-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3242-3244
doi:10.5923/j.ajmms.20251509.88
Received: Sep. 2, 2025; Accepted: Sep. 21, 2025; Published: Sep. 29, 2025

Features of Thyroid Ultrasonal Examination in Patients with Hypothyroidism
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLD. N. Kambarova
Andijan State Medical Institute, Uzbekistan
Correspondence to: D. N. Kambarova, Andijan State Medical Institute, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Ultrasonography is an indispensable additional tool in hypothyroidism, which can be observed at almost all ages, from the prenatal period to geriatric age groups. It should be remembered that hypoechogenicity is a key sign of hypothyroidism.
Keywords: Hypothyroidism, Ultrasonography, Thyroid gland
Cite this paper: D. N. Kambarova, Features of Thyroid Ultrasonal Examination in Patients with Hypothyroidism, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3242-3244. doi: 10.5923/j.ajmms.20251509.88.
Article Outline
1. Introduction
- Hypothyroidism, caused by a low level of thyroid hormones, is one of the most common endocrine diseases. It has various etiologies and manifestations; when left untreated, it increases morbidity and mortality. Although the main cause of hypothyroidism worldwide is still a iodine-deficient diet, in regions where food intake of iodine is sufficient, it is an autoimmune thyroid disease. Today, it is successfully treated with exogenous thyroid hormone [3].Hypothyroidism often constitutes a significant part of the daily workload of endocrinology and radiology. Interdisciplinary communication is very important in approaching and treating this endocrine disorder. In the last 30-40 years, the most specific visualization method in routine thyroid disease examination is ultrasound examination (USI) [1]. Ultrasonography has significantly changed medical practice. Relative ease of use, absence of ionizing radiation, low cost, and accessibility of the patient's bed made it invaluable in many clinical settings where patients with thyroid diseases are examined. The superficial location of the thyroid gland during ultrasound provides the advantage of high resolution for assessing thyroid parenchyma and its lesions. Ultrasound is an indispensable examination for almost all thyroid diseases.On the other hand, thyroid ultrasound absolutely requires specific recognition of various sonographic manifestations of autoimmune diffuse thyroid disease, especially in the clinical picture of antibody-free hypothyroidism. This is also important for determining whether the focal anomaly represents a true node that may require fine-needle aspiration biopsy or is a part of an inflammatory process often called a pseudo-node [3,4]. Ultrasound examination, like other tests, should be used to confirm a differential diagnosis when it is necessary to answer a specific diagnostic question based on the patient's medical history and physical examination [5].It must be precisely correlated with other data. The justification for thyroid ultrasound should be made taking into account the patient's medical history and the results of laboratory tests.Purpose of the research. Prove the advantage of using ultrasound in the diagnosis of thyroid hypothyroidism.
2. Materials and Methods of Research
- The study included 118 patients with chronic migraine (CM). The diagnosis of migraine was made according to the International Classification of Headaches (ICHD-III).The patients were divided into 3 groups. The 1st group consisted of 38 patients with chronic headache lasting up to 5 years and hypothyroidism. The 2nd group included 41 patients with CM with a headache duration of more than 5 years and hypothyroidism. The 3rd group consisted of 39 patients with CM without hypothyroidism. A control group was also created, which included 20 practically healthy individuals.The age range of patients in the three groups, as well as in the control group, was >20 years, but <50 years. Thus, the average age of the 1st group was 28.7±4.6 years; 2nd group - 36.3±5.2 years; 3rd group - 31.9±3.8 years; control group - 33.5±5.4 years.
3. Results and Their Discussion
- All patients underwent ultrasound of the neck organs before admission to the hospital and outpatient clinic. It was conducted in standard modes (gray scale mode), ED, and SDK. When performing ultrasound in polyclinics, several tasks were solved. Firstly, documentary confirmation of thyroid enlargement was required, determining the structure, if possible, thyroid size and volume, location, size, and volume of thyroid nodes. Secondly, the task of ultrasound at this stage was to assess thyroid nodal formations using the TIRADS system.Outpatient examinations were performed in various medical institutions on ultrasound machines of different classes (mainly linear (7-14 MHz) and convex sensors) by ultrasound doctors of different levels of training.When analyzing the protocols of outpatient ultrasound in patients of the 1st group, it was established that in all cases, the size, location of the thyroid gland, and its relationship with surrounding organs and vessels corresponded to the true size of the thyroid gland (Table 1).
|
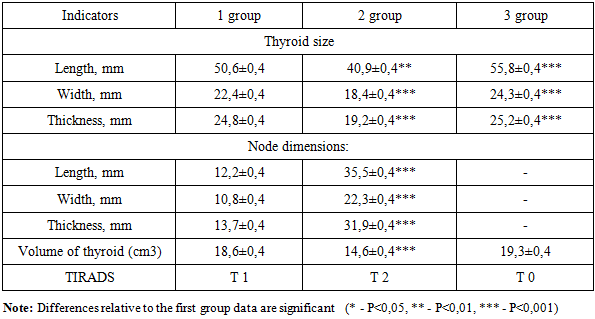
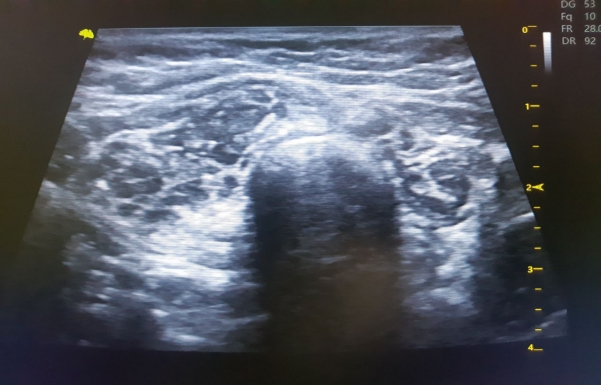 | Figure 1. Patient Z.N., 1990. DS: Hypoplasia of the thyroid gland 1st degree |
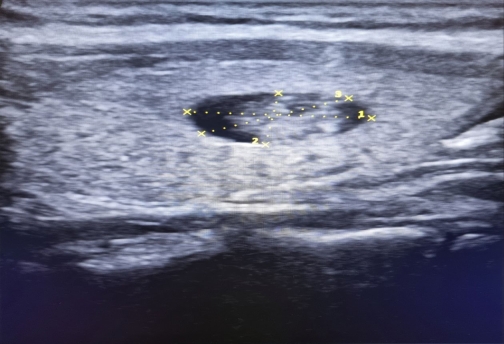 | Figure 2. Patient A.M., 1980 DS: Right thyroid gland cyst |
 | Figure 3. Patient M.B., 1996 DS: 2-3-degree thyroid hypoplasia |
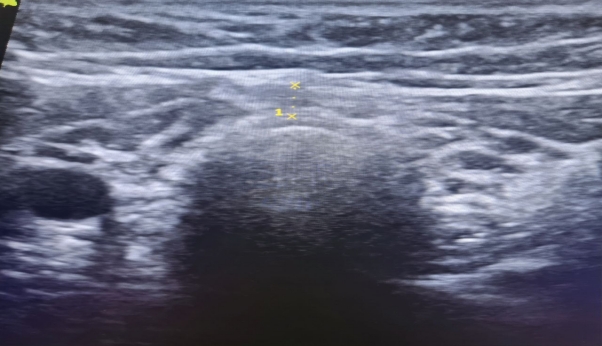
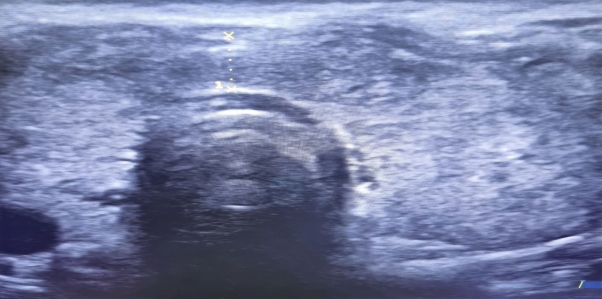 | Figure 4. Patient F.D., 1992. D-d: Diffuse thyroid gland 2st degree. The image shows the measurement of the neck thickness |
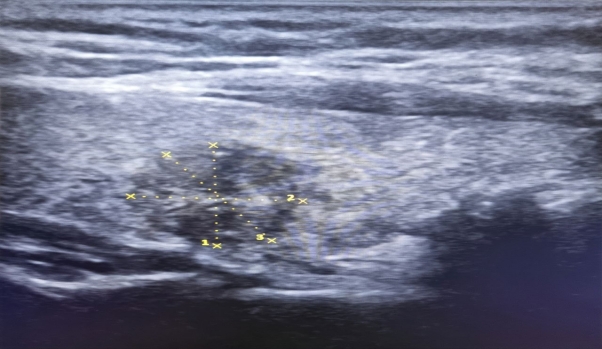 | Figure 5. Patient L.R., 1985 y. D-d: right lobe node of the thyroid gland |
4. Conclusions
- Ultrasonography is an irreplaceable additional tool for hypothyroidism, which can be observed in almost all age groups, from the intrauterine period to geriatric age groups.