-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3269-3278
doi:10.5923/j.ajmms.20251509.94
Received: Aug. 22, 2025; Accepted: Sep. 21, 2025; Published: Sep. 30, 2025

Molecular-Genetic Predictors of Atrial Fibrillation in Patients with Arterial Hypertension in the Uzbek Population
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdullaeva G. Zh.1, Mashkurova Z. T.1, Zakirova D. V.2, Radzhabova G. M.1, Yusupova Kh. F.1, Ibragimov N. N.1, Abdullaev A. A.2
1Republican Specialized Scientific and Practical Medical Center of Cardiology, Tashkent, Uzbekistan
2Center for Advanced Technologies, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

To investigate the association between polymorphisms of the PITX2 (rs6817105), CAV1 (rs11773845, rs3807990), and KCNN3 (rs13376333) genes and the development of atrial fibrillation (AF) in patients with arterial hypertension (AH) in the Uzbek population. The study included 154 patients with AH who were initially diagnosed with paroxysmal AF (n = 21; 13.64%), persistent AF (n = 44; 28.57%), and permanent AF (n = 89; 57.79%). The mean age of patients with AH and AF at baseline was 64.1 ± 10.35 years. The control group (n = 91) consisted of patients with AH without AF, with a mean age of 56.03 ± 12.18 years. Clinical and instrumental examinations were performed (ECG, echocardiography, Holter monitoring), as well as molecular genetic analysis of extracted DNA using real-time PCR. Associations between polymorphisms and AF were evaluated using logistic regression and different inheritance models. Statistical analysis was performed with Statistica 10.0 and SNPassoc (R). Statistically significant associations were identified between several polymorphisms and the risk of atrial fibrillation in patients with arterial hypertension in the Uzbek population. The rs6817105 polymorphism of the PITX2 gene demonstrated a strong association with AF: carriage of the minor C allele increased the risk of AF 2.76-fold (OR = 2.76; p = 3.27×10⁻⁷) under the log-additive inheritance model. For rs11773845 of the CAV1 gene, an association was found at both the allele and genotype levels: presence of the A allele (p = 6.22×10⁻¹¹) and the heterozygous AC genotype (OR = 2.43; p = 0.001) significantly increased the likelihood of AF. Interestingly, analysis of rs3807990 of the same CAV1 gene revealed the opposite effect: carriage of the C allele was associated with a reduced risk of AF (OR = 0.71; p = 0.049), suggesting a potential protective role. Finally, the rs13376333 polymorphism of the KCNN3 gene also showed a significant association with AF: the C allele was more frequent in patients with rhythm disturbances, increasing AF risk (OR = 1.63; p = 0.020) under the log-additive model. These findings confirm the role of the studied genetic markers in the pathogenesis of atrial fibrillation in patients with arterial hypertension and highlight the importance of genetic testing in this group of patients. The present data demonstrate, for the first time, associations of several single nucleotide polymorphisms with atrial fibrillation in patients with arterial hypertension in the Uzbek population. These results emphasize the importance of integrating molecular genetic markers into clinical practice for personalized risk assessment and prevention of cardiac arrhythmias.
Keywords: Arterial hypertension, Atrial fibrillation, PITX2 rs6817105 polymorphism, CAV1 rs11773845 polymorphism, CAV1 rs3807990 polymorphism, KCNN3 rs13376333 polymorphism
Cite this paper: Abdullaeva G. Zh., Mashkurova Z. T., Zakirova D. V., Radzhabova G. M., Yusupova Kh. F., Ibragimov N. N., Abdullaev A. A., Molecular-Genetic Predictors of Atrial Fibrillation in Patients with Arterial Hypertension in the Uzbek Population, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3269-3278. doi: 10.5923/j.ajmms.20251509.94.
1. Introduction
- Atrial fibrillation (AF) is one of the most common arrhythmias, associated with high morbidity and mortality. According to the European Society of Cardiology, the prevalence of AF in the adult population ranges from 1% to 4%, with the rate increasing with age, reaching 10–15% among individuals over 80 years old [1]. AF significantly increases the risk of stroke, heart failure, and cognitive impairment, making the study of factors influencing its development critically important. In addition to traditional risk factors such as age, arterial hypertension (AH), obesity, and diabetes mellitus, genetic factors play a substantial role in the pathogenesis of AF. Current research suggests that up to 40% of AF cases may be attributable to hereditary predisposition, and one of the key directions in cardiogenetics is the study of single nucleotide polymorphisms (SNPs) that affect the structural and electrophysiological properties of the atria [2]. Particular interest lies in the study of AF in patients with AH, since hypertension is one of the main predisposing factors for the development of this arrhythmia. However, not all patients with AH develop AF, indicating a significant role of genetic predisposition. Studies conducted among various ethnic groups have demonstrated that the prevalence of AF-associated polymorphisms varies depending on racial and ethnic background. The Uzbek population was formed under the influence of Central Asian, Iranian, Turkic, and Mongoloid ethnic groups, which may have led to an altered frequency of specific SNPs affecting cardiovascular diseases [3]. However, data on AF in the Uzbek population are virtually absent, despite its unique features shaped by genetic factors. Analysis of the literature from European, Chinese, and other populations has identified several polymorphic variants of genes associated with AF risk. In particular, the rs13376333 polymorphism of the KCNN3 gene, which encodes small-conductance calcium-activated potassium channels (SK3), has been identified as a risk factor for AF. A study in the Han Chinese population showed that the T allele of rs13376333 was significantly more frequent in patients with AF compared to the control group (7.6% vs. 3.6%; p < 0.001), confirming its importance as a potential marker of arrhythmia susceptibility [4]. Furthermore, a meta-analysis including 24,339 participants confirmed that this SNP increases the risk of overall AF (OR = 1.33) and lone AF (OR = 1.58) [5]. Another important genetic biomarker is the rs6817105 polymorphism of the PITX2 gene, located on chromosome 4q25, which has been identified as one of the most significant predictors of AF. This SNP influences the development of the cardiac conduction system, left atrial morphology, and sinus node function. According to Tomomori et al. [6], the minor allele of rs6817105 increases AF risk more than twofold (OR = 2.12; p = 4.9×10⁻²⁶). Importantly, the frequency of this polymorphism varies among different ethnic groups, and its investigation in the Uzbek population will help determine its clinical significance in this cohort. Another promising marker is the rs3807990 variant of the CAV1 gene, which encodes caveolin-1, a protein involved in the regulation of vascular tone, lipid metabolism, and inflammatory processes. A study conducted in 2019 showed that this SNP is associated with hypercholesterolemia and endothelial dysfunction, potentially contributing to the development of AH and AF [7]. In turn, the rs11773845 polymorphism in the same gene was linked to metabolic syndrome and elevated triglyceride levels in the Latin American population, highlighting its possible relevance to cardiovascular disease development in other ethnic groups as well [8]. The genetic predisposition to AF has also been confirmed by Sasano et al. [2], who identified that SNPs rs6817105, rs3807989, rs10824026, and rs2106261 can be used for AF and stroke risk stratification. Their risk prediction model demonstrated an AUC = 0.631 for AF and an AUC = 0.950 for stroke, indicating high predictive value of these polymorphisms. Given the high prevalence of AH in Uzbekistan and the lack of molecular genetic research on AF-associated markers in this population, there is a strong need for local studies aimed at identifying genetic predictors of AF in hypertensive patients in the Uzbek population.
2. Materials and Methods
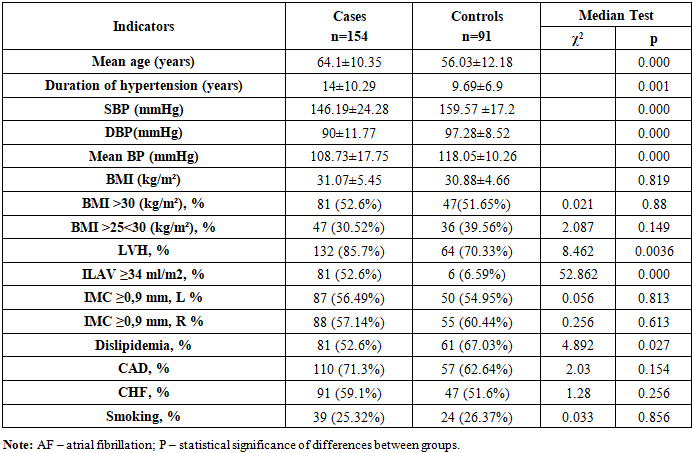
- The study included 154 patients with arterial hypertension (AH), in whom atrial fibrillation (AF) was initially diagnosed as paroxysmal in 21 cases (13.64%), persistent in 44 cases (28.57%), and permanent in 89 cases (57.79%). The mean age of AH patients with AF at baseline was 64.1 ± 10.35 years (Table 1). The control group (n = 91) consisted of AH patients without AF, with a mean age of 56.03 ± 12.18 years. As shown in Table 1, patients with AH and AF differed from the control group in terms of age, duration of hypertension, and office blood pressure measurements. Notably, the age of AH patients with AF was significantly higher compared with the control group: 64.1 ± 10.35 years versus 56.03 ± 12.18 years (p = 0.000). The duration of hypertension was also longer in the AF group than in the control group, amounting to 14.0 ± 10.29 years versus 9.69 ± 6.9 years, respectively (p = 0.001). The number of patients with left ventricular hypertrophy (LVH) was significantly higher in the AH + AF group than in AH patients without AF: 132 (85.7%) versus 64 (70.33%) (χ² = 8.462, p = 0.0036). It is important to note that the proportion of patients with left atrial volume index (LAVI) ≥ 34 ml/m² was substantially greater among AH patients with AF compared with those without AF: 52.6% versus 6.59%, respectively (χ² = 52.862, p = 0.000). It should be noted that the two groups did not differ in the number of patients with CAD and CHF.
|
3. Results
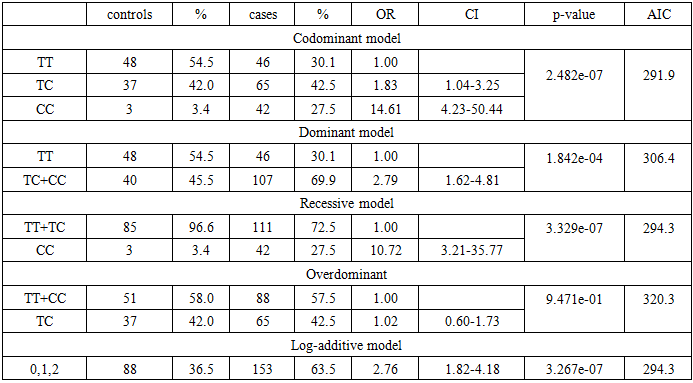
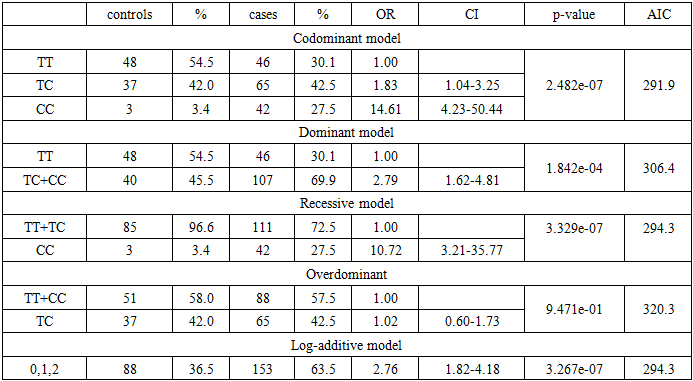
- A total of 154 hypertensive patients with atrial fibrillation (cases) and 91 hypertensive patients without atrial fibrillation (controls), all from the Uzbek population, were genotyped. Below are the results of molecular-genetic analysis and the determination of correlations between genetic markers and the case and control groups using the statistical method of logistic regression. An analysis of the distribution of allele and genotype frequencies was conducted for the following gene polymorphisms involved in the development of atrial fibrillation in hypertensive patients in the Uzbek population: rs6817105 polymorphism of the PITX2 gene, rs11773845 polymorphism of the CAV1 gene, rs3807990 polymorphism of the CAV1 gene, and rs13376333 polymorphism of the KCNN3 gene.rs6817105 polymorphism of the PITX2 gene and atrial fibrillationTo study the association of the rs6817105 polymorphism of the PITX2 gene with atrial fibrillation in hypertensive patients, 153 hypertensive patients with AF (cases) and 88 hypertensive patients without AF (controls), all from the Uzbek population, were genotyped. When analyzing the distribution of genotype and allele frequencies of the rs6817105 polymorphism of the PITX2 gene among hypertensive patients with AF, the following genotype distribution was observed: TT genotype – identified in 46 (30.1%) patients, TC genotype – in 65 (42.5%), CC genotype – in 42 (27.5%), χ2=8.882, p=0.012 (Table 2). The allelic distribution was nearly equal: T allele – 51.3%, C allele – 48.7%, χ2=0.320, p=0.571. The opposite pattern was observed among hypertensive patients without AF. In particular, the allelic distribution showed a significant predominance of the T allele compared with the C allele: 75.6% versus 24.4%, respectively, χ2=90.011, p=0.000. The genotype ratio TT:TC:CC was as follows: 54.5% : 42.0% : 3.4%, χ2=56.284, p=0.000. Thus, the obtained results indicate a significantly greater accumulation of the T allele and TT genotype of the rs6817105 polymorphism of the PITX2 gene among hypertensive patients without AF compared with hypertensive patients with AF, in whom, on the contrary, the C allele prevailed.
|

|
|

|
|

|
|

|
4. Discussion
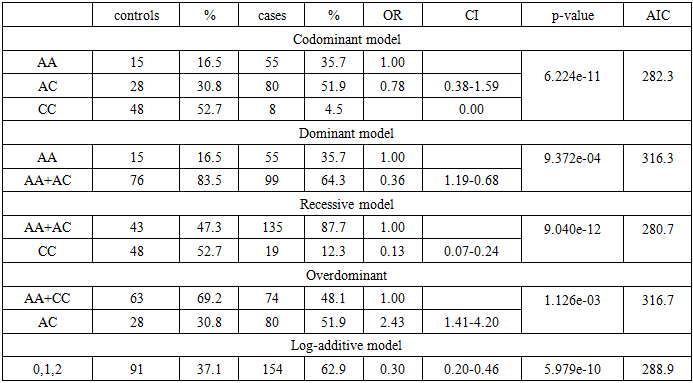
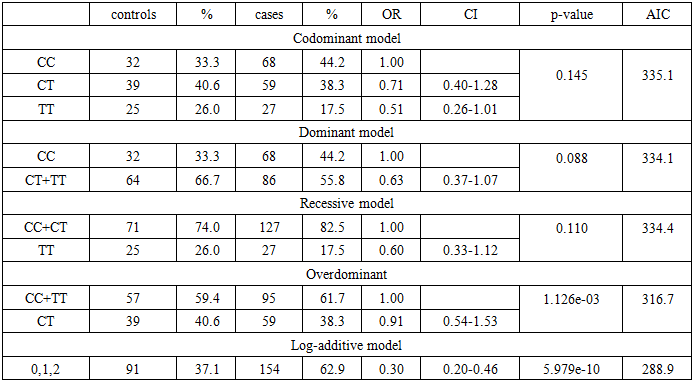
- It is well known that hypertension (HTN) contributes to the development of cardiac rhythm disturbances, in particular ventricular arrhythmias, but most frequently atrial fibrillation [14], which represents a manifestation of hypertensive cardiomyopathy [15]. Even high-normal blood pressure is associated with an increased risk of AF [16], and HTN is the most common comorbid diagnosis in patients with AF.Altered geometry of the left ventricle (LV) is often associated with diastolic dysfunction [17, 18]. Enlargement of the left atrium (LA) is also frequently observed in patients with HTN, which is associated with adverse cardiovascular outcomes [19, 20], an increased incidence of AF [21], and diastolic dysfunction [22, 23]. In the present study, the age-dependent nature of AF development in patients with HTN was confirmed, as well as the undeniable influence of the duration of HTN, which is associated with the severity of cardiovascular remodeling. Specifically, in the group of hypertensive patients with AF compared to controls without AF, a significantly higher number of cases of left ventricular hypertrophy (LVH) and increased left atrial volume index (LAVI) were observed.To elucidate the genetic mechanisms of electrophysiological disturbances of the myocardium in HTN, various genes encoding key physiological systems were investigated. The literature describes mutations in the cardiac sodium channel gene (SCN5A) and in KCNQ genes, which may cause rhythm disturbances, including AF. Over the past decade, several genome-wide association studies (GWAS) have identified the ATFB5 gene with the rs2200733 single-nucleotide polymorphism at locus 4q25 as the most common chromosomal variant present in patients with AF [24]. In our previous study, we analyzed the potential relationship between rs2200733 (ATFB5) and the development of AF in individuals of Uzbek nationality [25]. The distribution of genotypes and alleles of rs2200733 among all enrolled patients coincided with results from previous studies conducted in various European countries [26, 27]. Our findings were consistent with the results of a meta-analysis [28] and indicated a significant association between the rare mutant variant (TT genotype) and a fourfold increased risk of AF. In the present study, we examined associations with polymorphisms most pathognomonic for AF, as described in the literature: rs6817105 of the PITX2 gene, rs11773845 of the CAV1 gene, rs3807990 of the CAV1 gene, and rs13376333 of the KCNN3 gene. We identified associations of:- C allele (OR = 2.76, 95% CI: 1.82–4.18, p = 3.267e-07) and CC genotype (OR = 1.02, 95% CI: 0.60–1.73, p = 0.947) of rs6817105 (PITX2);- AC genotype (OR = 2.43, 95% CI: 1.41–4.20, p = 1.126e-03) and A allele (OR = 1.00, p = 6.224e-11) of rs11773845 (CAV1);- C allele of rs3807990 (CAV1) (OR = 0.71, 95% CI: 0.51–1.00, p = 0.049);- C allele (OR = 1.63, 95% CI: 1.07–2.50, p = 0.020) and CC genotype (OR = 1.00, p = 0.023) of rs13376333 (KCNN3).with the risk of atrial fibrillation in hypertensive patients of the Uzbek population. The present study, aimed at identifying molecular–genetic markers of AF in hypertensive patients, has high scientific and practical significance. The data obtained allow us to refine the prevalence of SNPs associated with AF in this population, as well as their contribution to the development of arrhythmias in hypertensive patients. This may contribute to the development of custom genetic panels for AF risk assessment, optimization of treatment strategies, and implementation of a personalized approach to the therapy of hypertensive patients with a predisposition to AF. The introduction of modern genetic technologies into clinical practice will make it possible to more accurately assess the risk of arrhythmias in patients and to apply preventive measures to reduce morbidity and mortality associated with this rhythm disorder.
5. Conclusions
- This study is the first to demonstrate associations of the C allele and CC genotype of rs6817105 (PITX2), the AC genotype and A allele of rs11773845 (CAV1), the C allele of rs3807990 (CAV1), and the C allele and CC genotype of rs13376333 (KCNN3) with the risk of atrial fibrillation in hypertensive patients of the Uzbek population.