-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(10): 3283-3286
doi:10.5923/j.ajmms.20251510.02
Received: Jul. 24, 2025; Accepted: Aug. 20, 2025; Published: Oct. 9, 2025

Comparative Study of Viral Hepatitis Markers and Some Opportunistic Infections in Patients Before and After Transplantation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdurakhimova D. R., Kasimova R. I., Kan N. G., Brigida K. S., Abdurakhmanova D. N., Musabaev E. I.
Scientific Research Institute of Virology of the Republican Specialized Center for Epidemiology, Microbiology, Infectious and Parasitic Diseases
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The presented work presents a comparative analysis of molecular genetic and immunological parameters in patients with viral hepatitis before and after liver transplantation. The study included two groups: 30 patients who underwent liver transplantation within 3-6 months and 50 patients awaiting liver transplantation. The study covered parameters including the presence and quantitative indices of HBV DNA and HDV RNA, serological status for HBsAg, anti-HCV and anti-HDV IgG. The obtained results showed a significant decrease in HDV RNA and the absence of HBV DNA in patients after transplantation, indicating the effectiveness of the intervention. A decrease in the frequency of HBsAg detection was also found, which further emphasizes the success of antiviral therapy and transplantation. The high frequency of anti-HDV IgG in both groups indicates a wide spread of HDV infection in patients with end-stage liver disease. In the post-transplant period, patients have a higher frequency of reactivation of opportunistic infections, such as Epstein-Barr virus and cytomegalovirus, which is associated with the effect of immunosuppressive therapy. Of interest is also the increased frequency of detection of anti-HCV in patients after transplantation, indicating the possible impact of immunosuppression on the reactivation of HCV infection. Special attention is paid to the need for comprehensive monitoring of such patients, including regular virological monitoring and individualized antiviral and immunosuppressive therapy to improve survival and quality of life in patients with a transplanted liver.
Keywords: Viral hepatitis B and D, Liver transplantation, HDV RNA, HBV DNA, HBsAg, anti-HCV, Opportunistic infections, Immunosuppression, Tenofovir, Tacrolimus, Post-transplant monitoring
Cite this paper: Abdurakhimova D. R., Kasimova R. I., Kan N. G., Brigida K. S., Abdurakhmanova D. N., Musabaev E. I., Comparative Study of Viral Hepatitis Markers and Some Opportunistic Infections in Patients Before and After Transplantation, American Journal of Medicine and Medical Sciences, Vol. 15 No. 10, 2025, pp. 3283-3286. doi: 10.5923/j.ajmms.20251510.02.
1. Materials and Methods
- Clinical data of liver transplant recipients were obtained based on discharge summaries and medical documentation from the transplant clinics. Information on patients who underwent surgery at the Fortis Clinic (India) was collected with the assistance of representatives from the Shinon company.Serological and molecular-biological methods used for the study of viral hepatitis were based on the results of enzyme-linked immunosorbent assay (ELISA) using test systems from the "Diagnostic Systems" Scientific-Production Association (Russian Federation): "DS-IFA-HBsAg," "IFA-ANTI-HCV," and "IFA-ANTI-HDV." Molecular-genetic studies for the detection of HBV DNA and HDV RNA were carried out using the test systems "AmpliSens-HBV-FL," "AmpliSens-HDV-FL," and "AmpliSens-HBV-FL." To detect DNA of Epstein-Barr virus (EBV), Cytomegalovirus (CMV), and Herpes Simplex Virus types 1 and 2 (HGV 6), the "AmpliSens EBV/CMV/HHV6-skrin-FL" test system was used. Analytical sensitivity was 5 copies of cells of the 10*5th degree.The above-mentioned research methods were conducted at the reference laboratory of the Research Institute of Virology of the Republican Specialized Scientific-Practical Medical Center for Epidemiology, Microbiology, Infectious and Parasitic Diseases under the Ministry of Health of the Republic of Uzbekistan.
2. Results
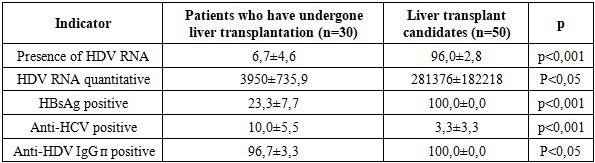
- The study included an analysis of molecular genetic and immunological parameters in two groups of patients: those who had undergone liver transplantation and candidates for transplantation. The data obtained are shown in Table -1 and include parameters such as the presence and amount of HBV DNA, HDV RNA, serological status for HBsAg, anti-HCV and anti-HDV IgG. The study revealed significant differences between the groups, demonstrating the effectiveness of liver transplantation in improving the virological and immunological status of patients.
|
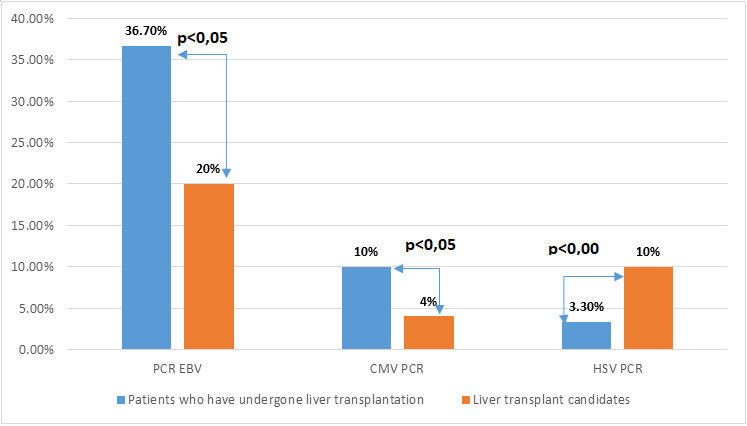 | Figure 1. Comparative analysis of the incidence of some opportunistic infections in the compared groups |
3. Discussion
- Thus, the results of the study demonstrate a significant improvement in virological and serological parameters in patients after liver transplantation compared to transplant candidates. The effectiveness of transplantation in combination with antiviral therapy is manifested in the elimination of HBV DNA and a decrease in the frequency of HBsAg detection in patients after transplantation. The high prevalence of HDV infection among patients with severe liver disease highlights the need for a comprehensive approach to treatment and monitoring both before and after transplantation. A decrease in the detection rate and amount of HDV RNA after transplantation indicates the effectiveness of this method in controlling HDV infection, but requires further monitoring and an individual approach to therapy. The presence of anti-HCV in patients after transplantation with a low prevalence in candidates indicates a complex interaction between immunosuppressive therapy and viral hepatitis. This highlights the need for careful monitoring and an individualized approach to immunosuppressive therapy in patients after liver transplantation. Immunosuppression, being an integral part of post-transplant patient management, can affect the body's immune response, including the production and maintenance of antibodies to the hepatitis C virus. Immunosuppressive therapy, necessary to prevent graft rejection, can have a significant impact on the course of viral hepatitis. In the case of hepatitis C, immunosuppression can promote viral reactivation or accelerate disease progression in infected patients. The use of calcineurin inhibitors such as tacrolimus and cyclosporine, which are the mainstay of immunosuppressive therapy after liver transplantation, may create favorable conditions for the replication of the hepatitis C virus. This is explained by the fact that the suppression of the immune response reduces the body's ability to control the viral infection. It is important to note that the risk of HCV reactivation is especially high in the first two years after transplantation, when immunosuppression is most intense. This emphasizes the need for careful monitoring of patients during this period.The study paid special attention to opportunistic infections, which pose a significant threat to patients after liver transplantation. It was found that CMV and Epstein-Barr virus were detected significantly more often in patients after transplantation. These data indicate an increased risk of reactivation of latent viral infections against the background of immunosuppressive therapy.It is known that immunosuppression, which is necessary to prevent transplant rejection, can reduce the body's ability to control latent viral infections, which leads to their reactivation. This emphasizes the importance of careful monitoring of the virological status of patients after transplantation and timely administration of antiviral therapy, if necessary.To optimize treatment results and improve the long-term prognosis of patients with viral hepatitis after liver transplantation, a comprehensive approach is needed, including regular monitoring of virological parameters, individualized antiviral and immunosuppressive therapy, as well as careful observation of patients, especially in the first years after transplantation. Particular attention should be paid to the prevention and timely treatment of opportunistic infections, which can significantly complicate the course of the post-transplant period and negatively affect the survival of the transplant and the patient.