-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3225-3229
doi:10.5923/j.ajmms.20251509.84
Received: Sep. 5, 2025; Accepted: Sep. 24, 2025; Published: Sep. 29, 2025

Morphological Structure of the Levator Muscles in Congenital and Acquired Ptosis of the Upper Eyelid
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKurbanova Nilufar Pulatovna
Assistant, Department of Anatomy, Urgench Branch of the Tashkent Medical Academy, Uzbekistan
Correspondence to: Kurbanova Nilufar Pulatovna, Assistant, Department of Anatomy, Urgench Branch of the Tashkent Medical Academy, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article considers the morphological features of various forms of ptosis of the levator muscle of the upper eyelid – congenital and acquired. It pays special attention to the comparative study of the structural organization of muscle fibers, the severity of connective tissue components, as well as the vascular and nervous supply of the muscle. The data obtained show significant differences in the architectonics of the levator muscle depending on the genesis of ptosis, which indicates the inequality of the pathogenetic mechanisms underlying these conditions. The revealed morphological features allow us to take a fresh look at the principles of surgical correction of ptosis and emphasize the need for an individual approach to choosing surgical tactics. The results of the work can serve as a morphological basis for further improvement of methods of plastic ophthalmic surgery.
Keywords: Upper eyelid ptosis, Levator muscle, Morphology, Congenital ptosis, Priobretyonny ptosis, Histology, Ophthalmosurgery, Morphometry, Eyelid anatomy, Surgical correction
Cite this paper: Kurbanova Nilufar Pulatovna, Morphological Structure of the Levator Muscles in Congenital and Acquired Ptosis of the Upper Eyelid, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3225-3229. doi: 10.5923/j.ajmms.20251509.84.
Article Outline
1. Introduction
- In recent years, the problem of individualization of ptosis treatment has been actively discussed in the literature, which is impossible without a clear understanding of the levator muscle architectonics. Domestic and foreign studies have established that the muscle structure in the congenital form of the disease is characterized by pronounced hypoplasia of fibers and their partial replacement with connective tissue, while acquired ptosis is characterized by atrophy, dystrophy and sclerotic changes [1, p. 112].The study of the morphology of the levator muscle is of particular importance in childhood, when congenital ptosis can cause amblyopia due to constant overlap of the pupil. In such cases, surgery becomes not only a cosmetic procedure, but also the prevention of irreversible visual impairment.A comprehensive study of the morphological structure of the levator muscle allows us to clarify the pathogenesis of ptosis, deepen our understanding of the causes of its insufficiency and determine areas for improving surgical techniques.Blepharoptosis is one of the common pathologies of the accessory apparatus of the eye, occupying a leading place in the structure of eyelid diseases. Currently known etiological factors of upper eyelid ptosis may be muscle changes of various genesis, disorders of neuromuscular transmission, damage to the oculomotor nerve and its nucleus, disruption of sympathetic innervation, trauma and inflammation of the eyeball [1]. Statistical data on the incidence of upper eyelid ptosis are few and contradictory. It has been shown that blepharoptosis accounts for 9% of all eye pathologies [2]. It is noted that in 40% of cases, simple unilateral ptosis is detected, in 7% of cases – bilateral, in 21% of cases – unilateral ptosis with damage to the superior rectus muscle [3]. According to other data, the simple form of ptosis occurs in 75% of patients, and the complicated form is recorded in 25% of cases [4]. Congenital ptosis is often primarily perceived as a cosmetic defect. However, this pathology also has a negative impact on the functional development of the eye, leading to obscuration amblyopia, strabismus, corneal refractive errors, and visual field limitation. It is also possible to develop contractures of the neck muscles and impaired posture, which is due to the forced position of the head. The clinical features of acquired ptosis of the upper eyelid are varied and are determined by the type and causes of occurrence. This pathology causes complications such as chronic headaches due to forced tension of the frontal muscle, psychosomatic disorders that affect the social activity of patients. With successful correction of blepharoptosis, mental discomfort is reduced, helping in social adaptation [5]. In addition to a cosmetic defect and psychological disorders, blepharoptosis leads to the development of such a serious pathology as uncorrectable astigmatism [6]. With partially or completely limited active excursion of the upper eyelid, functional disorders occur that limit the field of vision from above, accompanied by constant fatigue, the development of amblyopia and binocular vision disorder, forced head position and cervical osteochondrosis [7]. With pronounced ptosis of the upper eyelid, changes in the curvature of the cornea are likely to occur. Keratometric and video cartographic studies have shown that with successful surgical correction of blepharoptosis, refraction also changes due to changes in the curvature of the cornea. A third of patients with blepharoptosis showed signs of transient astigmatism greater than 1 diopter [8].There is no proven significant effectiveness of conservative methods (UHF therapy, electrophoresis, myostimulation) in the treatment of blepharoptosis, therefore surgical intervention is necessary, which is one of the most difficult problems faced by ophthalmologists. The frequency of repeated operations to eliminate ptosis of the upper eyelid, according to different authors, ranges from 5 to 35% of cases [3,9]. Today, there are a large number of methods of surgical treatment of blepharoptosis, the main ones of which are operations on the levator of the upper eyelid itself and its aponeurosis, suspensory operations and operations on the superior tarsal muscle [5–7]. To achieve a positive treatment result, it is necessary to accurately determine the etiological factor, perform thorough preoperative diagnostics and select a pathogenetically oriented surgical method. The effectiveness of surgical intervention largely depends on the presence of dystrophic changes in the muscle, which can be detected by histological analysis after the resection of the levator of the upper eyelid. Pathological processes occurring in the levator of the upper eyelid require deep analysis for the correct determination of further pathogenetically substantiated tactics of surgical treatment. Thus, the initial morphological state of the levator complex of the upper eyelid is the most important factor that determines positive treatment results, which determined the purpose of this study.Purpose of the Scientific Work. Based on dynamometric data and the results of histological examination, to study the features of the morphological structure of the levator in congenital and acquired ptosis.
2. Materials and Testing Methods
- In 2024–2025, on the dynamometric indicators such as the strength and fatigue of the upper eyelid levator prepared in the Khorezm branch of the Republican Scientific and Practical Center of Oncology.The study of the morphological structure of the upper eyelid levator muscle was conducted on clinical material obtained from patients with various forms of ptosis who underwent surgical treatment in an ophthalmosurgical hospital. The sample included 42 patients aged 5 to 65 years. Of these, 21 cases were congenital forms of ptosis, 18 were acquired, and 3 more samples made up a conditional control group represented by tissues obtained during reconstructive surgeries without signs of ptosis. The biological material was fixed in 10% neutral formalin, subjected to standard wiring and embedded in paraffin blocks. Sections 5–6 μm thick were stained with hematoxylin and eosin for a general assessment of the structure, picrofuchsin according to Van Gieson to identify connective tissue, and an immunohistochemical study was also carried out using antibodies to desmin and type I collagen. For quantitative assessment, computer morphometry methods were used using the Leica digital microscopy system.
3. The Obtained Results and Their Discussion
- Histological examination of specimens obtained from patients with congenital ptosis revealed marked hypoplasia of muscle fibers. They were noticeably thinned, had abnormal orientation, and in some cases demonstrated fragmentation. In most preparations, uneven fiber diameter was observed, indicating a disruption of normal myogenesis.The study of the macroscopic characteristics of the removed fragments showed that in the congenital upper eyelid ptosis group, the average length of the resected fragment was 1.22±0.34 mm, while in the acquired upper eyelid ptosis group this value was significantly greater and was 2.33±1.32 mm (p ≤0.05). No statistically significant differences were found in the height and width of the removed fragments, which were 0.59±0.33 mm and 0.52±0.38 mm in the congenital ptosis group, respectively. The height of the removed fragments in the acquired ptosis group was 0.61±0.57 mm, and the width was 0.45±0.23 mm (Fig. 1). Most of the levator fragments in the congenital upper eyelid ptosis group were pale pink, had an irregular shape, and a soft elastic consistency (Fig. 2).
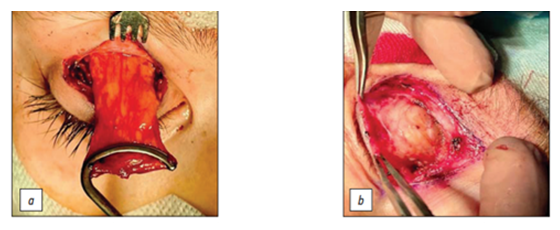 | Figure 1. Macroscopic picture of the removed levator fragment: a — congenital ptosis; b — acquired ptosis of the upper eyelid |
 | Figure 2. Levator fragment removed from patients with congenital ptosis of the upper eyelid |
 | Figure 3. Levator fragment removed from patients with acquired ptosis of the upper eyelid |
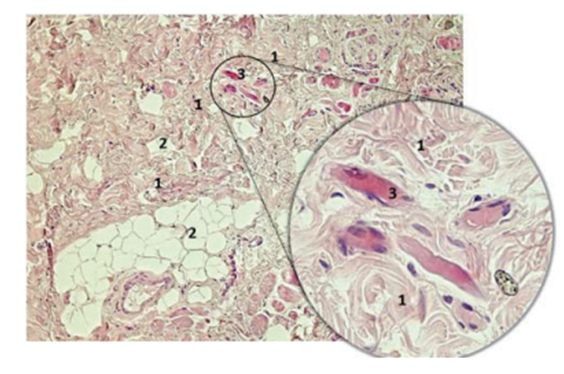 | Figure 4. Histological preparation of levator in congenital ptosis with proliferation of fibrous-adipose tissue. Color — hematoxylin/eosin, magnification 100x, inset — 400x. 1 — fibrous tissue, 2 — adipose tissue, 3 — skeletal muscle fibers |
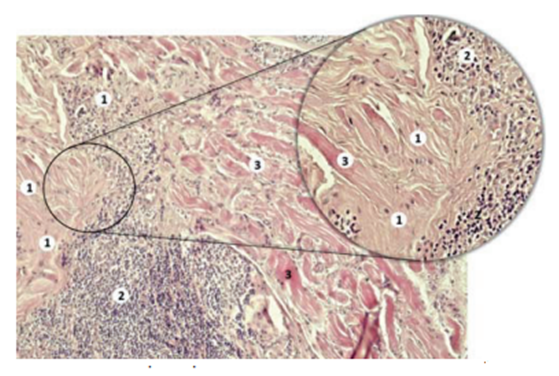 | Figure 5. Histological preparation of levator in congenital ptosis with the proliferation of fibrous tissue. Color — hematoxylin/eosin, magnification 100x, inset — 400x. 1 — fibrous tissue with hyalinosis, 2 — mononuclear inflammatory infiltration of a focal nature, 3 — skeletal muscle fibers |
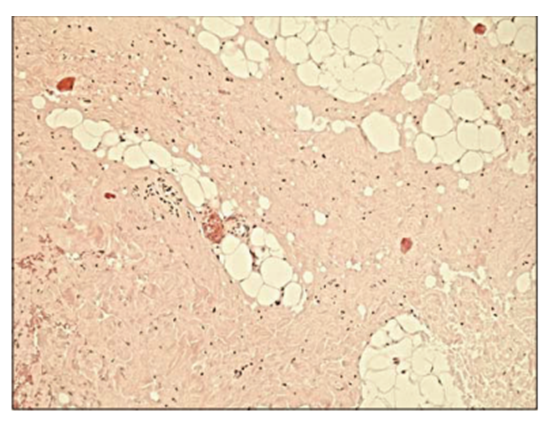 | Figure 6. Histological preparation of levator with acquired ptosis of the upper eyelid with the proliferation of fibrous-adipose tissue. Color — hematoxylin/eosin, magnification 100x |
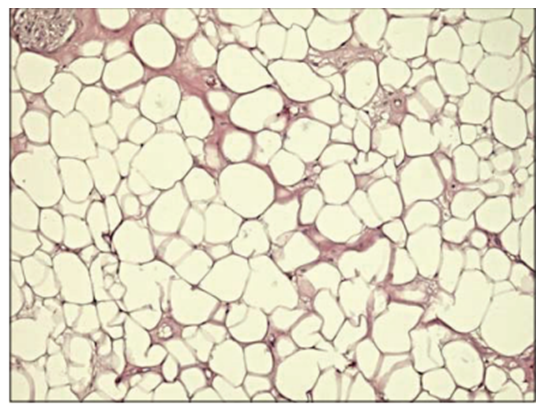 | Figure 7. Histological preparation of levator with adipose tissue overgrowth with acquired ptosis of the upper eyelid. Color — hematoxylin/eosin, magnification 100x |
4. In Conclusions
- Dynamometric and histological analysis of the morphological structure of the levator in congenital and acquired ptosis of the upper eyelid revealed a number of features. Congenital ptosis is generally characterized by relatively low strength and rapid fatigue of the levator of the upper eyelid, a higher frequency of occurrence of proliferation of fibro–fatty and fibrous tissue. In the group of acquired ptosis, proliferation of fibro–fatty and fatty tissue is determined in equal proportions, and according to dynamometric data, they are distinguished by average strength and fatigue. The results obtained can be used to diagnose various forms of ptosis and select an effective method for surgical correction of this pathology.The conducted study allowed us to identify the morphological features of the levator muscle of the upper eyelid in congenital and acquired ptosis.1. In congenital ptosis, the muscle is characterized by hypoplasia of fibers, their pronounced replacement with connective tissue, a decrease in the density of capillaries and nerve endings. These changes confirm the congenital nature of the pathology and explain the limited compensatory capabilities.2. In acquired ptosis, the morphological picture is represented by dystrophic changes in muscle fibers, moderate sclerosis, microcirculation disorders and changes in the aponeurosis. The pathology is secondary and develops gradually.3. Quantitative differences in the thickness of muscle fibers, the percentage of connective tissue, the density of blood vessels and the number of nerve endings indicate the different nature of congenital and acquired ptosis. 4. Clinical manifestations of the disease directly correlate with morphological changes: congenital ptosis is accompanied by minimal eyelid mobility and low efficiency of standard surgical techniques, while acquired ptosis is more amenable to reconstructive treatment. 5. The data obtained confirm the need for a differentiated approach to the choice of surgical tactics and can serve as a morphological justification for improving the methods of plastic ophthalmic surgery.