-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3298-3302
doi:10.5923/j.ajmms.20251510.05
Received: Sep. 19, 2025; Accepted: Oct. 2, 2025; Published: Oct. 9, 2025

Optimizing the Management of Acute Adhesive Intestinal Obstruction in Children: A Retrospective Analysis of Surgical and Conservative Approaches
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSaydaliyev Sultongozi Sotvoldiyevich1, Sapoxonov Xasanhon Sapoxon ogli2
1PhD., Head of Deparment of General Surgery of Fergana Medical Institute of Public Health, Pediatric Surgeon of the Highest Category of Fergana Branch of Republican Scientific Center of Emergency Medical Care, Uzbekistan
2Lecturer of Fergana Public Health Medical Institute, Pediatric Surgeon of the Highest Category, Head of Department of Emergency Pediatric Surgery of Fergana Branch of Republican Scientific Center of Emergency Medical Care, Uzbekistan
Correspondence to: Saydaliyev Sultongozi Sotvoldiyevich, PhD., Head of Deparment of General Surgery of Fergana Medical Institute of Public Health, Pediatric Surgeon of the Highest Category of Fergana Branch of Republican Scientific Center of Emergency Medical Care, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article presents the experience of comprehensive treatment of children with adhesive disease of the abdominal cavity. It is based on the results of examination and treatment of patients with postoperative adhesive complications in the abdominal cavity, drawn from 195 cases treated at the clinic from 2023 to 2025. The patients’ ages ranged from 3 months to 18 years. A total of 152 (77.9%) patients were hospitalized once, 28 (14.3%) patients were hospitalized twice, and 12 (6.1%) patients were hospitalized 3 to 11 times. Of these, 29 (14.8%) had evident intra-abdominal adhesions and, to facilitate completion of a full videoendolaparoscopic adhesiolysis, received a preoperative intraperitoneal injection of a centrally prepared fibrinolytic mixture (composition: heparin 10,000 IU + fibrinolysin 20,000 IU + hydrocortisone 125 mg + gentamicin 80 mg + novocaine 0.25% – 200 mL) followed by protocolized therapeutic procedures. No postoperative complications or recurrence were observed. With the use of endovideolaparoscopic technology, all operated patients were mobilized early and had an average hospital stay of 3.7 days.
Keywords: Abdominal adhesive disease, Children, Prevention, Videolaparoscopic adhesiolysis
Cite this paper: Saydaliyev Sultongozi Sotvoldiyevich, Sapoxonov Xasanhon Sapoxon ogli, Optimizing the Management of Acute Adhesive Intestinal Obstruction in Children: A Retrospective Analysis of Surgical and Conservative Approaches, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3298-3302. doi: 10.5923/j.ajmms.20251510.05.
1. Introduction
- Acute adhesive intestinal obstruction (AAIO) is one of the complex issues in emergency abdominal surgery. According to various data, AAIO accounts for between 2.6% and 9.4% of all acute surgical abdominal conditions [1]. In recent years, contrary to expectations, there has been a rising trend in the incidence of this pathology [2] [1]. The number of patients with intestinal obstruction of neoplastic genesis is increasing each year. Against the background of a decrease in manifest forms of intestinal obstruction (volvulus, intussusception, etc.), the frequency of adhesive obstructions has significantly increased. This is often associated with patients’ late presentation to medical facilities and an increase in diagnostic errors at all stages of care for this category of patients [1] [3]. Acute mechanical intestinal obstruction, as a rule, requires prompt observation and treatment; thus, it is traditionally classified as a “clinical” pathology [3]. Emergency surgery remains the main method of treating patients with AAIO; however, the high rate of mortality and postoperative complications forces physicians to seek alternative treatment methods [4]. In the diagnosis of AAIO, an urgent surgical intervention is typically the first consideration. Early surgical doctrine held that “a patient with ileus must be operated on before the sun sets or before it rises on them” – in other words, within a few hours of onset. Today, surgery for acute mechanical AAIO is recognized as the only radical treatment. One of the leading figures in abdominal surgery, the Hungarian surgeon Imre Litteráti (Littmann), stated metaphorically in the 1970s: “…even the most advanced multicomponent drug therapy aimed at restoring water-salt balance cannot bring such relief to a patient with intestinal obstruction as cutting just one constricting adhesion with the surgeon’s finger and surgical instrument” [5]. This empirically accepted scientific concept remains relevant and pressing to this day.Aim of the Study: To analyze the diagnosis, treatment, and complications in pediatric patients with adhesive disease of the abdominal cavity (postoperative intra-abdominal adhesions and their consequences).
2. Materials and Methods
- This study is based on the examination and treatment results of 195 pediatric patients with adhesive complications in the abdominal cavity following surgical interventions, who were treated in our clinic from 2023 through 2025. The patients’ ages ranged from 3 months to 18 years. Of the total, 152 (77.9%) patients were admitted to the hospital once, 28 (14.3%) patients were admitted twice, and 12 (6.1%) patients were hospitalized between 3 and 11 times.All patients who developed abdominal pain syndrome after previous abdominal surgeries underwent standard clinical examinations, as well as abdominal ultrasonography. If ultrasound examination did not reveal clear signs of an adhesion process, additional instrumental and laboratory investigations were performed to determine the cause of the pain syndrome. These included plain abdominal radiography, contrast study of gastrointestinal passage, irrigography, fibrogastroduodenoscopy (FGDS), excretory urography, computed tomography (CT), and other relevant tests as needed.
3. Results and Discussion
- Among the 195 patients with adhesive disease of the abdominal cavity in our series, 29 (14.8%) underwent planned laparoscopic adhesiolysis. Conversion to open surgery was required in 10 cases (5.1%), and the remaining 156 patients (80%) were managed with conservative therapy. If an alternate pathology was identified as the cause of symptoms, patients were referred to the appropriate specialists (gastroenterologist, nephrologist, etc.). For patients in whom ultrasound examination confirmed the presence of adhesions, the treatment strategy depended on the severity of the pain syndrome and the patient’s medical history. In cases of mild to moderate pain, a full course of anti-adhesion (conservative) therapy was prescribed, followed by a repeat ultrasound evaluation. Patients with severe pain syndrome, as well as those who had experienced an episode of adhesive intestinal obstruction within the last three months, received a course of anti-adhesion therapy conducted in parallel with preparation for elective surgery.After the first course of anti-adhesion therapy, a follow-up abdominal ultrasound was performed. If the abdominal pain had resolved and the sonographic signs of adhesions were absent, patients were discharged for outpatient follow-up. These patients were advised to adhere to a diet and were monitored for 3–5 years, with abdominal ultrasound check-ups once every 6 months [6].
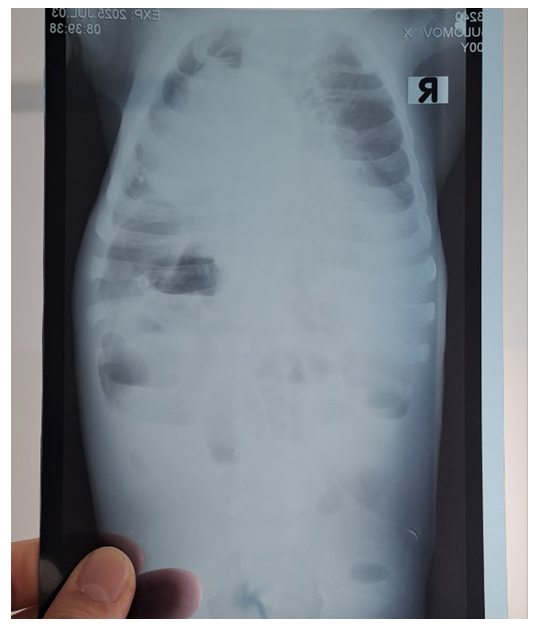 | Figure 1. Patient I.A., 11 years old, diagnosis: AAIO. Diagnostic abdominal radiograph |
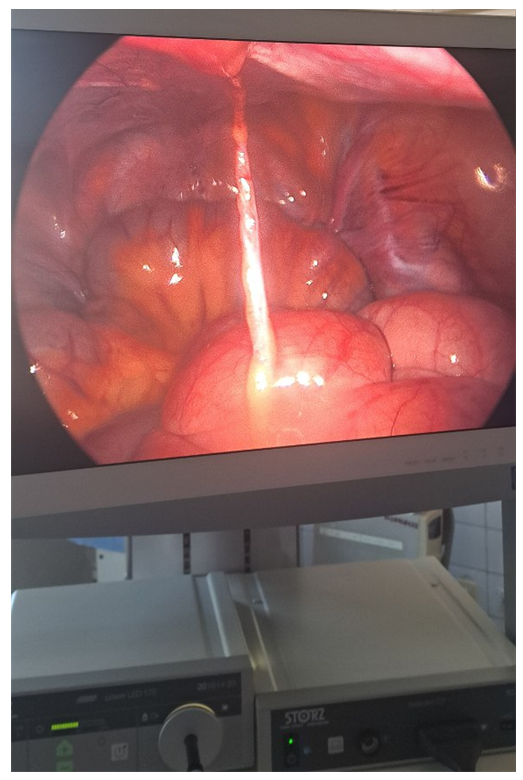 | Figure 2. Patient I.A., diagnosis: AAIO. Intraoperative view during adhesiolysis |
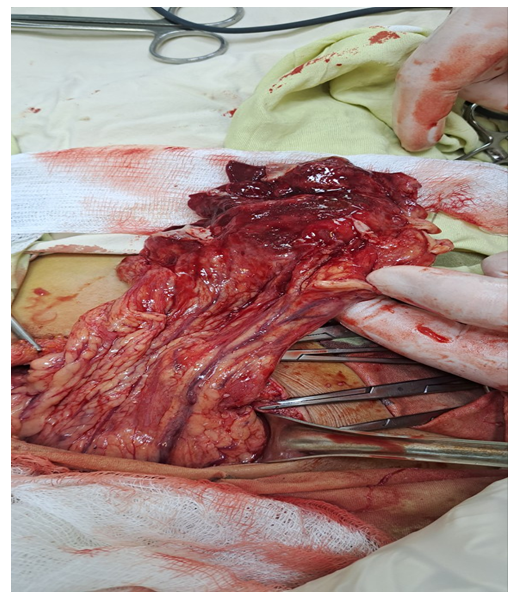 | Figure 3. Patient K.B., 14 years old, diagnosis: AAIO. Necrotic intestinal tissue following adhesive intestinal obstruction |
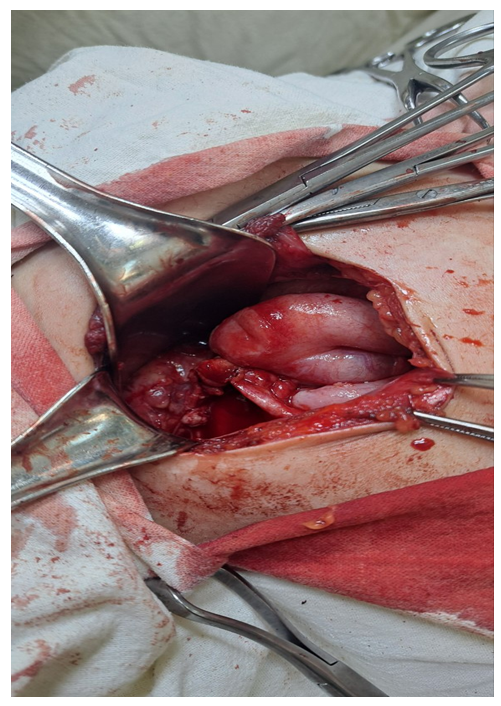 | Figure 4. Patient I.A., diagnosis: AAIO. Operative process (laparotomy after conversion) |
4. Conclusions
- Indications for elective surgical treatment of patients with acute adhesive intestinal obstruction include an unsatisfactory clinical effect of conservative therapy and the presence of ultrasound signs of intestinal loops adherent to the parietal or visceral peritoneum. In patients who achieved a clearly positive clinical effect from conservative management—namely, when the ultrasound signs of conglomerated adhesions to the peritoneum were eliminated—multiple courses of conservative therapy were carried out until the pain syndrome had completely resolved. The above information confirms that minimally invasive surgical methods are necessary for the early prevention of abdominal adhesive disease. The use of our fibrinolytic mixture (FLM) during surgery dissolves fibrin bands, normalizes fibrinolysis, and most importantly, prevents the formation of adhesions. Performing videolaparoscopic adhesiolysis with intraoperative FLM treatment of the abdominal cavity lowers fibrinogen levels and normalizes fibrinolysis; this approach has proven effective in the postoperative management and early prevention of adhesive disease in children.