Pulatov Oleg Karimovich1, Turaev Feruz Fatxullayevich2
1Independent Researcher of the Karshi Branch of the Republican Specialized Scientific-Practical Medical Center of Cardiology, Uzbekistan
2Cardiac Surgeon of the Republican Specialized Scientific-Practical Medical Center of Surgery named after Academician V. Vakhidov, Uzbekistan
Correspondence to: Pulatov Oleg Karimovich, Independent Researcher of the Karshi Branch of the Republican Specialized Scientific-Practical Medical Center of Cardiology, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Background. Acquired heart valve diseases are often accompanied by left atrial dilatation, which worsens the clinical course of the disease and increases the risk of atrial fibrillation, thromboembolic events, and heart failure. Left atrioplasty, performed in combination with valve surgery, is an effective method to reduce atrial volume and improve postoperative outcomes. Objective. To evaluate the early postoperative course and long-term outcomes of left atrioplasty in patients with acquired heart defects complicated by left atriomegaly. Methods. A prospective clinical study was conducted on patients with acquired heart valve diseases who underwent surgical treatment including left atrioplasty. Patients were divided into groups depending on the surgical technique used (Kawazoe, “Mercedes” modification, and standard valve surgery without atrioplasty). Early postoperative results were assessed using clinical status, echocardiographic and hemodynamic parameters, while long-term outcomes were analyzed based on rhythm disturbances, functional class (NYHA), thromboembolic complications, and survival rate. Results. Early postoperative outcomes demonstrated significant improvement in hemodynamic stability, regression of symptoms, and reduction in left atrial volume in patients who underwent atrioplasty compared to control. In the long-term follow-up, the incidence of atrial fibrillation and thromboembolic events was lower in the atrioplasty group, while functional capacity and quality of life were significantly improved. The effectiveness of atrioplasty was higher in patients with marked atrial dilatation when appropriate surgical techniques were applied. Conclusion. Left atrioplasty in acquired heart defects provides favorable early postoperative recovery and demonstrates long-term clinical benefits. The procedure is especially justified in patients with giant left atrium, as it contributes to improved hemodynamic outcomes, lower arrhythmic complications, and better survival rates.
Keywords:
Acquired heart defects, Left atrioplasty, Left atrial dilatation, Atrial fibrillation, Long-term outcomes, Cardiac surgery
Cite this paper: Pulatov Oleg Karimovich, Turaev Feruz Fatxullayevich, Evaluation of the Early Postoperative Course and Long-Term Outcomes of Left Atrial Atrioplasty in Acquired Heart Defects, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3261-3268. doi: 10.5923/j.ajmms.20251509.93.
1. Introduction
Surgical treatment of mitral valve defects still remains one of the pressing issues in modern cardiac surgery. Damage to the mitral valve leads to enlargement of the left heart chambers, with the left atrium being the first to respond to alterations in valve function. Hemodynamic changes are manifested by compression of the right heart chambers and the vena cava. In addition, left atrial hypertrophy reduces venous return and compresses the posterior-lateral wall of the left ventricle, bronchial tree (airways), and the esophagus, resulting in severe respiratory failure, basal segment atelectasis of the lower lung lobes, dysphagia, and relevant symptoms associated with compression of the descending thoracic aorta.Atriomegaly is considered an important risk factor in the surgical treatment of patients with mitral valve defects. In the early postoperative period, it is often associated with the development of cardiac and pulmonary insufficiency, as well as a high in-hospital mortality rate, which, according to some sources, reaches 20–35%, and according to others, 8–32% [6,9].As a direct consequence of mitral valve lesions, the volume and linear dimensions of the left atrium increase. As a result, the isolated enlargement exceeding the “normal limit” dimensions is compounded by the additional dilation of a previously non-enlarged atrium, leading to worsening of the clinical condition, progression of chronic heart failure, and the development of atrial fibrillation [7,10].Furthermore, an enlarged, especially giant left atrium, serves as a substrate for arrhythmias (paroxysmal or permanent forms). Atrial fibrillation occurs as a complication in 50–80% of cases associated with mitral valve disease [8].Therefore, the issue of enlarged or giant left atrium and the search for optimal surgical correction methods remains relevant. To eliminate the mechanical compression caused by the left atrium, several surgical techniques for reducing atrial volume have been developed, differing in location and method of atrioplasty [1-3]. However, there is no universal technique, and there is no consensus regarding their effectiveness or necessity. Moreover, clear evidence-based recommendations regarding the required degree of atrial reduction are lacking [4,5].Analysis of clinical data and evaluation of the immediate and long-term outcomes of various atrioplasty techniques are of great importance for assessing the effectiveness of surgical methods for reducing left atrial enlargement. In this regard, at the current stage of development of cardiac surgery in our country, it is necessary to improve, develop, and implement modern high-tech diagnostic methods and surgical technologies, as well as to establish approaches for reducing and preventing specific (cardiac surgical) postoperative complications [6–10].Aim of the Study. To evaluate the effectiveness of left atrial volume reduction (atrioplasty) techniques in the surgical correction of heart valve defects complicated by atriomegaly, and to develop approaches for improving surgical outcomes.
2. Materials of the Study
The research was conducted on the basis of the results of 138 surgically treated patients: 94 patients (68.1%) at the Republican Specialized Scientific-Practical Medical Center of Surgery named after Academician V. Vakhidov, and 44 patients (31.9%) at the Karshi branch of the Republican Specialized Scientific-Practical Medical Center of Cardiology.Among them, 108 patients underwent surgical reduction of an enlarged left atrium (LA) simultaneously with correction of mitral valve defects. Depending on the type of atrioplasty performed, patients were divided into two groups:• Group I – atrioplasty according to Kawazoe technique – 94 patients (68.1%);• Group II – atrioplasty according to “Mercedes” modification – 14 patients (10.2%).The control group (Group III) consisted of 30 patients (21.7%) with LA enlargement of more than 5.5–6 cm, who underwent only mitral valve surgery without atrial volume reduction (Figure 1).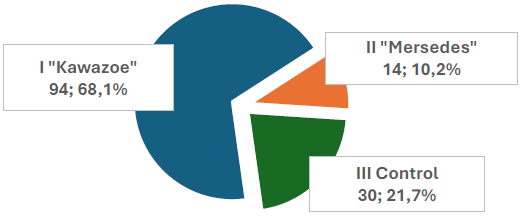 | Figure 1. Distribution of patients by groups |
The mean age of the patients was 44.3 ± 13.3 years (ranging from 13 to 69 years). Gender distribution: 46 (33.4%) males and 92 (66.6%) females. In Group III, the mean age was 41.1 ± 12.7 years (ranging from 17 to 65 years), including 13 (43.33%) males and 17 (56.67%) females.According to the etiology of mitral valve defects, the majority of patients had a long-term history of rheumatic disease – 129 (93.4%), connective tissue dysplasia – 2 (1.5%), and infective endocarditis – 7 (5.1%) (Figure 2).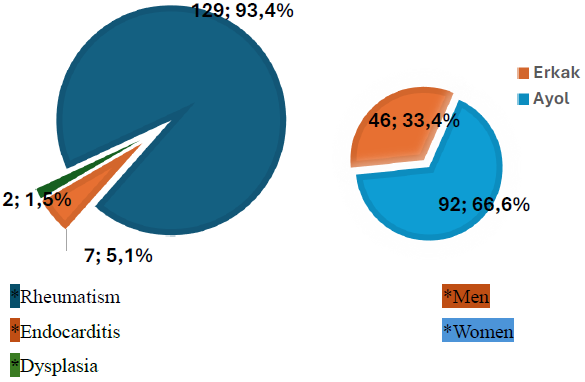 | Figure 2. Distribution of patients by gender and etiology of defects |
All surgical interventions – valve replacement and atrioplasty – in patients with defects showed that the course of the postoperative period largely depended on multiple factors, among which the initial condition of the patient played a leading role.In Group I, postoperative complications occurred in 26 patients (27.7%), while 68 patients (72.3%) had an uneventful recovery. In Group II, complications were observed in 4 patients (28.6%), whereas 10 patients (71.4%) had no complications. The highest rate of complications was recorded in the control group – 26 patients (86.6%), while only 4 patients (13.3%) had an uncomplicated postoperative course.The course of the postoperative period was aggravated by factors such as disease duration, pronounced circulatory decompensation (myocardial dysfunction, changes in systemic and pulmonary circulation), left heart chamber dilatation, the presence of intracardiac infection, hepatic-renal insufficiency, and neurological disorders. The development of postoperative complications was largely determined by the stage of the defect, which was reflected in the increase in complications in accordance with worsening functional class.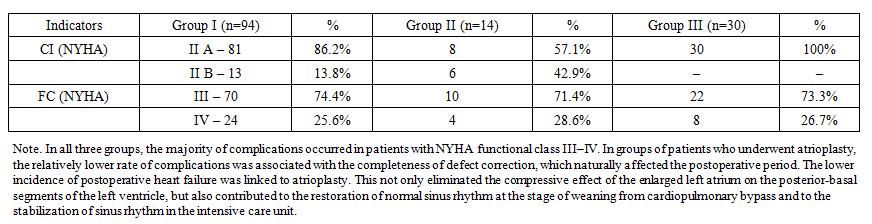 | Table 1. Distribution of patients by circulatory insufficiency (NYHA class) and functional class (FC) |
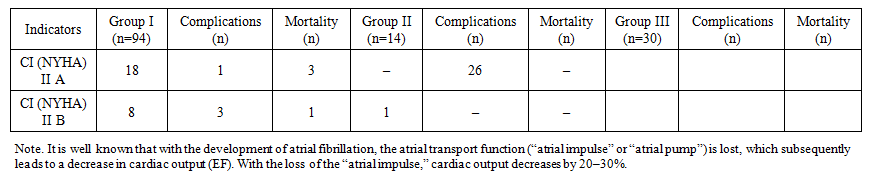 | Table 2. Postoperative complications and mortality by groups |
Restoration of sinus rhythm confirms the theory of the left atrium (LA) contributing up to 20–30% of the stroke volume to cardiac output. Thus, when left ventricular (LV) relaxation is impaired (diastolic dysfunction), especially in patients with long-standing rheumatism and cardiosclerosis, the release of calcium ions from the cytosol (hyaloplasm, i.e., the free portion of cytoplasm) slows down. As a result, the dissociation of actin–myosin cross-bridges within the sarcomeres occurs more slowly, and the suction effect of the LV is significantly weakened.At this stage, ventricular filling becomes increasingly dependent on the augmentation of left atrial contraction – the so-called “atrial pump,” which is 100% effective in sinus rhythm. Due to the “atrial pump,” adequate ventricular filling can be maintained for a prolonged period. A normally functioning left atrium also serves as a buffer, protecting the pulmonary microcirculatory bed and the thin-walled right heart chambers from the negative impact of elevated diastolic pressures associated with LV diastolic dysfunction.Left atrial dysfunction, on the other hand, contributes to increased pulmonary venous pressure during physical activity, which in turn causes dyspnea, pulmonary venous congestion, deterioration of pulmonary function, and the development of pulmonary arterial hypertension. Ultimately, all hemodynamic disturbances associated with left atrial myopathy lead to worsening heart failure, thereby increasing the risk of mortality and hospitalizations.The duration of cardiotonic support in Group I patients averaged 22.3 ± 4.1 hours*, in Group II – 34.5 ± 7.1 hours*, while in the control group it was significantly longer, reaching 57 ± 7.3 hours (*p < 0.05). These findings indicate that the control group required more prolonged cardiotonic support. In this group, the non-reduced enlarged left atrium compressed the basal segments of the left ventricular posterior wall, necessitating longer and more intensive inotropic support to restore contractility.Failure to perform atrioplasty also affected another important postoperative indicator – the duration of mechanical ventilation. The mean duration of respiratory support across all groups was 14.5 ± 1.9 hours. However, in Group I the duration of mechanical ventilation was 10.8 ± 2.2 hours*, in Group II – 13.9 ± 1.8 hours*, while in the control group it was significantly higher at 18.8 ± 1.7 hours* (*p < 0.05). This once again demonstrates that correction of atriomegaly (atrioplasty) improves pulmonary ventilation parameters, facilitates faster recovery of spontaneous breathing, and leads to quicker restoration of respiratory function.Consequently, the length of stay in the intensive care unit (ICU) also differed between groups. In Group I, the average ICU stay was 1–1.5 days (36.4 ± 4.4 hours); in Group II – 1.5–2 days (48.2 ± 4.5 hours); whereas in the control group it was significantly longer – 3–4 days (93.5 ± 4.3 hours, *p < 0.05).In addition to preoperative changes, the extent of surgical intervention, the duration of cardiopulmonary bypass, and the remodeling of intracardiac hemodynamics played a crucial role in determining the clinical course of the postoperative period and contributed to the development of a number of complications.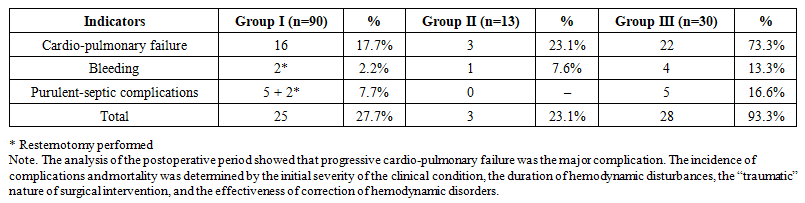 | Table 3. Number of complications and causes of death in the postoperative period by groups |
The average ICU stay among patients with complications was 91.5 ± 8.8 hours (3.5–4 days). By groups, this indicator was 72.8 ± 8.8 hours in Group I, 96.4 ± 9.2 hours in Group II, and 93.5 ± 4.3 hours in the control group. The average length of hospital stay (bed-days) was 11 ± 2 days in Group I (Kawazoe technique), 12 ± 1 days in Group II, and 18 ± 4 days in the control group. | Table 4. Postoperative parameters by groups |
Another important indicator of the effectiveness of atrioplasty is the evaluation of long-term outcomes. The follow-up results demonstrated that normalization of hemodynamics in the left heart and changes in LA size in most patients had a significant clinical impact during the postoperative period. This was reflected in the positive dynamics of many defect-related symptoms — improvement of general condition, reduction of dyspnea and palpitations, regression of signs of decompensation in systemic and pulmonary circulation, recovery of hemodynamics, and favorable cardiac chamber remodeling.For the assessment of long-term outcomes, data from repeated outpatient examinations were analyzed. Long-term results of surgery for mitral valve disease with atriomegaly and LA reduction were evaluated in 91 patients (68.4% of discharged patients). Among them, 54 patients underwent Group I Kawazoe atrioplasty, 13 patients underwent Group II “Mercedes” atrioplasty, and 24 patients were included in the control group. The average follow-up period was 13.0 ± 5.5 years (Figure 3).Analysis of outcomes related to elimination of valve-associated complications depending on the technique of LA reduction and mitral valve intervention showed the following:• Group I (Kawazoe atrioplasty): 94.7% free of valve-related complications,• Group II (Mercedes atrioplasty): 88.9%,• Control group: 74.2%.Similarly, analysis of outcomes related to elimination of cerebrovascular complications demonstrated:• Group I (Kawazoe atrioplasty): 88.2%,• Group II (Mercedes atrioplasty): 84.1%,• Control group: 76.4%.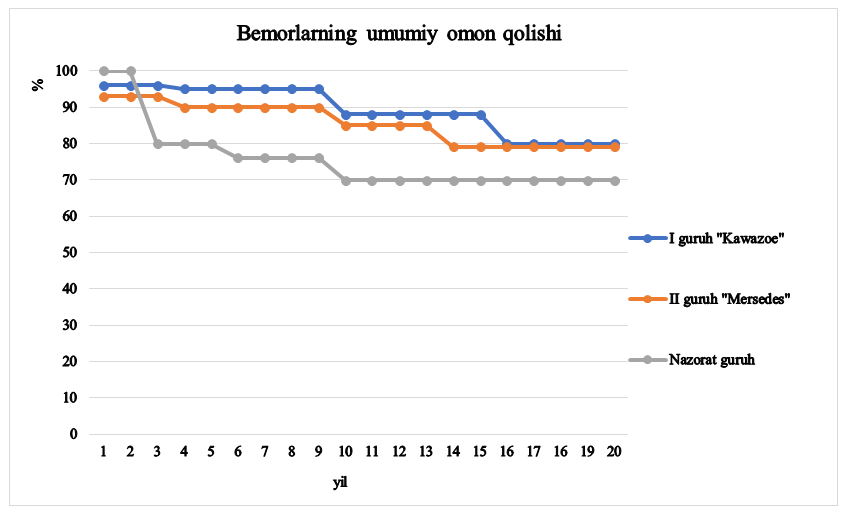 | Figure 3. Overall survival of patients |
We evaluated long-term outcomes using the three-point scale widely accepted in cardiac surgery and employed by many researchers: good, satisfactory, and unsatisfactory results (Marcinkevichus A., 1991; Tsukerman G.I., 1990; Gromova G.V., 1999).Outcomes were considered good when the patient’s condition normalized: complaints characteristic of prosthetic valve dysfunction disappeared, manifestations of heart failure significantly decreased, and tolerance to physical activity improved. Physical performance corresponded to NYHA functional class I–II. Electrocardiographic, echocardiographic, and X-ray examinations revealed positive changes, manifested in the reduction of cardiac chamber dimensions, improvement of myocardial microcirculation, and enhancement of contractile function parameters. Postoperative complications did not leave harmful consequences for the organism, and no activity of inflammatory processes was observed.Satisfactory results were defined as cases where, according to echocardiographic and radiographic findings, correction of hemodynamics led to an improvement in the patients’ clinical status and objective condition. However, disturbances of rhythm persisted on electrocardiography or enlargement of the cardiac chambers continued on echocardiography. In this group, physical activity was preserved at an acceptable level, with performance corresponding to NYHA functional class II–III.In addition to the severity of the patients’ condition, limiting factors affecting surgical efficacy included reactivation of inflammatory processes and residual effects of postoperative complications, such as rhythm disturbances, arrhythmias, and complete atrioventricular blocks.Unsatisfactory results included cases where subjective and objective indicators remained unchanged or worsened after surgery. Typically, such outcomes occurred in the presence of active endocarditis, when the body’s compensatory reserves were exhausted. Analysis of unsatisfactory results showed that all these patients exhibited high activity of endocarditis, and outcomes of repeat surgeries depended on the severity of cardiac and multi-organ failure, as well as the nature of the surgical intervention performed.An analysis of the dynamics of outcomes showed that 67 patients (73.6%) were assessed as having good results, while 24 patients (26.4%) were classified as satisfactory.Regression of radiological signs of the defect following surgical interventions was primarily associated with improvement in pulmonary condition, followed by a decrease in the size of cardiac chambers (LA, RA, RV, LV). The dynamics of pulmonary pattern changes served as an indicator of pulmonary circulation status. Preoperatively, 43.4% of patients demonstrated pulmonary vascular pattern enhancement, 12.88% showed signs of pulmonary congestion, and in long-term follow-up these indicators persisted in only 15.8% of patients. Signs of pulmonary stasis decreased in 62% of patients, indicating that these changes were not irreversible.In the dynamics of the cardiopulmonary coefficient, a significant reduction was recorded. Preoperatively, 70% of patients had a cardiopulmonary coefficient above 0.60; in the long-term period this was seen in only 24.8%. Before surgery, 30% of patients had a cardiopulmonary coefficient between 0.50 and 0.60, while in the long-term follow-up this was noted in only 14.7% of patients.In the long-term period, changes in respiratory parameters characterizing the compression of the respiratory organs were recorded in patients who underwent atrioplasty. Thus, radiological studies allow for an objective assessment of the postoperative dynamics in patients after left atrial volume-reducing interventions using different techniques. The results of the study demonstrated that after such surgery, many radiological signs of the defect regressed over time, and the duration as well as the nature of this process were primarily determined by the type of defect and the initial state of the myocardium.Comprehensive echocardiographic examination provides information on the size and volumetric parameters of the cardiac chambers, enables visualization of prosthetic valves, assessment of their function, evaluation of myocardial contractile function, detection of regurgitation on the tricuspid valve, and calculation of such important hemodynamic indicators as the transvalvular pressure gradient and the effective orifice area of the prosthetic mitral valve.Echocardiographic monitoring did not reveal any signs of prosthetic mitral valve dysfunction in any of the groups. The long-term echocardiographic data confirmed statistically significant differences in parameters related to changes in cardiac chamber volumes and left ventricular ejection fraction (LVEF) recorded in the early postoperative period. Thus, in Groups I and II, in addition to the significant reduction in LA and RA volumes documented during the hospital stage (P < 0.05) in patients with primary atriomegaly and mitral valve disease, a decrease in pulmonary artery pressure, as well as an increase in LV ejection fraction and contractility index, were observed when compared to preoperative values (Table 5).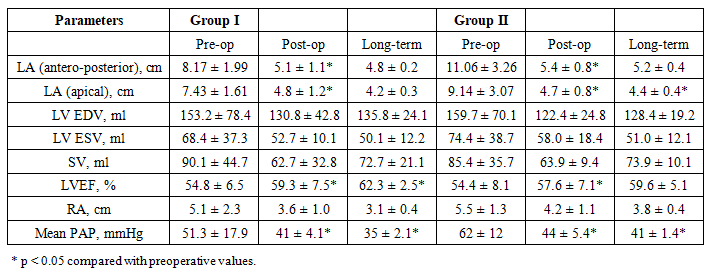 | Table 5. Long-term echocardiographic parameters in patients of Groups I and II |
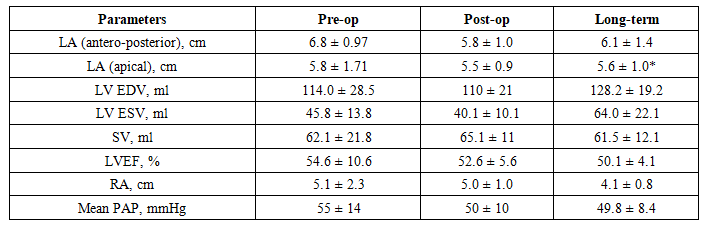 | Table 6. Long-term echocardiographic parameters in patients of the control group (Group III) |
Findings:• In Groups I and II (Kawazoe and Mercedes atrioplasty), long-term follow-up confirmed a sustained reduction in LA and RA size, decreased pulmonary artery pressure, and improved LV systolic function (EF ↑).• In contrast, in the control group, there was a slight increase in LA dimensions, an increase in LV volume, and a decline in contractility (EF ↓). Additionally, among 91 patients examined in long-term follow-up:• 62.6% (57 patients) maintained sinus rhythm,• 37.4% (34 patients) had atrial fibrillation.Sinus rhythm was preserved in 64% of Group I (Kawazoe), 48.8% of Group II (Mercedes), and only 28.1% of the control group.One Group I patient required reoperation after 14 years due to bioprosthetic dysfunction.Among patients in the control group, one patient required reoperation 4 months after the initial surgery. Control echocardiography revealed isolated left atrial (LA) thrombosis without mitral prosthesis dysfunction. At the time of the initial operation, the LA measured 6.5 cm and atrioplasty had not been performed. It was determined that the patient had violated anticoagulant therapy compliance, with untimely monitoring of PTI.In the late postoperative period, no clinically significant bleeding events associated with anticoagulant therapy were observed. Following surgery, all patients demonstrated improvement in their functional class, with the majority reaching NYHA class II. Reduction of the enlarged LA, combined with simultaneous correction of mitral valve pathology, resulted in normalization of intracardiac hemodynamics and a decrease in heart failure manifestations.By the end of the first postoperative year, in most patients, systemic and pulmonary circulatory abnormalities associated with giant LA enlargement and mitral valve defects had been successfully reversed. The subsequent course and occurrence of complications depended on myocardial functional reserves, adequacy of concomitant valve correction, occurrence of prosthetic endocarditis, adequacy of drug therapy, and adherence to comprehensive rehabilitation measures.Timely monitoring and systematic prevention of complications, as well as adequate pharmacological therapy during the late postoperative period, are essential for maintaining favorable functional outcomes. At discharge, all patients were advised to continue medical therapy. During the first year, patients underwent a rehabilitation period, and if the defect was adequately corrected, assignment of disability groups II or III was recommended depending on professional background. Considering work profile, activity of inflammatory processes, stage of circulatory failure, rhythm disturbances, and residual postoperative complications, a certain proportion of patients could even be permitted to return to work.
Additionally, among 91 patients examined in long-term follow-up:• 62.6% (57 patients) maintained sinus rhythm,• 37.4% (34 patients) had atrial fibrillation.Sinus rhythm was preserved in 64% of Group I (Kawazoe), 48.8% of Group II (Mercedes), and only 28.1% of the control group.One Group I patient required reoperation after 14 years due to bioprosthetic dysfunction.Among patients in the control group, one patient required reoperation 4 months after the initial surgery. Control echocardiography revealed isolated left atrial (LA) thrombosis without mitral prosthesis dysfunction. At the time of the initial operation, the LA measured 6.5 cm and atrioplasty had not been performed. It was determined that the patient had violated anticoagulant therapy compliance, with untimely monitoring of PTI.In the late postoperative period, no clinically significant bleeding events associated with anticoagulant therapy were observed. Following surgery, all patients demonstrated improvement in their functional class, with the majority reaching NYHA class II. Reduction of the enlarged LA, combined with simultaneous correction of mitral valve pathology, resulted in normalization of intracardiac hemodynamics and a decrease in heart failure manifestations.By the end of the first postoperative year, in most patients, systemic and pulmonary circulatory abnormalities associated with giant LA enlargement and mitral valve defects had been successfully reversed. The subsequent course and occurrence of complications depended on myocardial functional reserves, adequacy of concomitant valve correction, occurrence of prosthetic endocarditis, adequacy of drug therapy, and adherence to comprehensive rehabilitation measures.Timely monitoring and systematic prevention of complications, as well as adequate pharmacological therapy during the late postoperative period, are essential for maintaining favorable functional outcomes. At discharge, all patients were advised to continue medical therapy. During the first year, patients underwent a rehabilitation period, and if the defect was adequately corrected, assignment of disability groups II or III was recommended depending on professional background. Considering work profile, activity of inflammatory processes, stage of circulatory failure, rhythm disturbances, and residual postoperative complications, a certain proportion of patients could even be permitted to return to work.
3. Conclusions
Left atrial enlargement in mitral valve disease, due to compression of the posterobasal segments of the left ventricle and the development of heart failure, is an indication for atrioplastic surgical procedures (left atrial volume reduction). When the left atrium exceeds 5.5–6.0 cm, suture techniques such as “Kawazoe” and “Mercedes” atrioplasty are recommended.• For Kawazoe atrioplasty, the main indication is enlargement of the para-annular segment beyond 5–6 cm.• For Mercedes atrioplasty, the indication is enlargement of the left atrial dimension involving both the para-annular segment (>5–6 cm) and the segment between the right and left pulmonary veins (>5 cm).• Kawazoe atrioplasty is particularly indicated when the enlarged left atrium compresses the posterobasal segments of the left ventricle, the main bronchi, and pulmonary parenchyma.The Kawazoe technique reduced left atrial size from 8.2 ± 1.9 cm to 5.1 ± 1.1 cm (p < 0.05), while the Mercedes technique reduced size from 11.1 ± 3.3 cm to 5.4 ± 0.8 cm (p < 0.05). These procedures did not significantly prolong cardiopulmonary bypass time (139.1 ± 60 min) or aortic cross-clamp time (99.3 ± 32 min) (p > 0.05).Among patients, the suture atrioplasty technique demonstrated more favorable postoperative effects, including an increase in left ventricular ejection fraction (from 54.8 ± 6.5% to 59.3 ± 7.5%), regression of pulmonary hypertension, and a decrease in pulmonary artery pressure (from 62 ± 12 mmHg to 41 ± 5.4 mmHg) (p < 0.05).Application of atrioplasty restored sinus rhythm in 88 patients (63.7%) in the early postoperative period and preserved sinus rhythm in 57 patients (62.6%) in long-term follow-up, thereby preventing thromboembolic complications.The overall survival rate at 10 years was 85–88%.
References
| [1] | Kawazoe K., Verri S., Takahara Y. Left atrial reduction for mitral valve disease with giant left atrium. J Thorac Cardiovasc Surg. 1983. |
| [2] | Dzemeshkevich S.L. Surgical treatment of patients with mitral valve defects and giant left atrium. Klinicheskaya Meditsina, 2000. |
| [3] | Sinatra R., Pulitani I., Antonazzo A. Surgery for giant left atrium: atrial reduction and mitral valve surgery. Ann Thorac Surg. 2001; 72(3): 911–917. |
| [4] | Armstrong R. Surgical reduction of the left atrium: indications, methods and results. Heart Lung Circ. 2007. |
| [5] | Apostolakis E., et al. Left atrial reduction techniques for giant left atrium: current evidence and outcomes. Eur J Cardiothorac Surg. 2008; 33(3): 391–402. |
| [6] | Braunwald E., Zipes D.P., Libby P. Heart Disease: A Textbook of Cardiovascular Medicine. 7th ed. Philadelphia: WB Saunders; 2005. |
| [7] | Camm A.J., Kirchhof P., Lip G.Y.H., et al. Guidelines for the management of atrial fibrillation. Eur Heart J. 2010; 31: 2369–2429. |
| [8] | Bonow R.O., Mann D.L., Zipes D.P., Libby P. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 9th ed. Philadelphia: Saunders Elsevier; 2011. |
| [9] | Creswell L.L., Schuessler R.B., Rosenbloom M., Cox J.L. Hazards of postoperative atrial arrhythmias. Ann Thorac Surg. 1993; 56: 539–549. |
| [10] | Fuster V., Rydén L.E., Cannom D.S., et al. ACC/AHA/ESC 2006 guidelines for the management of atrial fibrillation. J Am Coll Cardiol. 2006; 48: e149–246. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML