Zakirov Muzaffar Rakhimdzhanovich
Researcher at the Urgench Branch of the Tashkent Medical Academy, Uzbekistan
Correspondence to: Zakirov Muzaffar Rakhimdzhanovich, Researcher at the Urgench Branch of the Tashkent Medical Academy, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
Polychemotherapy, being one of the key methods of treating malignant neoplasms, is accompanied by a high risk of developing nephrotoxic complications. Antitumor drugs can cause a wide range of kidney damage, including glomerular and tubulointerstitial changes, electrolyte disturbances, clinically manifested by acute kidney injury with subsequent transformation into chronic kidney disease. The article discusses the pathomorphological features of these injuries, their clinical and morphological relationship and risk factors due to both the patient's characteristics and the specificity of the cytostatic agents used. The need for early diagnosis of nephrotoxicity, comprehensive assessment of the excretory function of the kidneys and timely implementation of preventive and therapeutic measures is emphasized. Particular attention is paid to the role of a multidisciplinary approach in the management of cancer patients, which can increase the effectiveness of antitumor treatment and reduce the incidence of severe complications.
Keywords:
Polychemotherapy, Antitumor drugs, Nephrotoxicity, Acute kidney injury, Chronic kidney disease, Glomerular lesions, Tubulointerstitial changes, Electrolyte disturbances, Pathomorphology, Cancer patients
Cite this paper: Zakirov Muzaffar Rakhimdzhanovich, Pathomorphological Aspects of Kidney Damage Caused by Polychemotherapy, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3219-3224. doi: 10.5923/j.ajmms.20251509.83.
1. Introduction
The increase in the incidence of cancer in recent decades requires the development of new drugs and methods of influencing tumor cells, and in some cases, the intensification of chemotherapy regimens. Along with the successes achieved in the treatment of tumor diseases, the toxicity of the treatment is a fairly big problem. Kidney damage developing in cancer patients can lead to a change or increase in the concentration of drugs, thereby increasing their toxicity, prolonging the duration of hospitalization and increasing mortality. The spectrum of kidney damage in tumor diseases is quite wide and can be caused both by direct tumor infiltration and damage to renal tissue by tumor cell metabolites, glomerular damage, and by the nephrotoxic effect of drugs and radiation therapy. In addition, one should take into account the risks associated with complications after bone marrow transplantation (BMT), infections against the background of immunosuppression (including sepsis), and tumor lysis syndrome [1-3]. Chemotherapeutic drugs are a common cause of acute and chronic kidney damage in cancer patients. Nephrotoxicity is predominantly associated with damage to the proximal, less commonly distal tubules and glomeruli [4,5].Purpose of the Scientific Work is a comprehensive study of structural and functional changes in renal tissue under the influence of antitumor drugs, identification of characteristic morphological markers of nephrotoxicity, as well as clarification of the pathogenetic mechanisms of damage for the subsequent development of diagnostic criteria, prognostic indicators and preventive approaches to reducing the risk of renal dysfunction in cancer patients undergoing polychemotherapy.
2. Materials and Testing Methods
The material obtained included outpatient cards, medical histories, results of clinical examinations of patients, as well as the results of studies of macropreparations taken during operations and micropreparations prepared from them at the Khorezm branch of the Republican Scientific and Practical Center of Oncology in 2024–2025.
3. The Obtained Results and Their Discussion
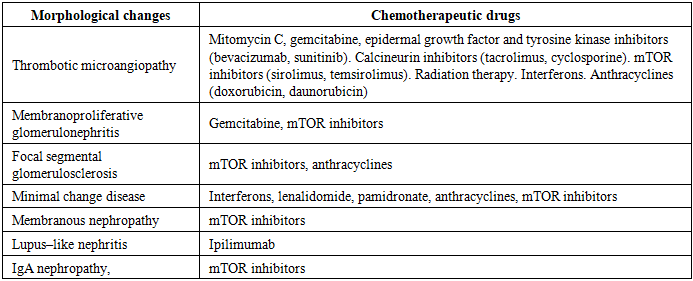
Acute tubular damage is most often represented by acute tubular necrosis, isolated tubulopathy, and crystalline nephropathy. Interstitial tissue lesions develop as acute and/or chronic interstitial nephritis. Glomerular lesions are more often associated with paraneoplastic syndrome or direct tumor damage, but can occur after stem cell transplantation, less often – after the use of certain chemotherapeutic drugs [4,5].The main groups of antitumor drugs include the following [6]:alkylating agents (ifosfamide, platinum drugs);antimetabolites (methotrexate);antitumor antibiotics;substances of natural (mainly plant) origin;hormones, agonists and antagonists of hormones; – targeted drugs (angiogenesis inhibitors, tyrosine kinases) and other drugs.Among the above, alkylating agents and antimetabolites have the greatest nephrotoxicity. In addition to cytostatic agents, various types of concomitant therapy in cancer patients (antibacterial, antifungal, antiviral drugs, immunoglobulins, contrast agents, bisphosphonates, analgesics, anticoagulants) can also lead to kidney damage. It is necessary to assess the risk factors for nephrotoxicity of polychemotherapy before starting treatment, which are divided into patient–related, renal and drug–related. Patient–related factors primarily include female gender and age over 65 years. Elderly people are characterized by a reduction in muscle mass, which leads to a decrease in the level of creatinine in the blood serum. This masks changes in the estimated glomerular filtration rate; a decrease in the intravascular fluid volume, which contributes to an increase in the concentration of drugs. Hypoalbuminemia is often observed in this cohort of patients, which, regardless of its origin (renal, extrarenal), is accompanied by a decrease in drug binding to proteins. Women are characterized by lower values of muscle mass and volemic characteristics of different body compartments, which can lead to the prescription of unjustifiably high doses of drugs. The presence of previous acute or chronic kidney disease is also unfavorable. Patients with existing chronic kidney disease have a higher risk of developing acute kidney injury.Dehydration, metabolic disorders leading to changes in urine pH, polymorphism of the CYP45 genes responsible for drug metabolism can increase the side effects of cytostatics. Symptoms of the tumor itself and the side effects of chemotherapy are important risk factors for nephrotoxicity. These include:a decrease in circulating blood volume with nausea, vomiting, heart failure, ascites, sepsis;infiltration of renal tissue by tumor cells in lymphomas and leukemias;dysproteinemia associated with various types of renal damage, including myeloma nephropathy, lung and heavy chain diseases, amyloidosis;electrolyte disturbances, which, alone or as part of tumor lysis syndrome, are accompanied by vasoconstriction of afferent arterioles and prerenal azotemia [5,7]. Local (renal) risk factors include microcirculation disorders, drug biotransformation with formation of active oxygen species, high concentration of nephrotoxic substances in the proximal tubules and sensitivity of the latter to ischemia. Drug–induced risk factors include: the need for long–term use of high doses of a combination of cytotoxic drugs, direct cytotoxic effect of not only the chemotherapeutic agents themselves but also their metabolites, poor solubility with formation of intratubular precipitates (characteristic, in particular, of methotrexate) [7,8]. The route of drug entry into the cell also plays an important role in the development of toxicity. For some drugs, there are special organic anion or organic cation transporters. Other drugs enter from the intraluminal space by endocytosis or pinocytosis. Genetic polymorphisms responsible for OCT activity can cause changes in drug concentration and lead to increased toxicity. Another mechanism of renal tubular injury is due to the reabsorption of high concentrations of cytostatics and their metabolites from the glomerular filtrate, which leads to damage to tubular cells [7]. Acute kidney injury due to chemotherapy can be represented by prerenal, renal, and postrenal azotemia. While some drugs have a single mechanism leading to renal injury, others can cause it in several ways. A specific prerenal injury can be the syndrome of increased capillary permeability when administering interleukin–2 or interferons. Postrenal causes are quite rare, but hemorrhagic cystitis caused by cyclophosphamide has been described, leading to the development of an intravesical thrombus and obstruction of the bladder outlet [1,9].Intrinsic renal lesions are the most common and can be divided into glomerular, tubular, and interstitial. Glomerular variants are less common and are mainly represented by thrombotic microangiopathy caused by antiangiogenic drugs and gemcitabine [7,9,10]. Other manifestations include focal segmental glomerulosclerosis against the background of all classes of interferon and pamidronate. Glomerular lesions during chemotherapy are presented in Table 1 [4].Table 1. Glomerular lesions in chemotherapy
 |
| |
|
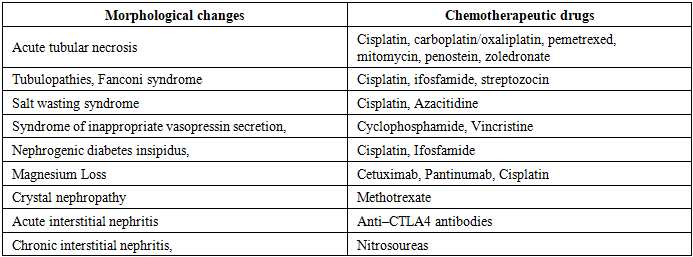
Thrombotic microangiopathy is accompanied by changes in arterioles and capillaries in the form of thickening and inflammation of their walls, separation of endothelial cells from the basement membrane, expansion of the subendothelial space due to the accumulation of proteins and cell decay products, as well as the formation of platelet thrombi with occlusion of the lumen. The most common causes of this glomerular lesion are mucin–producing tumors (stomach, mammary gland and lungs), lymphomas, radiation therapy, chemotherapy (angiogenesis inhibitors, mitomycin C, gemcitabine, bleomycin, alpha interferon). The time of thrombotic microangiopathy onset is from 1 day to several months after the administration of cytostatics. The pathogenesis of this complication is not fully understood. Increased angiogenesis, damage to endothelial cells, and tumor embolism may be important. Normal ADAMTS–13 activity is characteristic.There is no specific treatment, plasmapheresis is ineffective [7,10]. Thrombotic microangiopathy against the background of gemcitabine is characterized by proteinuria, arterial hypertension. The risk of thrombotic microangiopathy increases with long–term (more than 4 months) therapy with gemcitabine, with previous use of mitomycin. Treatment consists of discontinuing the drug, conducting plasma exchange. The question of using rituximab or eculizumab in this situation remains controversial [7,9,11]. Bevacizumab is a recombinant humanized monoclonal antibody against vascular endothelial growth factor. The administration of the drug is accompanied by the development of thrombotic microangiopathy with proteinuria in 21–63%, nephrotic syndrome – in 1.8%, arterial hypertension – in 3–36% of cases. Cetuximab is another monoclonal antibody to epidermal growth factor receptors, characterized by the development of severe hypomagnesemia [10].Tubulointerstitial lesions against the background of chemotherapy are most common, represented by the following types: acute tubular necrosis, tubulopathy, crystalline nephropathy, acute interstitial nephritis, chronic interstitial nephritis (Table 2). Acute tubular necrosis is clinically manifested by renal acute kidney injury. However, in some patients, the duration of its exposure and delayed recovery can lead to the development of chronic kidney disease.Table 2. Tubulointerstitial lesions in chemotherapy [7]
 |
| |
|
One of the characteristic laboratory signs is an increase in sodium excretion in the urine due to impaired reabsorption in the proximal tubules. Urinary sediment contains epithelial cells of the renal tubules and epithelial and granular casts. In some cases, there is a need for renal replacement therapy [6,7,11]. The use of some cytostatic drugs may also be accompanied by the development of tubulopathy. Damage to individual tubular segments may occur both with a decrease in the glomerular filtration rate and with preservation of the excretory function of the kidneys. Clinically, Fanconi syndrome (FS) is most often observed – dysfunction of the proximal tubules with impaired reabsorption of bicarbonates, amino acids, glucose and inorganic phosphate.The main manifestations include non–diabetic glucosuria, phosphaturia, renal tubular acidosis. Among cytostatic drugs, ifosfamide and platinum most often cause SF, while imatinib usually leads to hypophosphatemia [7,8,12]. Some drugs (for example, cisplatin) can also cause the development of "salt–losing kidney" with damage to the proximal tubules and loop of Henle. As a result of impaired reabsorption of water, sodium, potassium, magnesium, polyuria with increased excretion of the listed ions, expressed by a decrease in the total fluid volume, orthostatic hypotension are noted [7,13].The distal nephron is the main site of magnesium reabsorption. Hypomagnesia due to loss of magnesium in the urine is increasingly described with the use of new chimeric monoclonal antibodies to epidermal growth factor receptors, including cetuximab and panitumumab. The incidence of hypomagnesemia with these drugs ranges between 10% and 36%. Oral magnesium is the first line of therapy, but intravenous magnesium is required due to frequent gastrointestinal side effects that limit patient compliance and are not always effective. Hypomagnesemia usually resolves within 4–6 weeks after stopping the drug [7,8]. Vasopressin (antidiuretic hormone) increases the permeability of distal tubular and collecting duct cells to water, resulting in the excretion of more concentrated urine. This occurs as a result of the incorporation of water channels (aquaporins–2) into the apical membrane of epithelial cells of the distal tubules and collecting ducts.Chemotherapeutic drugs such as cisplatin and ifosfamide interfere with the activation of vasopressin, leading to the development of nephrogenic diabetes insipidus. Resolution of nephrogenic diabetes insipidus symptoms usually occurs within a few days to a few weeks after discontinuation of the drugs. Cyclophosphamide and vincristine are chemotherapeutic agents that, on the contrary, potentiate the release and action of vasopressin [7,8].Crystalline nephropathy is characterized by acute and/or chronic kidney damage due to precipitation and deposition of crystal deposits in the lumen of the tubules. The drug itself or its metabolites undergo crystallization, which depends on a number of factors, the most significant of which is a decrease in the volume of intravascular fluid. Clinical conditions that are accompanied by a decrease in the rate of urine flow predispose to the precipitation of crystals.Despite a large number of reports describing drug–induced acute interstitial nephritis, this pathology is quite rare after the use of conventional drug regimens. The exception is new biological drugs – monoclonal antibodies that modulate antitumor T–cell immunity [7,14]. In some cases, acute interstitial nephritis can transform into chronic. This situation usually occurs with a combination of drug– and patient–specific factors (excessive drug concentration, use of other nephrotoxic drugs, as well as concomitant diseases such as diabetes mellitus and arterial hypertension). There is data on the development of a similar effect over several months/years when using nitrosourea drugs. They are characterized by dose–dependent nephrotoxicity, which is more pronounced when using streptozocin and semustine compared to carmustine and lomustine [6,7,12].However, the "classic" nephrotoxic cytostatics are alkylating agents (ifosfamide, platinum) and antimetabolites (methotrexate). Ifosfamide is widely used to treat various solid tumors, as well as Hodgkin's and non–Hodgkin's lymphomas. It is a structural analogue of cyclophosphamide. The nephrotoxic properties are possessed by the metabolite of ifosfamide – chloroacetaldehyde, which causes tubular damage. An important role in this process is also played by the expression of cytochrome p450, responsible for the metabolism of ifosfamide into toxic substrates. In addition, basolateral absorption of ifosfamide, unlike cyclophosphamide, occurs with the help of the OCT–2 transporter, which is insensitive to the latter agent. The risk of acute kidney injury when using ifosfamide is somewhat lower compared to cisplatin and correlates with the time of drug elimination. Independent risk factors for its nephrotoxicity include a cumulative dose greater than 100 g/m2 and previous use of cisplatin [3,15].More often than acute tubular necrosis, ifosfamide causes isolated proximal tubular dysfunction, which can manifest as either Fanconi syndrome or isolated renal tubular acidosis. A fairly common complication of ifosfamide therapy is hemorrhagic cystitis. Its development is provoked by one of the drug's metabolites formed in the urine – acrolein. The antidote is uromitexan – a sulfur–containing substance (2–mercaptoethanesulfonate), which, interacting with the double bond in the acrolein molecule, forms a stable non–toxic thioether. In addition, uromitexan inhibits the formation of acrolein from 4–hydroxy metabolites of ifosfamide and thereby reduces its concentration in the urine [6,8,9]. Cisplatin is prescribed for a large number of solid tumors and lymphoma (about 30 types of tumors). Dose–dependent acute tubular necrosis with the use of this drug develops in 20–30% of patients, usually between the 7th and 10th day after administration. Cisplatin can also lead to isolated proximal tubulopathy (Fanconi syndrome, proteinuria, increased phosphaturia and natriuria). The risk of developing CKD increases in patients who have received 3 cycles of therapy (13.8% of patients) or more (20.9% of patients). Risk factors for nephrotoxicity during cisplatin therapy are age, concomitant pathology, ECOG status, decreased SCF (SCF less than 50 ml/min/1.73 m2, according to some authors, is an absolute contraindication for prescribing this drug) [9,16]. Cisplatin causes AKI in several ways.The main mechanism is oxidative damage associated with the hydrolysis of chloride ions and the formation of hydroxyl radicals. In addition, it can be realized through OCT–2. As a result, epithelial cells accumulate cisplatin, the metabolites of which cause oxidative stress and the production of proinflammatory cytokines. In addition, TNF–α aggravates apoptosis processes. Cisplatin can also directly cause cell death by activating a number of signaling pathways, such as the synthesis of the p53 protein. Finally, cisplatin can damage the vessels of the microcirculatory bed of the kidneys. Second–generation (carboplatin) and third–generation (oxaliplatin) platinum drugs have less nephrotoxicity due to the absence of chloride ions and reduced absorption by tubular cells using OCT–2. However, at high doses and in patients with appropriate factors, these drugs can cause acute tubular necrosis [9,15,16].Prevention of acute kidney injury when using platinum drugs includes adequate hydration and discontinuation of all potentially nephrotoxic drugs. A regimen consisting of prehydration using isotonic sodium chloride solution at a rate of 100 ml/h for 12 h before drug administration and continuous infusion of sodium chloride solution during and for at least two days after treatment with cisplatin is recommended without the use of diuretics, which can worsen renal function. In order to prevent nephropathy due to increased formation of uric acid (maximum concentrations are noted 3–5 days after administration), allopurinol or agents that cause alkalinization of urine are prescribed. Other preventive measures include the use of glutathione analogues – amifostine and sodium thiosulfate. However, these drugs are not very well tolerated (they can cause nausea and vomiting) and can reduce the antitumor effect of cytostatics.Therapy for cisplatin–induced acute tubular necrosis begins with discontinuation of the next dose of the drug. Magnesium preparations are prescribed. In the presence of severe electrolyte (hyperkalemia) and metabolic disorders, renal replacement therapy may be required. Sodium thiosulfate and other antioxidant drugs can be prescribed not only for prevention, but also for the treatment of acute tubular necrosis, but side effects and unproven clinical efficacy limit its use. Another theoretical possibility for preventing the nephrotoxic effect of platinum drugs is to prescribe drugs that compete for binding to OCT–2, such as cimetidine, but this option has not been proven clinically. The use of N–acetylcysteine, vitamin C is also unproven [9,13,16]. Currently, a number of clinical trials are being conducted to study the preventive effect of histone deacetylase (HDAC) inhibitors, which increase the expression of bone morphogenetic protein–7 (BMP–7) through epigenetic modification. Experimental studies of thalidomide in combination with cisplatin and curcumin in combination with cisplatin in rat breast cancer are also considered very promising. The use of the drug tempol, which is piperidine nitroxide, a class of stable free radicals with antioxidant activity that protect mammalian cells, in particular, from hydrogen peroxide, superoxide and tert–butyl hydroperoxide, is being studied as a chemo– and radioprotector. The antimetabolite methotrexate is used in a number of solid tumors, such as breast cancer, ovarian cancer, as well as in lymphomas and leukemia, and is also used in some autoimmune diseases (rheumatoid arthritis, psoriasis). The mechanism of action is associated with the inhibition of dehydrofolate reductase, a key enzyme of the folate pathway required for pyrimidine synthesis. The drug blocks the synthesis of RNA and DNA in rapidly dividing tumor cells. Up to 90% of the drug is excreted by the kidneys. Methotrexate is metabolized into two primary derivatives – 7–hydroxy–MTX and 2,4–diamino N10–methylpteroacid, which are, respectively, 6 and 10 times less soluble in urine compared to the original drug.Crystallization of these substances is the leading mechanism of methotrexate's damaging effects, although direct tubular toxicity may also play a role. Nephrotoxicity with methotrexate varies widely, from 1.8 to 12%. In most cases, peak serum creatinine concentrations occur 1 week after drug administration, with recovery 2–3 weeks later; however, in some situations, recovery may be delayed, increasing the risk of systemic toxicity of the drug, including myelosuppression and neurotoxicity [7,9]. Risk factors for acute kidney injury with methotrexate include: high doses of the drug; serum concentrations greater than 15 mmol/L at 24 h, 1.5 mmol/L at 48 h, 0.5 mmol/L at 72 h after administration, previous CKD, hypovolemia [9,12]. Prevention of methotrexate nephrotoxicity consists primarily of adequate hydration, alkalization of urine (pH 6–7 increases the solubility of methotrexate and its metabolites by 5–8 times), and the use of calcium folinate (leucovorin). The latter is a reduced form of folic acid and is used as an antidote to drugs that act as its antagonists. Leucovorin, unlike folic acid, does not require reduction by dihydrofolate reductase to convert it into tetrahydrofolate, which allows normalizing the disrupted process of DNA, RNA, and protein biosynthesis. The protective effect of calcium folinate is manifested only in relation to healthy cells. Due to these properties, the drug prevents the toxic effect of methotrexate on bone marrow and gastrointestinal tract cells [6]. The treatment regimen for the development of acute kidney injury includes the administration of leucovorin, but it does not significantly affect the already developed nephrotoxic effect of methotrexate. Glucarpidase is a recombinant enzyme that metabolizes methotrexate into non–toxic derivatives and reduces serum drug levels by 98% within 15 minutes. It is important to remember that methotrexate concentrations remain low for a long time after glucarpidase administration, and most patients do not require additional glucarpidase.Hemodialysis demonstrates high efficiency in decreasing methotrexate concentration, however, after the procedure, the drug concentration is quickly restored [7]. The algorithm of actions for the management of cancer patients at risk for developing nephrotoxicity is quite fully formulated and reflected in the Recommendations for monitoring renal function in cancer patients of the International Society of Geriatric Oncology [15]. The action plan includes:assessment of concomitant pathology;adequate hydration;assessment of the estimated glomerular filtration rate using one of the calculation formulas;dose adjustment for patients with impaired renal function before each administration of the drug;use of drugs with the least nephrotoxicity and/or antidotes to prevent nephrotoxicity;avoidance of combined administration of drugs that potentiate the nephrotoxic effect.
4. Conclusions
Antitumor drugs cause various types of kidney damage, including glomerular, tubulointerstitial damage, electrolyte disturbances, clinically manifested by acute kidney injury with the possibility of transformation into chronic kidney disease. Knowledge of risk factors for the development of nephrotoxicity associated with both the patient and the cytostatic drugs used, adequate assessment of the excretory function of the kidneys, prevention and timely treatment of kidney damage during antitumor therapy play an important role in the management of patients with cancer. A multidisciplinary approach to solving this problem will significantly improve the treatment outcomes of patients.
References
| [1] | Khamidova D.T., Rakhimov A.A. Diagnostic and treatment strategies in modern oncology. Journal of Medical Sciences. 2020; 5 (2): 34–41. |
| [2] | Umarov S.I., Sodikov J.F. Prevalence and prevention of oncological diseases. Medical Research. 2021; 2 (3): 45–52. |
| [3] | Eggink F.A., Vermue MC, Van der Spek C. The impact of centralization of services on treatment delay in ovarian cancer: A study on process quality.//Int J Qual Health Care. 2017 Aug 22: 1–7. |
| [4] | Mustafoev Z.M. Comparative description of morphometric parameters of kidneys in polypharmacy of anti-inflammatory drugs. 14.00.02 – Morphology. Doctor of Philosophy (PhD) Dissertation in Medical Sciences, Bukhara - 2023. |
| [5] | Fastova O.N. Histomorfometricheskie parametris pochechnyx telets krys razlichnyx agezrastnyx grupp na fone ingalyatsionnogo vozdeystvya toluene s primeneniem korektorov / O. N. Fastova // General pathology and pathological physiology. - K: 2014, No. 2. - S. 67-72. |
| [6] | Fazilbekova Z.N. Dynamics of heart rhythm variability indicators against the background of basic treatment in patients with chronic kidney disease stage III-IV, 14.00.05 - Internal medicine, Doctor of Philosophy (PhD) dissertation, Tashkent - 2025. |
| [7] | Korman DB. Basic anti-inflammatory chemotherapy. Prakticheskaya meditsina, M., 2006: 518; [Corman DB. Fundamentals of antitumor chemotherapy. Practical medicine, M., 2006: 518]. |
| [8] | Akhmedova N.Sh. Diagnostic predictors of the development of chronic kidney diseases and ways to prevent them, 14.00.05 - internal medicine, doctor of philosophy (PhD) dissertation, Tashkent - 2019. |
| [9] | Shvetsov M. Yu. Chronic kidney disease as an obshchemeditsinskaya problem: modern principles of nephroprophylaxis and nephroprotective therapy. Consilium Medicum. 2014; 07: 51–64. |
| [10] | Lameire N. Nephrotoxicity of recent anti-cancer agents. Clin Kidney J 2014; 7: 11–12. |
| [11] | Zupancic M, Shah PC, Shah-Khan F. Gemcitabine-associated thrombotic thrombocytopenic purpura. Lancet Oncol 2007; 8: 634–641. doi: 10.1038/cddis.2017.552. |
| [12] | Volkova MA. Clinical oncohematology. Medicine, M., 2007: 1120. |
| [13] | Ubaidullaeva B.N. Clinical-laboratory characteristics of anemia in patients with chronic kidney disease in the terminal stage 14.00.05 - Internal diseases. Doctor of Philosophy (PhD) Dissertation in Medical Sciences, Tashkent- 2021. |
| [14] | Aytbaev K.A., Murkamilov I.T., Fomin V.V. Nephrogenic anemia: new physiological approaches to therapy and basic imitation of hypoxic responses Almanakh clinical medicine. 2017. – #7. 45. S. 565–574. |
| [15] | Burnasheva E.V., Shatoxin Yu.V., Snejko I.V., Matsuga A.A. Anti-inflammatory therapy for cystic fibrosis. Nephrology. 2018; 22 (5): 17–24. |
| [16] | Abdullaev H.N. Early signs of malignant tumors and reasons for late referral of oncology patients to primary care. Methodical use, Bukhara, 2018. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML