Gulchekhra Kh. Khasanova1, Nigora Kh. Tukhtaeva2
1PhD Student of the Department of “Propaedeutics of Internal Diseases No. 2” of the Tashkent Medical Academy, Senior Lecturer of the Department of “Applied Cosmetology” of the Tashkent International Kimyo University, Tashkent, Uzbekistan
2Doctor of Medical Sciences, Associate Professor of the Department of Propaedeutics of Internal Diseases No. 2 of the Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Gulchekhra Kh. Khasanova, PhD Student of the Department of “Propaedeutics of Internal Diseases No. 2” of the Tashkent Medical Academy, Senior Lecturer of the Department of “Applied Cosmetology” of the Tashkent International Kimyo University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
A prospective observational study included 150 women aged 16–41 years with metabolic syndrome and serum 25(OH)D levels below 30 nmol/L. All participants were followed on an outpatient basis. The assessment protocol comprised anthropometric measurements, bioimpedance analysis of body composition, evaluation of carbohydrate and lipid metabolism, and genotyping of VDR polymorphisms (FokI and ApaI). The therapeutic program consisted of daily administration of cholecalciferol at a dose of 10,000 IU, myo-inositol 4 g, and adherence to a low-carbohydrate high-fat (LCHF) diet, in addition to standard metabolic syndrome therapy (metformin). After 8 weeks of intervention, the median serum 25(OH)D level reached the optimal range; body mass index decreased by 7.8% (p < 0.01), and waist circumference was reduced by 6.5% (p < 0.01). Significant improvements were also observed in HOMA-IR (−32%), triglycerides (−18%), and LDL-C (−11%), accompanied by an increase in HDL-C (+9%). The most pronounced metabolic benefits were recorded in carriers of the minor alleles FokI-T and ApaI-C. For the first time in the female population of Uzbekistan, an association between vitamin D deficiency and metabolic syndrome with VDR gene variants was confirmed, and the high effectiveness of a combined nutraceutical approach on an LCHF background was demonstrated. Based on the findings, a screening algorithm was developed that includes mandatory measurement of 25(OH)D levels and consideration of genetic risk factors, thus opening avenues for personalized therapy and improving both clinical outcomes and socioeconomic efficiency of treatment.
Keywords:
Metabolic syndrome, 25(OH)D, VDR gene, Body mass index, Insulin resistance
Cite this paper: Gulchekhra Kh. Khasanova, Nigora Kh. Tukhtaeva, Metabolic Syndrome in Women with Vitamin D Deficiency: Clinical Course and Implications, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3287-3293. doi: 10.5923/j.ajmms.20251510.03.
1. Introduction
To study the features of metabolic syndrome in women with vitamin D deficiency; to evaluate the impact of allelic and genotypic variants of VDR gene polymorphisms in patients with MS and vitamin D deficiency; and to improve the diagnostic and treatment algorithm for metabolic syndrome.Metabolic syndrome (MS) is one of the key medical and social problems of modern healthcare, as it is associated with a high risk of type 2 diabetes, cardiovascular disease, and all-cause mortality [1,2]. According to epidemiological studies, the prevalence of MS among women of reproductive age is steadily increasing, largely due to lifestyle changes, physical inactivity, and dietary factors [3].In recent years, special attention has been paid to the role of vitamin D deficiency as an independent risk factor for the development of MS components [4]. It is well established that low 25(OH)D levels are associated with obesity, disturbances of carbohydrate and lipid metabolism, and insulin resistance [5,6]. Furthermore, polymorphisms of the vitamin D receptor (VDR) gene, particularly FokI and ApaI, influence tissue sensitivity to vitamin D and may determine individual features of the MS course [7,8].Despite the accumulated evidence, information on the relationship between vitamin D deficiency, genetic markers, and clinical manifestations of MS in the female population of Central Asia remains limited. This highlights the need for in-depth studies aimed at elucidating pathogenetic mechanisms and developing personalized strategies for the treatment and prevention of MS, taking into account vitamin D status and genetic predictors.Thus, investigating the features of metabolic syndrome in women with vitamin D deficiency has high clinical and social significance, opening prospects for implementing personalized treatment programs and improving their effectiveness.
2. Materials and Methods
A total of 150 women with clinically diagnosed metabolic syndrome, who were under outpatient observation at the “Level Med” clinic and the National Medical Center during the period from 2023 to 2024, were included in the study. The mean age of the participants was 34 ± 6 years. All patients were thoroughly informed about the aims and protocol of the study and provided written informed consent to participate.The examination program was based on a comprehensive approach and included:• Questionnaire survey and collection of subjective data concerning medical history and lifestyle;• Anthropometric assessment (body weight, height, body mass index, waist and hip circumference);• Clinical and laboratory tests, including complete blood count and biochemical analysis, measurement of glucose, homocysteine, and insulin levels, calculation of HOMA-IR index, lipid profile, as well as serum 25(OH)D concentration;• Genetic analysis aimed at determining two polymorphisms of the vitamin D receptor (VDR) gene — FokI and ApaI.All stages of the examination were carried out according to a unified protocol, following methodological standards that ensured reproducibility and reliability of the obtained data.
3. Results and Discussion
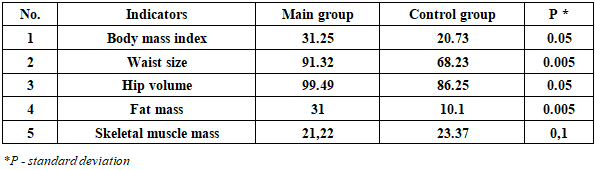
Analysis of the characteristics of the women included in the study revealed several factors determining a high risk of metabolic disorders. One of the key modifiable factors was age: it was established that in women over 35 years, the risk of obesity increased substantially (RR = 2.52; 95% CI 2.12–3.01; OR = 6.36; 95% CI 4.14–9.66). This result is consistent with population-based studies showing an increase in the prevalence of overweight and obesity among women aged 35–45 years. According to our analysis, the mean age of women with normal body weight was 32.3 ± 4.4 years, which was significantly lower than that of patients with overweight (37.7 ± 2.8 years; p = 0.035) and obesity (40.7 ± 4.2 years; p < 0.0001). (Table 1).Table 1. Characteristics of patients by age and BMI data
 |
| |
|
Subjective DataAccording to the results of the questionnaire survey (Fig. 1), a number of clinical and anamnestic features were identified: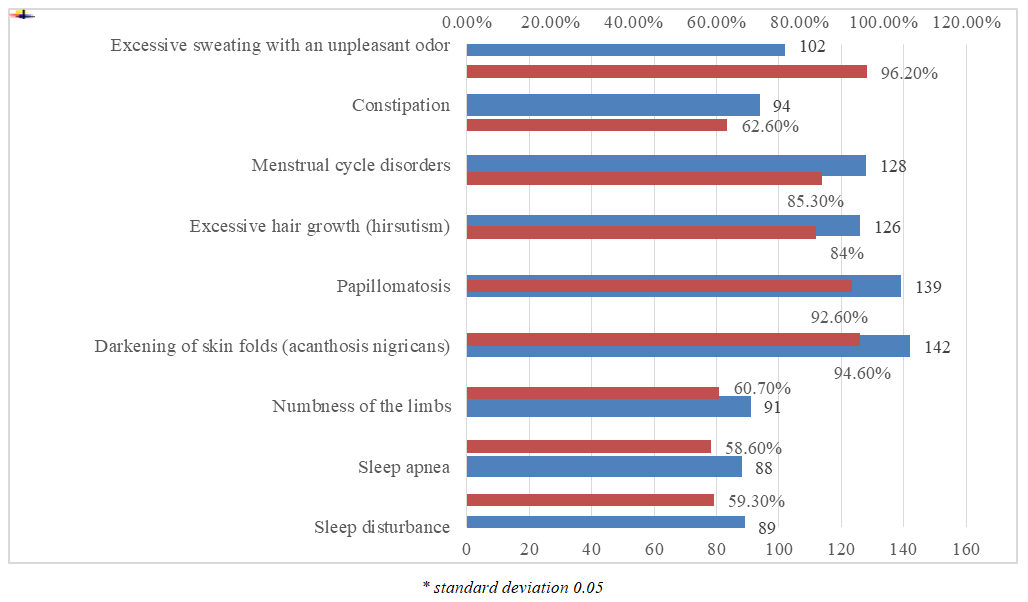 | Figure 1. Analysis of subjective complaints other than excess weight of the examined patients (n = 150) |
The diagram illustrates the frequency of major complaints among women of reproductive age who underwent screening for metabolic syndrome (MS). The data are presented both in absolute numbers (red values) and as percentages of the total sample (labels on the right axis).Clinical-anamnestic highlights:1. Dermatological manifestations of insulin resistance. Acanthosis nigricans and papillomatosis were observed in 94.7% and 92.7% of women, respectively, indicating long-standing hyperinsulinemia. In current literature, these dermatological signs are regarded as cutaneous markers of pronounced insulin resistance and early predictors of MS and type 2 diabetes [4].2. Endocrine-reproductive disorders. The high prevalence of oligo-/amenorrhea (85.3%) and clinical hirsutism (84.0%) suggests a phenotype of polycystic ovary syndrome (PCOS) overlapping with MS. This condition is associated with vitamin D deficiency and an increased cardiovascular risk, thereby justifying extended laboratory testing (serum 25(OH)D, LH/FSH ratio, total and free testosterone, HOMA-IR).3. Somatovegetative manifestations. More than half of the women reported hyperhidrosis, constipation, paresthesias, as well as sleep disturbances including episodes of apnea. This symptom complex reflects early signs of autonomic dysfunction and obstructive sleep apnea (OSA), which contribute to the aggravation of insulin resistance and arterial hypertension.The results show that cutaneous and reproductive manifestations—pathognomonic signs of metabolic disturbances—are present in more than 80% of overweight women. This underscores their high clinical and diagnostic significance for MS screening and for the development of preventive programs.Anthropometric indicators of the examined women also varied within different ranges (Table 2).Table 2. Bioimpedance data and BMI of respondents in the main and control groups
 |
| |
|
Analysis of the bioimpedance data confirmed that abdominal fat distribution (waist circumference > 91 cm) serves as an objective criterion of metabolic syndrome and is significantly correlated with the severity of insulin resistance and elevated vascular risk.The presence of sarcopenic obesity—a combination of reduced skeletal muscle mass with excessive fat accumulation—reflects an unfavorable prognosis, since a decrease in muscle mass reduces tissue insulin sensitivity and limits the body’s metabolic reserve.Practical implications:1. The primary therapeutic focus should be directed toward reducing fat mass while maintaining or increasing skeletal muscle mass. This can be achieved through resistance training, adequate protein intake, and optimization of vitamin D status.2. To objectively assess dynamics, it is recommended to perform repeated bioimpedance analysis every 3–6 months and to measure waist circumference monthly.The next stage of the respondents’ evaluation consisted of laboratory testing (Table 3).Table 3. Analysis of vitamin D levels in the blood depending on the BMI indicators of respondents
 |
| |
|
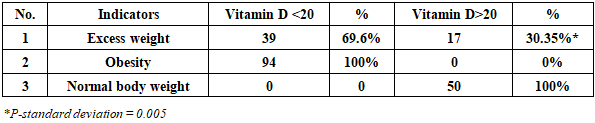
Analysis of the obtained data revealed a clear inverse relationship between serum 25(OH)D concentration and the degree of excess body weight. A decrease in vitamin D levels was accompanied by a significant increase in the likelihood of shifting from the normal BMI range toward obesity. In the study cohort, 25(OH)D deficiency was statistically significantly associated with both overweight and, to a greater extent, obesity. These results emphasize the need for targeted screening and timely correction of vitamin D deficiency as an integral component of comprehensive prevention and therapy of metabolic syndrome.Pathophysiological mechanisms:• Sequestration in adipose tissue. Expansion of fat depots reduces circulating 25(OH)D levels due to adipocyte “trapping” and an increase in the distribution volume.• Metabolic impairment. In obesity, there is suppression of 1-α-hydroxylase activity, acceleration of 25(OH)D catabolism by 24-hydroxylase, and chronic low-grade inflammation, all of which collectively reduce the bioavailability of active metabolites.• VDR signaling dysfunction. Vitamin D deficiency disrupts the expression of IRS-1 and GLUT-4, which exacerbates insulin resistance and creates a “vicious cycle” of further fat accumulation.• The data presented below demonstrate that reduced vitamin D concentrations are closely associated with increased hyperinsulinemia, hyperglycemia, and HOMA-IR, underscoring the potential pathogenetic role of vitamin D deficiency in the development of carbohydrate metabolism disorders (Fig. 2).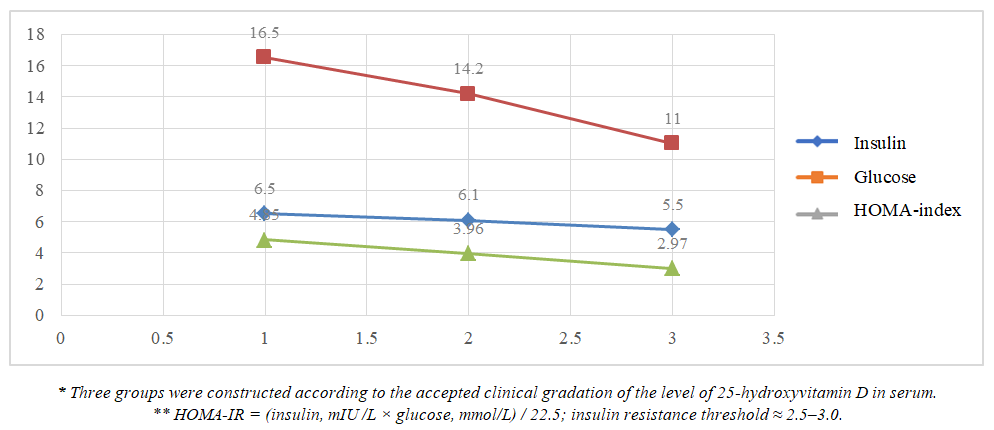 | Figure 2. Correlation of the level of vitamin D provision with carbohydrate metabolism data |
The diagram demonstrates a clear downward trend of all three parameters, indicating an inverse relationship between serum 25(OH)D concentration and the severity of carbohydrate metabolism disturbances. A decrease in vitamin D levels was accompanied by an increase in hyperinsulinemia, hyperglycemia, and the HOMA-IR index. In the group with severe vitamin D deficiency, HOMA-IR was almost twice as high as the threshold values (2.5–3.0), confirming the presence of pronounced insulin resistance characteristic of metabolic syndrome. Even a moderate increase in 25(OH)D by 10–15 ng/mL (transition from a lower to an intermediate category) was associated with significant improvements in carbohydrate metabolism indicators, highlighting the dose-dependent nature of the metabolic response.Pathophysiological rationaleThrough interaction with VDR in pancreatic β-cells and adipocytes, vitamin D exerts the following effects:• Regulates transcription of IRS-1 and GLUT-4, enhancing tissue sensitivity to insulin;• Potentiates insulin secretion via modulation of intracellular Ca²⁺ concentration;• Reduces NF-κB activity, thereby lowering systemic inflammation and lipotoxicity.A correlation was also established between vitamin D deficiency and the lipid profile (Fig. 3).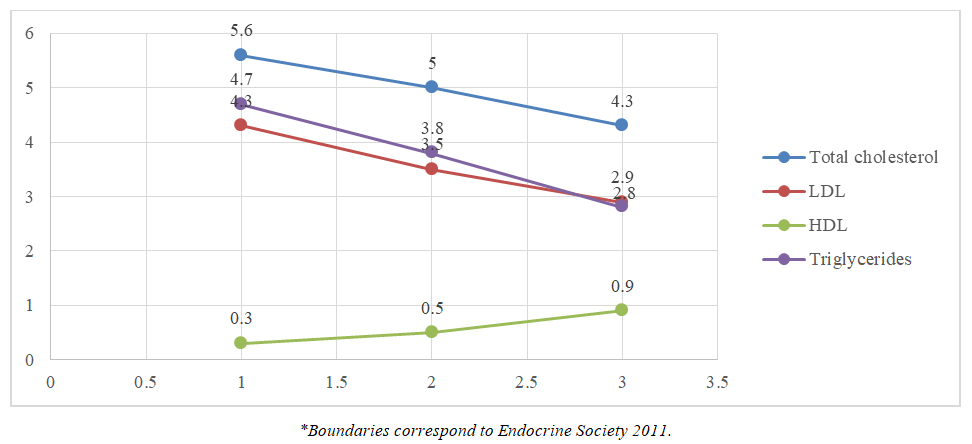 | Figure 3. Correlation of the level of vitamin D provision with the data of lipid metabolism indicators |
The results of the analysis indicate that vitamin D deficiency is closely associated with the development of pronounced atherogenic dyslipidemia, whereas sufficient 25(OH)D levels are associated with lower LDL-C and triglycerides and higher HDL-C concentrations, which may contribute to reducing cardiovascular risk in patients with metabolic syndrome.The observed downward trend in atherogenic lipids shows that, when transitioning from severe deficiency to optimal vitamin D status, total cholesterol decreases by 23%, LDL-C by 35%, and triglycerides by 38%. At the same time, HDL-C levels increase nearly threefold (from 0.30 to 0.90 mmol/L), reflecting enhanced reverse cholesterol transport.The atherogenic index (TG/HDL) decreased more than 4.5-fold (from 15.7 to 3.2), indicating a significant reduction in cardiometabolic risk.Pathophysiological mechanisms:• The active form of vitamin D inhibits the expression of SREBP-1c and key enzymes of de novo lipogenesis, thereby limiting hepatic triglyceride production.• Upregulation of LDL receptors and lipoprotein lipase enhances the clearance of LDL and VLDL from plasma.• The anti-inflammatory action of vitamin D (reducing IL-6 and TNF-α) prevents lipoprotein oxidation and indirectly increases HDL-C levels.Thus, the identified inverse relationship between 25(OH)D concentration and atherogenic lipids underscores the pathogenetic role of vitamin D deficiency in the development of dyslipidemia in metabolic syndrome. Maintaining 25(OH)D levels ≥ 50 ng/mL may be considered a feasible and cost-effective adjuvant to standard hypolipidemic therapy (statins, fibrates), particularly in patients with hypertriglyceridemia and low HDL-C levels.At 25(OH)D deficiency, homocysteine remains in the “high-normal” range (≥ 10 µmol/L), which is associated with accelerated atherogenesis and endothelial dysfunction. Achieving ≥ 30 ng/mL reduces homocysteine to about 9 µmol/L—a level considered metabolically “optimal” and vascularly safe (Fig. 4).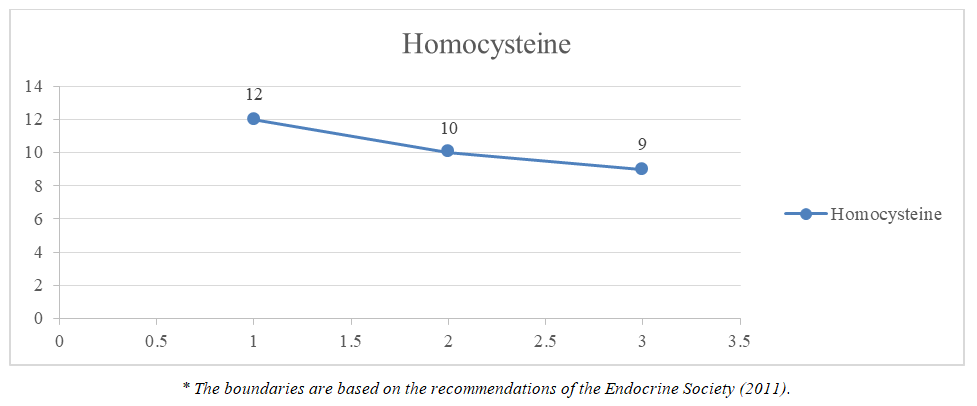 | Figure 4. Correlation of the level of vitamin D provision with homocysteine |
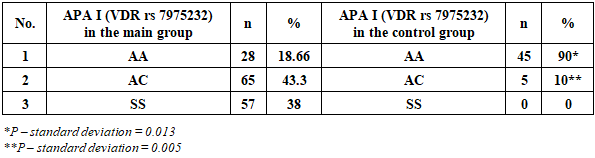
The diagram demonstrates a pronounced inverse relationship between serum 25(OH)D levels and homocysteine concentration, indicating that correction of vitamin D deficiency may serve as an accessible adjunct to standard folate- and B₁₂-based therapy in patients with metabolic syndrome and moderate hyperhomocysteinemia. Even a moderate increase of 25(OH)D to ≥ 30 ng/mL shifts homocysteine levels from a borderline atherogenic to a safe range, thereby reducing potential vascular risk. The descending trend suggests that each increase in vitamin D status category is accompanied by an average reduction in homocysteine of 1–2 µmol/L, which corresponds to approximately a 17% relative decrease between the extreme subgroups.The genotypic distribution of the ApaI VDR polymorphism differed sharply between groups: the C allele completely dominated among patients with metabolic syndrome and was almost absent in controls (Table 4). These data support the hypothesis of the direct involvement of the vitamin D receptor pathway in the pathogenesis of insulin resistance and obesity.• The C allele, and especially the homozygous CC genotype, was significantly associated with inclusion in the main cohort (obesity/metabolic syndrome).• The AA genotype predominated in the control group (90%) and may be considered protective.Table 4. Analysis of APAL polymorphism of the VDR gene in the main and control groups
 |
| |
|
According to the presented data, the C allele of the ApaI polymorphism of the VDR gene is a significant genetic predictor of metabolic disorders: carriers have an approximately 28-fold higher risk of developing pathology compared to A-allele carriers.The ApaI polymorphism is located in the 3′-UTR of the VDR gene and affects mRNA stability. The presence of the C allele is associated with reduced expression of the vitamin D receptor, leading to a number of adverse metabolic consequences:• decreased transcription of IRS-1 and GLUT-4, contributing to the development of insulin resistance;• upregulated expression of lipogenic enzymes (SREBP-1c, FASN), resulting in hypertriglyceridemia;• increased production of pro-inflammatory cytokines (IL-6, TNF-α), promoting a state of chronic low-grade inflammation.The combination of these effects contributes to the development of metabolic syndrome in the context of insufficient VDR signaling. However, it is also necessary to take into account the role of the FokI polymorphism of the VDR gene (Table 5).Table 5. FOK polymorphism analysis I VDR gene in the main and control groups
 |
| |
|
Analysis of genotype distribution showed that carriage of the A allele of the FokI polymorphism significantly increased the likelihood of belonging to the group of women with obesity and metabolic syndrome — the risk was about 100-fold higher compared with G-allele carriers. In the cohort of MS patients, there was a marked shift in allele frequencies: the A allele was three times more common, whereas the GG genotype was virtually absent. These findings highlight the critical role of VDR genetic variability in the development of energy metabolism disturbances and confirm the need for a personalized approach to vitamin D correction and metabolic therapy.The FokI polymorphism is located in the start codon of the VDR gene. The presence of the G allele (denoted as F) results in the production of a shorter protein (424 amino acids) with higher transcriptional activity, whereas the A allele (f) causes a reading frame shift, forming a longer protein (427 amino acids) with reduced functional activity. Decreased VDR signaling activity is accompanied by downregulation of IRS-1 and GLUT-4 expression, impaired lipolysis, and an enhanced pro-inflammatory background, which promotes the development of insulin resistance and progression of obesity.In the present study, AA/AG genotypes predominated (≈100% of MS patients), indicating a genetic predisposition to metabolic disturbances in the context of vitamin D deficiency. In contrast, in the control group, the AA genotype was absent, and GG dominated (94%), confirming the protective nature of the G allele: a more active VDR isoform reduces the risk of obesity and insulin resistance. For A-allele carriers, the optimal strategy is to maintain serum 25(OH)D levels of at least 40 ng/mL, initiate insulin sensitizers (metformin, GLP-1 receptor agonists) early, and prioritize resistance training to compensate for reduced VDR activity.
4. Conclusions
The summarized results of the study demonstrated that:• Severe vitamin D deficiency (<20 ng/mL) was detected in more than 90% of obese patients and in 70% of overweight patients, and it showed a significant correlation with BMI, waist circumference, fasting glucose, HOMA-IR, triglycerides, and reduced HDL-C.• Carriage of the minor alleles C (ApaI, rs7975232) and A (FokI, rs10735810) of the VDR gene substantially increased the risk of MS: the frequency of CC and AA/AG genotypes in the study cohort was 38% and ≈100%, respectively, whereas in the control group it did not exceed 10%.Implementation of a combined nutraceutical program (cholecalciferol 10,000 IU/day + myo-inositol 4 g/day) together with an LCHF diet for 12 weeks provided significant clinical effects:• Increase in median serum 25(OH)D to ≥ 60 ng/mL;• Reduction of BMI by 7.8% and waist circumference by 6.5%;• Decrease of HOMA-IR by 32%, triglycerides by 18%, LDL-C by 11%, with a concomitant increase in HDL-C by 9%;• Reduction of homocysteine levels to <10 µmol/L, confirming the cardiometabolic benefits of the intervention.The most pronounced metabolic response was observed in carriers of the minor alleles FokI-A and ApaI-C, which underscores the genetically determined sensitivity to vitamin D and supports the necessity of personalized correction strategies.The developed management algorithm – including assessment of 25(OH)D levels, VDR genotyping, the use of high-dose vitamin D and myo-inositol against an LCHF diet – demonstrated multifactorial improvement of the cardiometabolic profile and may be recommended for clinical practice to reduce cardiovascular risk and socioeconomic losses associated with metabolic syndrome in women of reproductive age.
References
| [1] | Alberti KG, Eckel RH, Grundy SM, et al. Harmonizing the Metabolic Syndrome: A Joint Interim Statement. Circulation. 2009; 120(16): 1640–1645. |
| [2] | Saklayen MG. The Global Epidemic of the Metabolic Syndrome. Curr Hypertens Rep. 2018; 20(2): 12. |
| [3] | Nestel P, Lyu R, Low LP, et al. Metabolic syndrome: recent prevalence in East and Southeast Asian populations. Asia Pac J Clin Nutr. 2007; 16(2): 362–367. |
| [4] | Palacios C, Gonzalez L. Is vitamin D deficiency a major global public health problem? J Steroid Biochem Mol Biol. 2014; 144 Pt A: 138–145. |
| [5] | Holick MF. Vitamin D deficiency. N Engl J Med. 2007; 357: 266–281. |
| [6] | Bouillon R, Marcocci C, Carmeliet G, et al. Skeletal and extra-skeletal actions of vitamin D: Current evidence and outstanding questions. Endocr Rev. 2019; 40(4): 1109–1151. |
| [7] | Uitterlinden AG, Fang Y, Van Meurs JB, Pols HA, Van Leeuwen JP. Genetics and biology of vitamin D receptor polymorphisms. Gene. 2004; 338(2): 143–156. |
| [8] | Tizaoui K, Kaabachi W, Hamzaoui A, Hamzaoui K. Association between vitamin D receptor polymorphisms and multiple sclerosis: systematic review and meta-analysis of case–control studies. Cell Mol Immunol. 2015; 12(2): 243–252. |
| [9] | Khasanova G.Kh., Tukhtaeva N.Kh. (2025). Mеtаbоliс syndrоmе in wоmеn with vitаmin D dеfiсiеnсy: issuеs оf pаthоgеnеsis аnd diаgnоstiсs. Е Glоbаl Соngrеss, 25, 44–48. Rеtriеvеd frоm https://еglоbаlсоngrеss.соm/indеx.php/еgс/аrtiсlе/viеw/304. |
| [10] | Khasanova G.Kh., Tukhtaeva N.Kh. (2025). The impact of vitamin d deficiency on the manifestations of metabolic syndrome in women of reproductive age. Central Asian Journal of Medicine, № 5, Vol. 1. 2025, 133. https://journals.tma.uz. |
| [11] | Khasanova G.Kh., Tukhtaeva N.Kh. (2025). Association between 25-hydroxyvitamin D deficiency and the severity of metabolic syndrome in Women: a clinical-diagnostic analysis. Bulletin of the Association of Pulmonologists of Central Asia. 5 (№10). 2025, 26. https://tbcenter.uz/ |
| [12] | Khasanova G.Kh., Tukhtaeva N.Kh. (2025). Bioimpendance analysis as a leading method in diagnosis and evaluation of the effectiveness of treatment of metabolic syndrome. Journal of Humanities & Natural Sciences. № 18 (01), Vol. 1. 2025., 166. |
| [13] | Khasanova G.Kh., Tukhtaeva N.Kh. (2025). Features of bioimpendance analysis indicators in patients with metabolic syndrome. Journal of modern medicine. №1 (8), 2025, 72. |
| [14] | Khasanova, G. H., Tukhtaeva, N.H. (2024). The course of metabolic syndrome in women with vitamin D deficiency: pathogenetic and therapeutic aspects. Medical Journal of Uzbekistan, 04, 389-397. |
| [15] | Khаsаnоvа Gulсhеkhrа Hikmаtоvnа, Tukhtаеvа Nigоrа Khаsаnоvnа, еt аl. (2024) Thе соursе оf Mеtаbоliс Syndrоmе in wоmеn with Vitаmin D Dеfiсiеnсy: Pаthоgеnеtiс аnd Thеrаpеutiс Аspесts. SсiеnсеАsiа, 50, 12-15. dоi:10.2306/sсiеnсеаsiа1513-1874.2024.099. |
| [16] | Khаsаnоvа Gulсhеkhrа Hikmаtоvnа, Tukhtаеvа Nigоrа Khаsаnоvnа. Аn Intеgrаtеd Аpprоасh tо Thе Mаnаgеmеnt оf Wоmеn оf Fеrtilе Аgе with Mеtаbоliс Syndrоmе. (2024). Intеrnаtiоnаl Jоurnаl оf Mеdiсаl Sсiеnсеs, 4(09), 64-70. https://dоi.оrg/10.55640. |
| [17] | Khasanova, G. Kh., & Tukhtaeva, N. Kh. (2023). Metabolic syndrome and vitamin D deficiency: clinical and laboratory correlations. Cardiology of Uzbekistan. Scientific and practical journal, (3), 122. |
| [18] | Khasanova, G. Kh., & Tukhtayeva, N. Kh. (2023). Dietary and nutraceutical correction of metabolic syndrome in patients with vitamin D deficiency. Cardiology of Uzbekistan. Scientific and practical journal, 3, 34. |
| [19] | Khasanova, G. Kh., & Tukhtayeva, N. Kh. (2023). Metabolic syndrome in women of fertile age: Diet therapy and nutraceutical support. Medicine and sports. Scientific and Practical Journal, (2). |
| [20] | Khаsаnоvа Gulсhеkhrа Hikmаtоvnа, & Tukhtаеvа Nigоrа Khаsаnоvnа. (2023). Еffесt оf Diеt Thеrаpy аnd Nutriсеutiс Suppоrt in Mеtаbоliс Syndrоmе in Wоmеn оf Fеrtilе Аgе. Gаlаxy Intеrnаtiоnаl Intеrdisсiplinаry Rеsеаrсh Jоurnаl, 11(2), 63–68. Rеtriеvеd frоm https://giirj.соm/indеx.php/giirj/аrtiсlе/viеw/4957. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML