion program.
2. Materials and Methods Used
To find a solution to the formulated problems, we examined 106 patients with diabetes mellitus complicated by hyperglycemic ketoacidosis coma, aged 21 to 76 years. Of these, 52 were women and 54 were men. The duration of the disease ranged from 5 to 20 years. The patients were distributed according to age as follows: up to 30 years - 14 patients [1 died]; from 31 to 50 years - 43 [12 died]; from 51 to 70 years - 31 [7 died]; over 71 years - 18 [11 died]. Most patients [74 people] had type 1 diabetes. Type 2 diabetes was observed in 32 patients. The insulin dose used in the examined patients was 0.6±0.2 IU/kg per day.The main causes of diabetic decompensation and hyperglycemic ketoacidosis coma in the patients we observed are presented in Figure 1.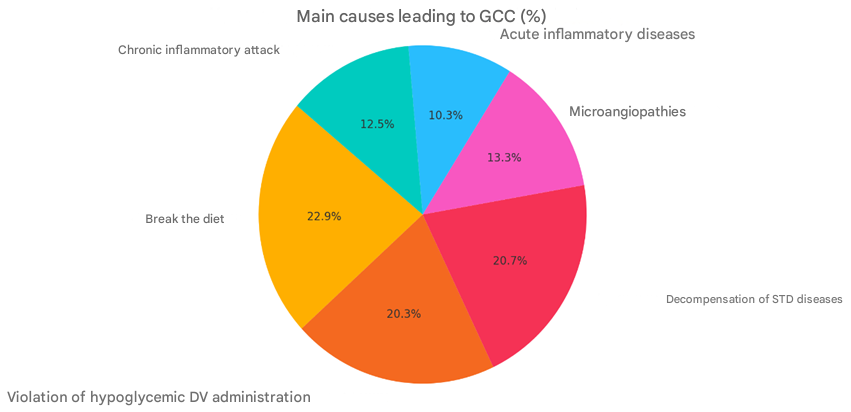 | Figure 1. Causes of hyperglycemic ketoacidotic coma (%) |
In the general structure of comorbidities, cardiovascular diseases [32.7%] were in the first place, and various inflammatory diseases [30.3%] were in the second place. The patients examined were initially divided into three groups depending on the stage of development of hyperglycemic ketoacidotic coma.The first group corresponded to the first (initial) stage of development of hyperglycemic ketoacidotic coma, characterized by moderate cellular dehydration, metabolic acidosis, and hyperkalemia due to increased cell membrane permeability.The second group corresponded to the second (cellular dehydration) stage of development of hyperglycemic ketoacidotic coma, characterized by a significant increase in osmolarity, electrolyte loss, ketonemia and ketonuria, and increasing cerebral symptoms.The third group corresponded to the third stage of development of hyperglycemic ketoacidotic coma (associated with general dehydration of the body), characterized by the maximum expression of clinical and biochemical manifestations of pathological processes, a pronounced increase in serum osmolality, severe symptoms of decompensated metabolic acidosis and general cerebral symptoms, combined with intracellular and extracellular dehydration.At the next stage of the study, the most simple and informative systems for dividing the examined patients into groups, applying and processing the data obtained were selected as the basis for assessing the severity of the general condition and the severity of the prognosis according to the SAPS II scale, as well as the degree of multiorgan failure according to the MODS scale.From the moment the patients were admitted to the intensive care unit, standard laboratory tests were performed. Biochemical tests were performed before the start of infusion-transfusion therapy, on the 1st-2nd and 3rd-4th days of the patients' stay in the intensive care unit. The level of glycemia was determined every 2-4 hours.The examination of biochemical and hematological parameters was carried out on the DIRUI SS-300B auto-chemistry Analyzer (China). Glycemia was determined on the Humalyzer Primus express analyzer (China). The study of the electrolyte composition of blood serum was carried out on the Rache HITACHI 902 apparatus of the Japanese company HITACHI.Serum osmolarity - using the Milliosmometer MT-2 apparatus, Russia. The colloid-oncotic pressure of blood serum was determined by the calculation method:KOBp = 0.52 x UZO – 11.4.where, KOBp – colloid-oncotic pressure of serum [mm. sim. above]; UZO – total serum protein [g/l].To study the parameters of central hemodynamics and the volemic index, the tetrapolar integral rheography method and tissue hydration were used in the cardiorespiratory system monitor complex KM-AR-01 – “Diamant”, St. Petersburg.Calculation of the parameters of central hemodynamics (stroke volume of the heart, stroke index, cardiac output, cardiac index, total peripheral resistance of blood vessels, specific peripheral resistance of blood vessels), as well as volemic indicators (total blood volume in the circulation, total serum volume in the circulation, total erythrocyte volume in the circulation) was carried out on a computer of the IBM/PC type using the software KM-AR-01 “Diamant”, St. Petersburg, according to the method of Tishenko M.I, modified by Yu.N.Volkov, V.G. Pokrovsky, I.P. Nikolayev et al.Echocardiography was performed on a series of patients using Clear Vae 550, Philips (Finland) and IDAN iM8 (Xt). The circulatory efficiency coefficient [CEC], which indicates the ratio of the pumping function of the heart to the total blood volume in circulation, was determined by the following formula:QASK = YUDH/AYUQH minute -1.Individual monitoring, including ECG, pulse oximetry, non-invasive arterial pressure measurement, capnometry, and body temperature measurement, was performed on the equipment “SCHILLIR ARGUS LCM plus” (Switzerland) and EDAN iM8 (China).
3. Technical Means and Methods of Processing Research Results
The results obtained in the study were processed on an IBM/PC computer using the basic package “Microsoft office 2010”. Methods for obtaining average values and mean square errors were used. General recommendations for medical and biological research were followed. The reliability of differences was assessed by calculating the Student's parametric test [t-distribution]. Differences between values were considered reliable when p <0.05 [t>2].Analysis of the data obtained showed that one of the leading systems sensitive to metabolic changes in organs and tissues in patients with hyperglycemic ketoacidosis coma is the cardiovascular system.The SAPS II scale allowed to classify patients and assess the probable prognosis of the disease. In this case, the higher the score, the higher the risk of developing a negative outcome. Subgroups with zero [up to 40 points] and 100% mortality [> 160 points] were excluded from the analysis. As a result, after randomization according to the results of the assessment on the SAPS II scale, 4 subgroups with a score rating from 60 to 160 points were formed [which, in turn, allowed to optimize the choice of the infusion therapy plan:1) the first subgroup [n=25] included patients in a state of hyperglycemic ketoacidotic coma [40-70 points on the SAPS II], the severity of their condition was mainly associated with acute endotoxicosis and water-electrolyte imbalance. In this case, the total circulating blood volume deficit was 25 ml/kg, which corresponded to stage I [moderate cellular dehydration] of the development of hyperglycemic ketoacidotic coma;2) the severity of the condition of patients in the second subgroup [n=36] with hyperglycemic ketoacidotic coma [71-100 points according to SAPS II], as in the first subgroup, was associated with acute endotoxemia and water-electrolyte imbalance. However, the total circulating blood volume deficit was 30 ml/kg, which corresponded to stage II [pronounced cellular dehydration] of the development of hyperglycemic ketoacidotic coma;3) in the third subgroup [n=29] [101-130 points according to SAPS II], the severity of the disease was accompanied by the onset of chronic inflammatory processes, which further aggravated the total circulating blood volume deficit [35 ml/kg], which corresponded to stage III [associated dehydration] of the development of hyperglycemic ketoacidotic coma;4) in the fourth subgroup [n=16] [131-160 points on SAPS II], the severity of the condition was assessed in combination with decompensation of concomitant cardiovascular diseases. The volume fraction of blood in the general circulation corresponded to the stage II [pronounced cellular dehydration] of the development of hyperglycemic ketoacidotic coma and was on average 27 ml/kg. Taking this into account, the SAPS II scale turned out to be optimal for the formation and analysis of groups of patients, and not for individual patients, but only for the assessment of the severity of the general condition of patients.Thus, the obtained results regarding the changes in the assessment of the severity of the general condition of patients indicate a high probability of positive results and effectiveness of rehydration therapy.If we consider the results of the analysis of similar indicators in deceased patients, it can be noted that the SAPS II score increased by 1-2 days and continued to increase until the end. The consistent increase in the score was characterized by the expressed decompensation of concomitant pathologies, the deterioration of the clinical condition of patients and an increase in the likelihood of adverse outcomes. Quantitatively, the increase in the score by 1-2 days in the control group increased by an average of 1.1 times for all subgroups, and in the main group by only 0.7 times. On the 3-4th day of infusion therapy, these indicators were 1.3 and 1.1 times, respectively.It should be noted that the main cause of death in patients with hyperglycemic ketoacidosis coma was multiorgan dysfunction and failure. Therefore, the assessment and diagnosis of multiorgan failure in patients with hyperglycemic ketoacidosis coma was carried out on the basis of simple, fairly simple research criteria. The multiorgan failure assessment system - MODS - adequately met these requirements. According to the results of our studies, in patients complicated by hyperglycemic ketoacidosis coma, which aggravates the course of diabetes mellitus, organ dysfunctions of one degree or another were observed in almost the same proportion. Dysfunction of various organs, except for the central nervous system, was observed in approximately 50% of cases in the form of mono- or polyfunctional disorders. Disorders of one degree or another in the functioning of the central nervous system were noted in 100% of cases. Pathological conditions in the blood coagulation system were much less common. In cases of hyperglycemic ketoacidosis coma, thrombocytopenia was rarely detected. The difference in scores in the groups ranged from 5 to 15.The results of the studies showed that in patients with hyperglycemic ketoacidosis coma, a decrease in the score on the MODS scale in the dynamic assessment of multiorgan failure is a positive predictive sign. On the contrary, an increase in the score on the MODS scale of multiorgan dysfunction is a negative predictive sign. The addition of clinically pathological symptoms was accompanied by a deterioration in the general condition and an increase in multiorgan dysfunction. Thus, the use of the MODS integral scale in dynamics to assess the degree of organ damage served not only as a method for classifying patients, but also made it possible to draw conclusions about the prognosis of the development of the pathological process in a particular patient, and to assess the effectiveness of the infusion therapy being carried out.Further results of the study showed that in both the control and main groups, surviving patients, the assessment scores significantly decreased by 1.4 and 1.8 times in the first two days, and by the end of the 4th day, this indicator decreased by almost 1.8 and 2.3 times, respectively. 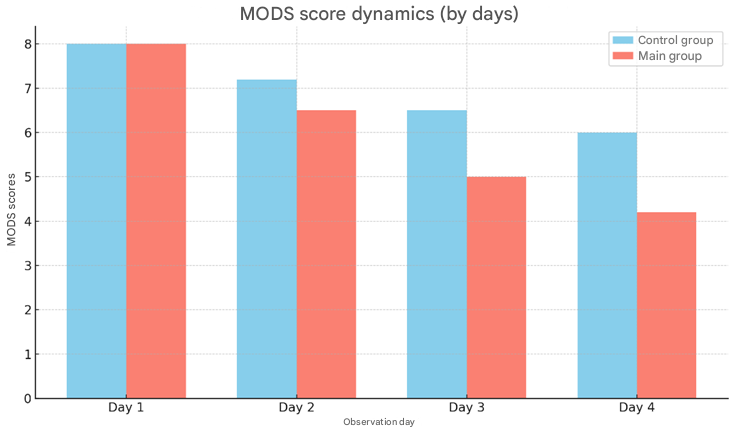 | Figure 2. Dynamics of MODS scores (in the control and main groups, by days) |
The dynamic score on the MODS scale corresponded to the level of treatment effectiveness. The percentage of patients who survived in the control and main groups was: in subgroup I - 83.3% and 92.9%, respectively; in subgroup II - 80.9% and 85.7%; in subgroup III - 35.3% and 60%; in subgroup IV - 20% and 44.5%. The overall effectiveness of treatment in the control group was 58.3%, in the main group - 74.6%.The results of the analysis showed that some patients admitted to the hospital had significantly higher scores on the MODS scale, which indicates a more serious clinical condition in them.This was confirmed by a significant increase in the score within the first two days from the start of treatment, indicating a progressive deterioration in the general condition of the patients [p<0.001]. In this case, the deterioration of the general condition was so severe that no further increase in the number of points was observed on days 3 and 4. This probably confirms that the deterioration of the general condition formed in the first two days was sufficient to end in death.In the control group, the quantitative increase in the score increased by an average of 1.58 times for all subgroups, and in the main group by only 0.77 times. In dynamics, the score on the MODS scale corresponded to the level of mortality. The proportion of patients who died in the control and main groups was: in subgroup I - 16.7% and 7.1%, respectively; II - 19.1% and 14.3%; III - 64.7% and 40%; IV - 80% and 55.6%. The overall mortality rate in the control group was 41.7%, in the main group - 25.4%. In order to optimize the infusion program, the main and control groups of patients were formed in these subgroups.In the main group [69 people], qualitatively and quantitatively stabilized pathogenetically based infusion programs were used, depending on the severity of the general condition of the patients according to the SAPS II scale. The volume and optimal ratio of saline, salt-free and colloidal solutions were selected based on the body weight of the patients.In the control group [37 people], a generally accepted traditional infusion program was used as part of infusion therapy.In the main group, patients used 0.9% sodium chloride or Rengatsit solution as saline solutions, 10% sodium chloride solution, and Succinasol solution as an antioxidant solution. 5% glucose solution was used as a salt-free solution, and Gelofusin and 10% albumin as colloidal solutions. In this case, attention was paid to the osmolarity of the solutions, the content of sodium, potassium and other electrolytes, as well as glucose.The use of solutions was carried out sequentially. First, crystalloid solutions (Sodium Chloride, Rengatsit, Succinasol) were administered, and then 10% sodium chloride was added to them. To optimize cell dehydration, a glucose-sparing solution (Cadens) was administered at the rate of 0.14±0.2 g per body weight. Then a colloidal solution (Gelofusin) was used. The volume, rate and sequence of infusion therapy, its qualitative composition were controlled on the basis of MVB, taking into account hemodynamic indicators, blood serum and urine osmolarity, colloid-oncotic pressure, electrolyte content, concentration indicators and volume of separated urine. Optimization of carbohydrate metabolism was carried out with short-acting insulin at the rate of 0.3±0.07 units per patient's body weight.One third of the dose [0.1±0.02 units/kg] was administered intravenously at a rate of 4.0-6.0±0.2 units/hour. The remaining amount of insulin was administered intramuscularly, maintaining the rate of decrease in glycemia at 3.0±0.5 mmol/hour. To compare the norm and the initial pathophysiological condition of patients in a state of hyperglycemic ketoacidosis coma, 14 practically healthy people were prospectively examined.In the intensive care of patients in a state of hyperglycemic ketoacidosis coma, the following were used:drugs with metabolic effects:– mildonium, 500-1000 mg per day;– tiotriozolin, 100-200 mg per day;– cocarboxylase, 100-200 mg per day;antioxidants and antihypoxants:– mexidol, 150-300 mg per day;– xanthinol nicotinate, 150-300 mg per day;nootropics:– Cytoflavin 10 ml 2 times in 100-200 ml of 0.9% sodium chloride solution.– Thiocetam 20-30 ml v / i in 100-200 ml of 0.9% sodium chloride solution.anticoagulants:– unfractionated heparin, 10-20 thousand units per day;– fractionated heparin – clexane, flenox 60-80 mg per day.Also drugs that improve blood microcirculation and rheological properties, H2-histamine blockers, cardiac glycosides, vitamin complexes.In the process of analyzing the results of the conducted studies, it was found that the central hemodynamic parameters of all four subgroups of patients in a coma with hyperglycemic ketoacidosis were similar, which made it possible to calculate the average value for each indicator in general.According to the data we obtained, the initial pathophysiological changes in patients in a coma with hyperglycemic ketoacidosis were characterized by significant changes in central hemodynamics. The heart rate index and cardiac index decreased by 45.5% and 30.4%, respectively, compared with the normal state [p<0.05]. An increase in the relative peripheral vascular resistance by 29.1% [p<0.05] and diastolic pressure by 27.9% [p<0.05] was noted, as well as tachycardia [30.5% increase in heart rate] [p<0.05].Thus, in the pathogenesis of reduced cardiovascular performance in patients with hyperglycemic ketoacidosis coma, a decrease in venous return to the heart, associated with various manifestations of associated dehydration occurring in the cell, is of great importance.Thus, the changes detected in central hemodynamics in patients in a state of hyperglycemic ketoacidosis coma indicated a violation of the compensatory mechanisms of the circulatory system, a sharp increase in cardiovascular insufficiency associated with a decrease in the pumping properties of the heart and the concomitant development of hypovolemia, the development of the “hypoperfusion” syndrome associated with the manifestation of various variants of dehydration. The exacerbation of the main pathological process leads to the destabilization of the microcirculatory control system, the intensification of various manifestations of limb ischemia and accompanying dehydration, and ultimately the formation of a hypokinetic type of blood circulation in patients, which was noted in 89.7% of patients in a state of hyperglycemic ketoacidosis coma.Certain differences were found in the frequency and severity of central hemodynamic changes in patients of subgroup I of the SAPS II scale during the implementation of the rehydration program. For example, in the control group of patients, the hypokinetic type of blood circulation was preserved during the first two days of treatment according to the generally accepted algorithm. At this stage, changes in central hemodynamic parameters remained mainly at the initial level and their elimination was clearly insufficient.For example, the mean diastolic pressure decreased by 7.4% [p<0.05], the initial tachycardia did not change.The heart rate index and cardiac index were not transformed, only the specific peripheral vascular resistance decreased by 37.3% [p<0.05]. In the next stage of the study, the mean diastolic pressure remained at a lower level by 3.3% [p<0.05]. The heart rate values did not change significantly. However, the heart rate index and cardiac index increased by 12% and 12.5%, respectively [p<0.05], QTSPQ decreased by 39% [p<0.05]. Thus, in the control group of patients in the second stage of the study, the hypokinetic type of blood circulation was preserved, its expression was slightly reduced in the last stage of the study.In patients in the main group, the implementation of an optimized infusion program already in the second stage of the study provided an improvement in central hemodynamic parameters, which was confirmed by a significant decrease in YUQT by 5%, ODB by 13.2%, YuZI by 24.4% and YUI by 14.3%. During the same periods, QTSPQ values almost doubled. On the 3rd-4th day of observation, a further improvement in central hemodynamic parameters was noted.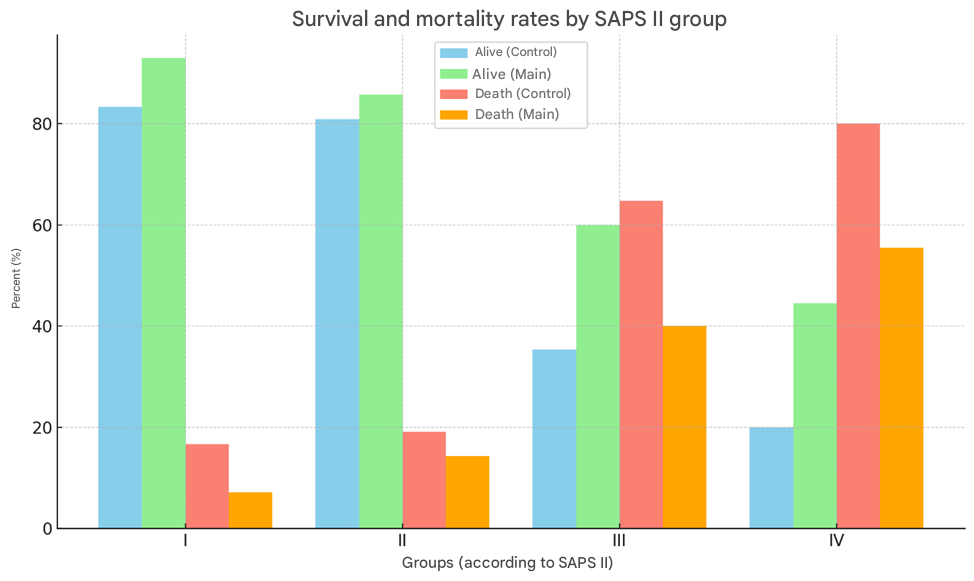 | Figure 3. Survival and mortality rates by SAPS II group (in percent) |
Thus, the use of optimized pathogenetically based infusion therapy in the main group of patients made it possible to sufficiently effectively compensate for volemic losses and stabilize the cardiovascular system at a new level, transferring it to a eukinetic type of blood circulation.Analysis of the results obtained in patients of subgroup II according to the SAPS II scale once again confirmed the differences in the degree of expression of changes in the manifestations of central hemodynamics in the conditions of the implemented infusion programs. For example, in the control group of patients, in the conditions of intensive infusion therapy, a hypokinetic type of blood circulation was noted in the first two days, just like in patients of subgroup I, but its expression clearly increased.At this stage, changes in central hemodynamic indicators remained mainly at the initial level, and the rehydration carried out did not eliminate the initial dehydration. In the third stage of the study, the HF remained at the initial level, the ABP decreased by 22% and the QTSPQ by 42% [p<0.05], the HF increased by 4% and the ICU by 9% [p<0.05].Thus, in patients in the control group, the circulatory system begins to stabilize relatively only by the 3rd-4th day of observation and passes into the eukinetic type.In the main group of patients, a significant improvement in central hemodynamic parameters was noted in the first two days when using a pathogenetically based infusion program. This was confirmed by a significant increase in the HF by 6%, the ABP by 17%, the HF by 42.7% and the ICU by 29.2%. During the same period, the QTSPQ values decreased by 59.5% [p<0.05]. At the last stage of observation, an improvement in central hemodynamic parameters was noted.Thus, the use of a coordinated infusion program in the main group of patients allows for a quick and complete solution to the problems of eliminating dehydration and transferring the circulatory system to a qualitatively new level - the eukinetic type.Analysis of the results in patients of subgroup III on the SAPS II scale showed that the formation of changes in central hemodynamic parameters was determined not only under the influence of infusion programs aimed at eliminating hyperglycemic ketoacidotic coma, but also under the influence of homeostatic changes caused by concomitant purulent-inflammatory diseases, which significantly determine the severity of the general condition of these patients. For example, in the control group, under generally accepted conditions of infusion therapy, during the first two days, a hypokinetic type of blood circulation was noted, just like in subgroup II, but its expression increased significantly. Moderate arterial hypotension and an increase in CSF pressure remained. At this stage of the study, pronounced changes in the cardiovascular system were noted more often than in similar patients in subgroup II. For example, the parameters of YuZI, YUI did not differ significantly from the initial indicators, QTSPQ decreased by 30.6%, respectively [p<0.05]. At the last stage of the study, changes in hemodynamic parameters due to the use of the generally accepted infusion program were accompanied by a decrease in ODB by 6.7% and QTSPQ by 42.7% [p<0.05]. The values of YuZI and YUI did not undergo significant changes. Thus, the reaction of the cardiovascular system under the influence of generally accepted infusion therapy in patients in subgroup III on the SAPS II scale showed a tendency to maintain a hypokinetic type of blood circulation with a characteristic deterioration of central hemodynamic parameters. Depression of the main hemodynamic indicators developed from the beginning of infusion therapy and persisted almost throughout the entire study period.In the main group of patients, in response to the implementation of coordinated infusion programs of rehydration, a decrease in the ABP by 8% [p<0.05] and an increase in the UZI and UUI by 38% and 54%, respectively, were noted on days 1-2 under stable UZI [p<0.05]. QTSPQ also significantly decreased by 53.7% [p<0.05]. On days 3-4 of observation, UZI [p<0.05] decreased by 6% and ABP by 25% [p<0.05] under conditions of an increase in UZI and UUI by 38% and 47.6%.Thus, as in the previous subgroups, regardless of the severity of the patient's general condition, the implementation of a coordinated infusion program contributed to the improvement of the indicators of ODB, YuZI, YUI and QTSPQ, while the nature of central hemodynamic changes in the study stages was most often represented by the eukinetic type of blood circulation.The results of the study in patients of subgroup IV according to the SAPS II scale showed that changes in central hemodynamic parameters were formed as a result of the implementation of infusion programs aimed not only at eliminating hyperglycemic ketoacidotic coma, but also at the changes that occur as a result of cardiovascular pathologies that cause and determine the severity of the general condition of these patients. For example, as a result of the use of conventional infusion therapy, a hypokinetic type of blood circulation was noted in the control group within the first two days, just like in patients of subgroup III. The deterioration of central hemodynamic parameters was characteristic: YUQT, O'DB increased. YuZI and YUI did not change compared to the initial data. QTSPQ decreased by 38.6% [p<0.05]. The depression of the main indicators of central hemodynamics, despite the initial correction, persisted at all stages of the study.Thus, in the control group of patients, under the influence of conventional infusion therapy, the severity of the initial hemodynamic disorders is not eliminated and no significant changes occur in the circulatory system.In the main group of patients under the influence of differential infusion programs, on the 1st-2nd day of observation, under stable conditions of ODB, a decrease in UFH by 6.4% [p<0.05], a change in YuZI and YUI by 37.6% and 40%, respectively [p<0.05]. QTSPQ also decreased significantly, namely by 55% [p<0.05]. On the 3rd-4th day of observation, a decrease in UFH by 12%, ODB by 6% [p<0.05], against the background of an increase in YuZI and YUI by 48% and 45% and a decrease in QTSPQ by 60%.Thus, the effect of a coordinated infusion program, even in patients with initial acute circulatory depression, leads to an improvement in central hemodynamic parameters by adapting the cardiovascular system to the eukinetic type of circulation.Thus, in 89.7% of patients in a state of hyperglycemic ketoacidosis coma, a hypokinetic type of circulation is noted, which is clearly evidenced by a sharp decrease in QTSPQ by 29.1%, ODB by 27.9%, YUZI by 45.5% and YUI by 30.4%.In patients in a state of hyperglycemic ketoacidosis coma, circulatory homeostasis disorders are noted in 97.4% of cases, associated with a decrease in UHQH by 43.4%, UHZH by 47.2% and UHEH by 31.1%.Due to a decrease in serum sodium concentration by 12.1%, a decrease in serum potassium concentration by 29.6% and zKOB by 17.5%, as well as an increase in serum osmolality by 16.5%, various water-electrolyte balance disorders are detected in 99.7% of the examined patients: in 21.7% of cases - moderate dehydration, in 51.2% - pronounced dehydration and in 26.8% - associated dehydration.The use of a generally accepted infusion program in patients in a coma with hyperglycemic ketoacidosis in 42% of cases does not provide sufficient stabilization of rehydration during the stages of intensive care.The severity and prognosis of the general condition of patients in a coma with hyperglycemic ketoacidosis should be determined according to the SAPS II scale, which is suitable for group assessment. In patients in a coma with hyperglycemic ketoacidosis, the severity of the general condition, multiorgan failure, and the effectiveness of intensive therapy should be assessed individually according to the MODS scale.The coordinated use of pathogenetically based infusion programs, taking into account the severity of the general condition of patients according to the SAPS II scale, leads to rapid stabilization of circulatory homeostasis and restoration of the circulatory system to a eukinetic type in 75% of cases, even at the initial stages of rehydration therapy.Consistent use of pathogenetically based, differentiated infusion programs, taking into account the severity of the patient's general condition according to the SAPS II scale, is an effective, reliable, and safe rehydration method in the treatment of patients in coma with hyperglycemic ketoacidosis.
References
| [1] | A. Boye, D. O. Acheampong, E. O. Gyamerah et al., “Glucoselowering and pancreato-protective effects of Abrus Pre-catorius (L.) leaf extract in normoglycemic and STZ/nic-otinamide—induced diabetic rats,” Journal of Ethnopharmacology, vol. 258, Article ID 112918, 2020. |
| [2] | B. A. Ahmed, A. S. Rao, and M. V. Rao, “In vitro callus andin vivo leaf extract of Gymnema sylvestre stimulate β-cellsregeneration and anti-diabetic activity in Wistar rats,” Phytomedicine, vol. 17, no. 13, pp. 1033–1039, 2010. |
| [3] | British Diabetic Association (BDA). (2023). Guidelines for the Management of Diabetic Ketoacidosis in Adults. Retrieved from: https://www.diabetes.org.uk. |
| [4] | D. O. Adeyemi and O. S. Adewole, “Hibiscus sabdariffarenews pancreatic β-cells in experimental type 1 diabeticmodel rats,” Morphologie, vol. 103, no. 341, pp. 80–93, 2019. |
| [5] | Fayfman, M., Pasquel, F.J., & Umpierrez, G.E.. Management of Hyperglycemic Crises in Patients with Diabetes. Endocrinology and Metabolism Clinics of North America, 2022, 49(1), 79-93. https://doi.org/10.1016/j.ecl.2019.10.005. |
| [6] | Gibb, F.W., et al. (2021). Management of Diabetic Ketoacidosis in Adults: A UK-Based Guideline. Diabetic Medicine, 2020, 38(9), e14633. https://doi.org/10.1111/dme.14633. |
| [7] | J. Yu, R. Zhang, T. Zhang et al., “Determination of too-sendanin and trans-anethole in Fructus Meliae Toosendanand Fructus Foeniculi by HPLC-MS/MS and GC-MS/MS inEvidence-Based Complementary and Alternative Medicine 31rat plasma and their potential herb-herb interactions,” Biomedical Chromatography: BMC, vol. 34, no. 7, Article IDe4837, 2020. |
| [8] | Joint British Diabetes Societies for Inpatient Care. Management of Hyperosmolar Hyperglycaemic State (HHS) in Adults: An updated guideline. Diabetic Medicine. 2023; 40(3): e14902. DOI: 10.1111/dme.14902. |
| [9] | Kitabchi, A.E., & Umpierrez, G.E. (2020). Hyperglycemic Crises in Diabetes Mellitus: DKA and HHS. Endocrinology and Metabolism Clinics of North America, 49(3), 487-501. https://doi.org/10.1016/j.ecl.2020.05.001. |
| [10] | M. Saleem, M. Tanvir, M. F. Akhtar, M Iqbal, and A Saleem,“Antidiabetic potential of Mangifera indica L. Cv. AnwarRatol leaves: medicinal application of food wastes,” Medicina(Kaunas, Lithuania), vol. 55, no. 7, 2019. |
| [11] | M. Srujana, R. Ramesh, and L. D. Nanjaiah, “Antidiabeticpotential of active fraction obtained from methanolic extractof Ichnocarpus frutescens: a possible herbal remedy,” Indian Journal of Pharmacology, vol. 50, no. 5, pp. 251–259, 2018. |
| [12] | Palacios, J.A., et al. Fluid Management in Diabetic Ketoacidosis: A Review of Current Evidence. Journal of Clinical Medicine, 2023, 12(2), 350. https://doi.org/10.3390/jcm12020350. |
| [13] | Pasquel FJ, Umpierrez GE. Hyperosmolar hyperglycemic state: a historic review of the clinical presentation, diagnosis, and treatment. Diabetes Care. 2024; 47(5): e123–e130. DOI: 10.2337/dc24-0123. |
| [14] | Umpierrez GE, Korytkowski M, ElSayed NA, et al. Hyperglycemic Crises in Adults With Diabetes: A Consensus Report. Diabetes Care. 2024; 47(8): 1257–1277. DOI: 10.2337/dci24-0032. |
| [15] | Wolfsdorf, J.I., Glaser, N., Agus, M., et al. (2022). ISPAD Clinical Practice Consensus Guidelines 2022: Diabetic Ketoacidosis and Hyperglycemic Hyperosmolar State. Pediatric Diabetes, 23(5), 522-546. https://doi.org/10.1111/pedi.13425. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML