-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3319-3323
doi:10.5923/j.ajmms.20251510.09
Received: Sep. 18, 2025; Accepted: Oct. 7, 2025; Published: Oct. 11, 2025

Application of the "VibroLUNG" Device in Comprehensive Intensive Care of Nosocomial Pneumonia in Patients with Combined Trauma
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLA. L. Rosstalnaya1, 2, Kh. Kh. Dadaev2, A. U. Takhirov2
1Center of Professional Development of Medical Workers, Tashkent, Uzbekistan
2Republican Research Center of Emergency Medicine, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the study was to analyze and evaluate the efficiency of vibroacoustic therapy using the “VibroLUNG” device as part of respiratory therapy in patients with combined severe traumatic brain injury, as well as to evaluate the results of the applied antibacterial protocol in the treatment of nosocomial pneumonia. A study of peripheral and central hemodynamics, as well as the dynamics of cerebrovascular parameters, was conducted under conditions of using various lung ventilation modes with vibroacoustic therapy using the “VibroLUNG” device in patients with combined severe traumatic brain injury complicated by nosocomial pneumonia. The data obtained showed that comprehensive antibacterial and respiratory therapy combined with vibroacoustic therapy reduced mortality by 19.2% in this patient group. The advantage and feasibility of using vibroacoustic therapy with the VibroLUNG device in a complex respiratory support system for patients with combined severe traumatic brain injury was proved.
Keywords: Nosocomial pneumonia, Pneumonia, Combined trauma, Traumatic brain injury
Cite this paper: A. L. Rosstalnaya, Kh. Kh. Dadaev, A. U. Takhirov, Application of the "VibroLUNG" Device in Comprehensive Intensive Care of Nosocomial Pneumonia in Patients with Combined Trauma, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3319-3323. doi: 10.5923/j.ajmms.20251510.09.
Article Outline
1. Introduction
- Today, the possibilities of intensive care in the treatment of patients with combined trauma have expanded [1]. The appearance of new drugs and technologies in intensive care units has reduced patient mortality due to traumatic shock. In most cases, the treatment of patients with severe trauma involves artificial lung ventilation (ALV), which is the most important method of correcting acute respiratory failure syndrome in neurosurgical patients. All these factors explain the importance of studying complications arising during respiratory support, one of which is nosocomial pneumonia (NP) [2-3].Despite certain successes achieved in recent decades in the treatment of patients with pneumonia, mortality rates remain high [4]. The NPs rank second in the structure of all hospital-acquired infectious complications, accounting for 15–18% [5-6], with ALV-associated pneumonia being associated with high mortality, with 33–70% of fatalities directly related to NPs [5]. According to various authors, the incidence of ventilator-associated pneumonia (VAP) ranges from 21.3 to 100%. Complications occur in 51.1% of ALV cases, and in 20.1% of deaths, they are the primary cause of death [2,6-7]. The diagnostics of NP is often quite a challenging task. A significant proportion of patients requiring long-term ALV have some form of respiratory pathology complicating differential diagnosis with pneumonia. It is most relevant for people with acute lung injury syndrome, chest injuries, pulmonary edema, concomitant chronic inflammatory pathology of the respiratory tract, etc. The high incidence of pneumonia in patients with combined trauma caused by resistant pathogens, as well as high attributable mortality rates and the inadequacy of initial empirical antibiotic therapy in general intensive care units, have led to the need to implement a strict protocol defining the initial empirical antimicrobial therapy in patients with severe combined trauma [6-9]. In recent years, convincing data has been obtained showing that in cases of timely and adequate empirical antibiotic therapy, the prognosis is significantly better than with delayed or inadequate therapy [8]. The main cause of severe and sometimes terminal conditions in patients with pneumonia is hypoxemia caused by acute respiratory failure. It should be noted that in pneumonia, as a rule, hypoxemia is initially combined with hypocapnia. Hypercapnia usually accompanies hypoxemia in the late stages of the disease, when treatment is unsuccessful. The most important pathogenetic factors causing the development of hypoxemia are: 1) exclusion of large areas of the lungs (segments, lobes, sometimes an entire lung) from ventilation, i.e., right-to-left intrapulmonary shunt; 2) interstitial pulmonary edema; 3) pulmonary circulation disorders; 4) intoxication impairing the oxygen-transport functions of the blood, leading to heart failure and alveolar pulmonary edema [10-11].The high incidence of nosocomial infections among patients with severe combined trauma, including severe traumatic brain injury, and an initial APACHE II score of more than 15 points leads to increased duration and cost of treatment in intensive care units, as well as high mortality rates [1,5,12]. Therefore, preventing the development of severe nosocomial infections is one of the most important tasks in treating this type of patients.The aim of the study was to analyze and evaluate the efficiency of vibroacoustic therapy using the “VibroLUNG” device as part of respiratory therapy in patients with combined severe traumatic brain injury, as well as to evaluate the results of the applied antibacterial protocol in the treatment of nosocomial pneumonia.
2. Material and Methods
- The study included 377 patients who were treated in the neurosurgical intensive care unit of the Republican Research Center of Emergency Medicine from 2019 to 2024. Only patients with combined severe traumatic brain injury (SCTBI) in whom nosocomial pneumonia (NP) was developed against the background of ongoing mechanical ventilation and based on the results of clinical and radiological examination were included in the comparative analysis. The mean age of men was 37.62±12.07 years (18-59 years), while the mean age of women was 41.07±12.66 years (21-58 years). Level of consciousness was not less than 7 points on the Glasgow Coma Scale. The inclusion criterion was a duration of mechanical ventilation exceeding 48 hours. The diagnosis of NP was considered probable in the presence of at least two of the following signs: body temperature above 38°C or below 36°C; white blood cell count >12×10⁹/L or <4×10⁹/L; appearance of new infiltrates on the radiograph; purulent nature of sputum.All patients underwent a clinical and neurological examination, monitoring of laboratory parameters (complete blood count, acid-base balance, arteriovenous oxygen difference - AVDO₂, hemoglobin oxygen saturation in the jugular vein - SO₂). The gas composition was studied in capillary, arterial and venous blood. The parameters were recorded at least 4 times a day on the EasyStat gas analyzer (Medical, USA), Roche OMNI C (Japan) from the blood of the radial or femoral artery, internal jugular vein with the calculation of the arteriovenous oxygen difference (AVO2) and the oxygen extraction coefficient (OEC). Measurement of cerebral hemodynamics. In patients of the second stage, cerebral blood flow was additionally examined using an HD 11 XE ultrasound scanner (Philips). The following hemodynamic parameters were evaluated through the middle cerebral artery (MCA): average linear blood flow velocity (Vm, cm/s); pulsatility index (Pi), characterizing vascular resistance; overshoot coefficient (OC), reflecting the dilation reserve. Standard access – temporal “window”. Calculation formulas:• Pi = (Vs – Vd) / Vm,• Vm = (Vs + 2Vd) / 3,• OC = V₂ / V₁ (based on the results of the carotid compression test).The studies were conducted on the 2nd day of admission and on the 7-8th day of hospital stay.In case of autoregulation disorder, intracranial pressure (ICP) was calculated using the formula: ICP = APm × RI × Vm⁻¹, where RI = (Vs – Vd)/Vs.Systemic hemodynamic indicators. Assessed by mean arterial pressure (MAP) and cerebral perfusion pressure (CPP): CPP = АDs × Vm × Vm⁻¹, where АDs — systolic blood pressure.Upon admission to the intensive care unit, patients received respiratory support in traditional SIMV VC, SIMV PC, and BiPAP modes (Drager, Hamelton device), as well as vibroacoustic therapy (VAT) using the “VibroLUNG” device. VAT is a non-invasive procedure of intensive vibroacoustic and resonance stimulation of the chest wall, both on the lung parenchyma and on the airways. [13-14]. The method is used for obstructive and restrictive pathology and inflammatory diseases of the lungs; it improves ventilation parameters by opening the functional reserve of the lungs, improving the drainage functions of the tracheobronchial tree and redistributing pulmonary perfusion. Vibroacoustic therapy also plays a significant role in the complex of resuscitation measures for respiratory failure.The VAT "VibroLung" device affects the respiratory tract with a generated sound signal from a bifocal position by two emitters in the range of 20-300 Hz. The floating effect of the sound wave causes a resonance effect, which has a safe and efficient impact on any type of damage to the lung parenchyma itself, as well as the bronchial tree, alveoli, and vessels. It allows to achieve better results with less intensity and exposure time, which is due to the oscillation of the vibroacoustic wave in the inhomogeneous pulmonary parenchyma and intrapulmonary component (edema, mucus, infiltration, hypostatic transudate), which improves drainage, ventilation, aeration, and reduces infiltration and proliferation [13-14]. The use of VAT against the background of mechanical ventilation reduces the area of lung collapse and atelectasis due to the effect on external pressure, the evacuation of bronchial secretions, promotes the acceleration of the processes of gravitational redistribution of intrapulmonary fluid and the improvement of ventilation-perfusion ratios. This, in turn, potentiates РЕЕР without additional increases in ventilation parameters.All patients initially received antibiotic therapy according to a protocol developed based on two regimens:• regimen 1 - cefoperazone/sulbactam 4 g/day + amikacin 1500–2000 mg/day;• regimen 2 - cefoperazone/sulbactam 4 g/day + levofloxacin 1000 mg/day.Subsequently, antibiotic therapy was adjusted based on the results of bacteriological studies.Patients were divided into two groups depending on the method of respiratory support:• Group I (n=190) — traditional mechanical ventilation, average duration - 10.9±1.3 days. The following modes were used: SIMV: FiO₂ 40–50%, Pasb 20–25 mbar, Pins 10–25 mbar, PEEP >7 mbar;• Group II группа (n=187) — a combination of traditional mechanical ventilation (SIMV) with vibroacoustic therapy (VAT) using the “VibroLUNG” device. The procedure lasted 5 minutes and was administered 3 to 10 times per day. The average duration of mechanical ventilation was 8.3±1.2 days. All patients in all groups were individually selected for mechanical ventilation parameters. Efficiency was assessed based on the following parameters: SpaO₂ — 96–99%, PaCO₂ — 34.7–35.2 mmHg., С, VCO.Data analysis was performed using STATISTICA 10 (StatSoft, Inc., 2011). The significance of differences was assessed using the Pearson χ² test at a p<0.05 level.
3. Results
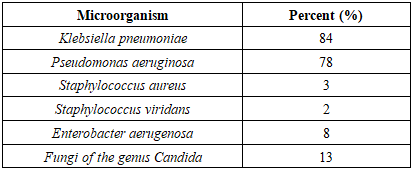
- Microbial landscape and antibiotic resistance analysis data were used to determine antibiotic sensitivity, which was distributed as follows: ceftriaxone 3%, ceftriaxone + sulbactam 84%, amikacin 82%, ciprofloxacin 86%, pefloxacin 23%, levofloxacin 81% (Tab. 1).
|
|

|

4. Discussion
- Nosocomial pneumonia. The use of combined ventilation was accompanied by a decrease in the incidence of pneumonia and a more favorable course of the infectious process, which was probably due to a reduction in the duration of mechanical ventilation (8.3 vs. 10.9 days) and improved mucociliary clearance.Survivability and outcomes. The average duration of coma in Group I was 6.63±1.89 days, and in Group II – 3.53±1.42 days. In the intergroup analysis, we did not find any statistically significant differences (р≥0,05). Among patients in Group I, favorable outcomes according to GOS were recorded in 18 (45%) patients, in Group II – in 43 (97.73%) patients (the difference with group I is statistically significant – p<0.001). Good recovery was achieved in 10% of patients in Group I, and in 40.91% of patients in Group II. We found a statistically significant difference between Group II and Group I at a level of p=0.003.All the data presented allow us to conclude that comprehensive respiratory support consisting of standard mechanical ventilation with sessions of high-frequency jet ventilation (HFJV) and vibroacoustic therapy using the “VibroLUNG” device is the most efficient.When conducting a comparative analysis of the clinical dynamics of Group II, we recorded the formation of cerebral ischemia due to the development of cerebral vasospasm in the intensive care unit, diagnosed clinically and instrumentally. A trend towards reduced mortality and improved neurological outcomes was recorded in Group II.
5. Conclusions
- The use of combined artificial lung ventilation with sessions of vibroacoustic therapy using the “VibroLUNG” device in patients with combined severe traumatic brain injury allows: to recruit the lungs, improve oxygenation and gas exchange parameters; to optimize cerebral hemodynamics and to reduce intracranial pressure; to shorten the duration of mechanical ventilation and to reduce the incidence of nosocomial pneumonia.Vibroacoustic therapy can be considered an efficient additional method in comprehensive intensive care for patients with SCTBI requiring long-term respiratory support, as well as in the prevention of secondary pulmonary complications.The antibacterial therapy protocol developed by us and applied according to schemes 1 and 2 in the ICU was the determining factor in reducing mortality in these patients using VAT by 18% and by 7% with traditional mechanical ventilation.
Ethical Approval and Consent to Participate
- Our institution's research ethics board does not require review or approval of case reports.Our investigation is conducted in accordance with the World Medical Association's Code of Ethics (Declaration of Helsinki).
Source of Funding
- Each author has reviewed and approved this manuscript. None of the authors has any conflict of interest, financial or otherwise. This manuscript is original, no part of it has been previously published, and it is not being considered for publication elsewhere. The corresponding author agrees to take full responsibility for authorship during the submission and review stages of the manuscript.
Conflict of Interests
- The authors declare no conflict of interest. This study does not include the involvement of any budgetary, grant or other funds. The article is published for the first time and is part of a scientific work.
ACKNOWLEDGEMENTS
- The authors express their gratitude to the management of the multidisciplinary clinic of Republican Research Center of Emergency Medicine for the material provided for our study.