-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3294-3297
doi:10.5923/j.ajmms.20251510.04
Received: Aug. 31, 2025; Accepted: Sep. 28, 2025; Published: Oct. 9, 2025

Morphological Representation of the Lung Surfactant Deficiency Model
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLSapaeva Sharofat Aminovna
Ph.D., Associate Professor, Head of the Department of Human Anatomy, Urgench State Medical Institute, Uzbekistan
Correspondence to: Sapaeva Sharofat Aminovna, Ph.D., Associate Professor, Head of the Department of Human Anatomy, Urgench State Medical Institute, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

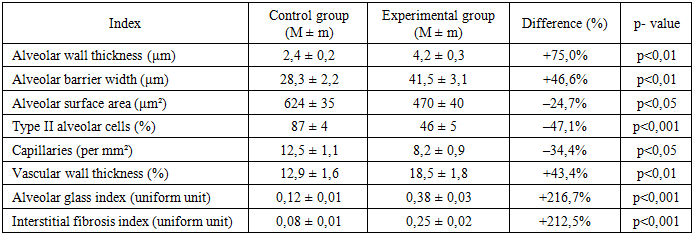
Surfactant deficiency is a major pathogenetic factor not only in neonatal respiratory distress syndrome (RDS), but also in adult acute respiratory distress syndrome (ARDS). In this study, the morphostructural changes that occurred in rat lung tissue in an experimental model of surfactant deficiency were studied using histological and morphometric methods. According to the results, in the experimental group, the alveolar walls thickened by 75%, the alveolar surface area decreased by 25%, and the number of type II alveolocytes decreased by 47%. In addition, edema, inflammatory infiltration, and fibrosis processes were observed in the interstitial tissues. Deficiency of type II alveolocytes and impaired surfactant synthesis led to the development of microatelectasis, a decrease in the gas exchange area, and increased hypoxia. These changes formed the morphological basis of respiratory distress syndrome and clinically indicated the possibility of developing chronic respiratory failure and pneumosclerosis. The data obtained serve as an important scientific basis for the development of new therapeutic agents for surfactant deficiency.
Keywords: Surfactant deficiency, Respiratory distress syndrome, Alveolocyte type II, Morphometry, Structural changes in the lungs, Interstitial edema, Fibrosis
Cite this paper: Sapaeva Sharofat Aminovna, Morphological Representation of the Lung Surfactant Deficiency Model, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3294-3297. doi: 10.5923/j.ajmms.20251510.04.
Article Outline
1. Introduction
- Surfactant deficiency is one of the main pathogenetic factors not only in respiratory distress syndrome observed in newborns, but also in acute respiratory distress syndrome (ARDS) developing in adults. Insufficient production of surfactant in the lung tissue or impaired function is manifested by alveolar collapse, impaired gas exchange, and hypoxia [1,2]. Surfactant deficiency in the neonatal period is often associated with high perinatal mortality and disability, which further increases the relevance of research in this area [4]. Although artificial ventilation, surfactant therapy, and intensive care methods are currently used to eliminate respiratory failure, in-depth study of morphostructural changes is crucial for the development of effective therapeutic approaches [3]. At the same time, ARDS observed in adults can often develop in conditions complicated by sepsis, pneumonia, trauma, or COVID-19. From this point of view, the study of the morphostructural manifestations of lung tissue is of great importance not only for the field of fundamental morphology, but also for clinical practice [5,8]. In this process, the detection of microscopic changes in the lungs, in particular, pathological changes in the alveoli, bronchioles, interalveolar barriers and capillary endothelium is an important scientific task [6]. The study of morphological changes by creating surfactant deficiency in experimental models not only provides an understanding of pathogenesis, but also creates a basis for the development of new drugs and biotechnological tools in the future [7]. In addition, by analyzing the changes occurring in epithelial cells, macrophages and interstitial connective tissue in the respiratory tract, it is possible to gain a deeper understanding of the mechanisms of inflammation and fibrosis [9, 12]. This is useful not only for understanding the pathogenesis of ARDS, but also for chronic obstructive pulmonary disease and interstitial pneumonia [10]. In the context of the acute respiratory syndrome pandemic (especially in cases associated with SARS-CoV-2), it has been confirmed once again that surfactant system dysfunction is a major factor in respiratory failure [11]. Therefore, the study of morphological manifestations in surfactant deficiency models is relevant not only from the point of view of traditional pneumopathologies, but also from the point of view of the global epidemiological situation. In conclusion, the study of morphostructural changes in lung tissue based on the surfactant deficiency model is of great importance not only from a scientific but also from a practical point of view. This research will serve to improve therapeutic strategies used in respiratory failure, test new innovative drugs, and improve the vital indicators of patients [13].The aim of this study is to identify morphostructural changes in rat lung tissue using histological and morphometric methods based on the study of an experimental model of surfactant deficiency and to evaluate these changes in relation to the pathogenesis of respiratory distress syndrome.
2. Materials and Methods
- The study was conducted on adult male Wistar rats with an average body weight of 180–220 grams. The animals were kept in standard laboratory conditions, and the feeding and care procedures were carried out in accordance with the International Bioethics Guidelines and Standards for the Use of Laboratory Animals (OECD, 2018; WHO, 2020). The rats involved in the experiment were divided into two groups: a control group and an experimental group called a surfactant deficiency model.In order to form a surfactant deficiency model, special methods were used to inhibit lung surfactant in animals. Under these conditions, an increase in the surface tension of the alveoli, their closure and the appearance of microatelectasis were observed, which clinically formed a model of respiratory distress syndrome.All animals were anesthetized under anesthesia and lung tissue was obtained. The obtained materials were fixed in 10% formalin solution, paraffin blocks were prepared, and 4–5 μm thick sections were prepared using a microtome. Various staining methods were used for morphological analysis: hematoxylin-eosin (H&E) to assess general histoarchitecture, Masson trichrome to detect fibrosis and collagen tissue. Surfactant Protein C was also used to assess type II alveolocytes. For morphometric analysis, the average alveolar wall thickness, alveolar barrier width, alveolar surface area, type II alveolocyte proportion, capillary density, and vascular wall thickness were calculated. Also, conditional indicators such as the alveolar edema index and interstitial fibrosis index were determined to assess pathomorphological processes. The results obtained were processed using mathematical and statistical methods. Each indicator was expressed as M ± m.The results of the study of the experimental model of surfactant deficiency showed consistent morphostructural changes in the lung tissue of rats. Histological analyses showed that, in contrast to the normal control group, the alveolar walls were thickened, the interstitial tissue was saturated with fluid, and elements of inflammatory infiltration were noted. Dystrophic changes were detected in the epithelial layer of the bronchioles, and in some places signs of desquamation. Histological analyses of the experimental group showed a number of pathological changes in the lung tissue, in contrast to the control group. In particular, the alveolar walls were significantly thicker than the theoretical norm, and their elasticity was reduced. In the interstitial tissues, edema elements were clearly visible and remained saturated with fluid. These changes lead to a decrease in the efficiency of the gas exchange process. Structural lung.Inflammatory infiltration elements were noted in the alveolar walls: accumulation of lymphocytes, macrophages, and in some cases neutrophils was observed. Such infiltration indicated the development of a chronic inflammatory process in the lung parenchyma. Dystrophic changes, granularity of the cytoplasm, pyknosis of the nuclei, and signs of vacuolation were noted in the epithelial layer of the bronchioles. In some parts of the epithelium, the boundaries of the cells were blurred and desquamation processes were noted - that is, the separation of cells from the basement membrane.Also, in some bronchioles, disproportionate thickening and twisting of the epithelial layer were observed, combined with dystrophic changes in the cellular composition. The muscle layers were also visible with unclear boundaries and in some places remained saturated with fluid. The vessel walls were also thickened, the endothelial cells were swollen, and in some places the cytoplasm was shown to be vacuolated (Fig. 1).
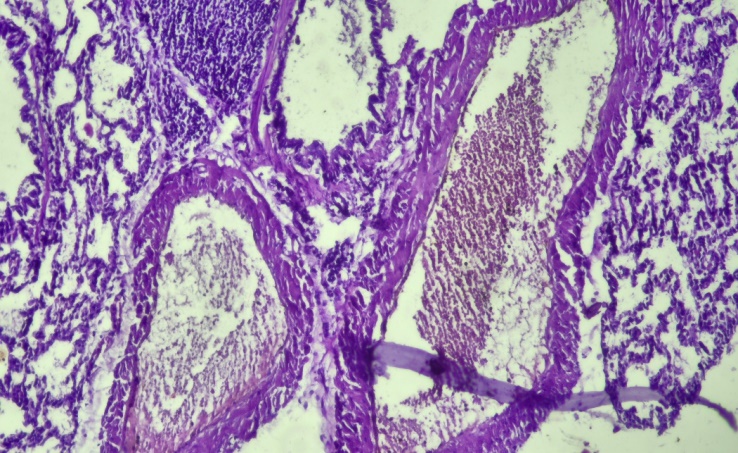 | Figure 1. The vessel wall is thickened and surrounded by lymphocytic infiltration. The interalveolar septa are thickened, with a tendency to fibrosis in some areas. Staining — hematoxylin-eosin, magnification ×400 |
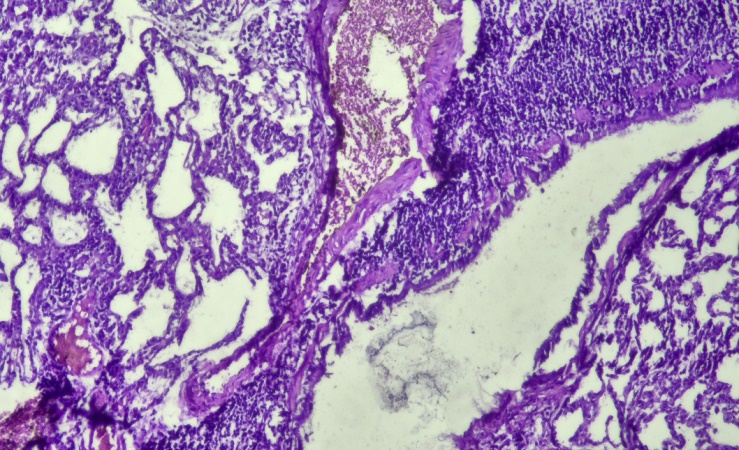 | Figure 2. Histological appearance of lung tissue. The alveoli show morphological abnormalities and dilatation. The interalveolar septa are thickened and in some places covered with cellular infiltration. Numerous inflammatory cells are found in the perivascular and peribronchiolar areas. Staining: hematoxylin-eosin, magnification ×200 |
|
3. Discussion of the Obtained Data
- The results of this study showed that the study of the surfactant deficiency model causes significant morphostructural changes in rat lung tissue. Morphological analyses revealed that changes such as thickening of the alveolar walls, interstitial edema, and inflammatory infiltration were consistently observed in the experimental group. These changes may reduce the efficiency of the gas exchange process and lead to increased hypoxia. A significant decrease in the number of type II alveolocytes and the disappearance of their luminal bodies were consistent with a decrease in surfactant synthesis. This exacerbates the situation associated with the closure of the alveoli, the development of microatelectasis, and a reduction in the gas exchange area. These findings are consistent with the studies of Sweet et al. (2019) and Jobe & Ikegami (2001). They also noted the dystrophy of type II alveolocytes and a decrease in surfactant proteins as one of the morphological bases of surfactant deficiency.Morphometry revealed a 75% increase in the thickness of the alveolar wall, a 25% decrease in the alveolar surface area, and a 47% decrease in the number of type II alveolocytes. These indicators indicate not only a decrease in gas exchange, but also the possibility of the development of chronic sclerotic processes in the lung parenchyma. At the same time, a sharp increase in the alveolar edema index and interstitial fibrosis index indicated the onset of irreversible tissue changes. This condition clinically constitutes the morphological basis of pneumosclerosis and chronic respiratory failure (ARDS Network, 2000).The results obtained are of great importance not only for a deeper understanding of the pathogenesis, but also for the effective evaluation of surfactant therapy in neonatal intensive care and adult ARDS. They also serve as a scientific basis for the development of new biopolymer and nanotechnological tools aimed at compensating for surfactant deficiency.
4. Conclusions
- 1. The experimental model of surfactant deficiency caused consistent morphostructural changes in rat lung tissue - thickening of the alveolar walls, interstitial edema and inflammatory infiltration.2. The proportion of type II alveolocytes decreased significantly, and as a result of the weakening of surfactant synthesis, microatelectasis and a reduction in the gas exchange area were observed.3. Morphometric analyses were characterized by a 75% increase in alveolar wall thickness in the experimental group, a decrease in the number of capillaries, and a sharp increase in alveolar edema and interstitial fibrosis indices.4. These changes constitute the morphological basis of respiratory distress syndrome and hypoxia, and are an important scientific and practical basis for the correction of surfactant deficiency and the development of new treatment methods.