-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3209-3213
doi:10.5923/j.ajmms.20251509.81
Received: Sep. 6, 2025; Accepted: Sep. 24, 2025; Published: Sep. 29, 2025

Clinical and Laboratory Features of Antibiotic-Associated Diarrhea in Young Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShavdirova Gulbonu Mansurovna, Rabbimova Dilfuza Toshtemirovna
Samarkand State Medical University, Samarkand, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Antibiotic-associated diarrhea (AAD) is one of the most frequent complications of antibacterial therapy in early childhood. Due to the morphofunctional immaturity of the gastrointestinal tract and the immune system, its clinical course is highly variable, requiring a differentiated diagnostic and therapeutic approach. The incidence of AAD in young children ranges from 5% to 30%, with the highest rates observed in preterm infants and those under one year of age. This is largely explained by the immaturity of the intestinal microbiota and immune system. In the post-COVID period, the irrational use of antibiotics has further increased the prevalence of AAD, emphasizing the need for improved methods of diagnosis, severity assessment, and treatment.
Keywords: Antibiotic-associated diarrhea, Clostridioides difficile, Fecal calprotectin, Young children
Cite this paper: Shavdirova Gulbonu Mansurovna, Rabbimova Dilfuza Toshtemirovna, Clinical and Laboratory Features of Antibiotic-Associated Diarrhea in Young Children, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3209-3213. doi: 10.5923/j.ajmms.20251509.81.
Article Outline
1. Introduction
- Antibiotic-associated diarrhea (AAD) is one of the most frequent complications of antibacterial therapy in early childhood, with an incidence ranging from 5% to 30%, reaching the highest rates in preterm infants and children under one year of age [1]. According to WHO, AAD is defined as the occurrence of ≥3 unformed stools per day during or within 8 weeks after antibiotic treatment, in the absence of other causes [1].The role of Clostridioides difficile in pediatric AAD remains controversial, as many infants and young children are asymptomatic carriers [2,3]. Globally, the irrational use of antibiotics—particularly in outpatient pediatric practice—contributes to both antibiotic resistance and the growing prevalence of AAD [3].AAD not only worsens the clinical course of underlying diseases but also increases healthcare costs due to prolonged hospitalization and the need for additional therapy. Current challenges include the limited availability of diagnostic methods, lack of validated severity assessment tools, and insufficient evidence-based approaches for management in young children.Recent studies highlight the importance of gut microbiota disturbances, the pathogenic role of C. difficile, and the potential of early diagnostic markers such as fecal calprotectin and C. difficile toxins [4]. Personalized antibiotic strategies and adjunctive therapies, including lactoferrin, are being actively investigated, but standardized management protocols in pediatrics remain to be developed [5].
2. Methodology of the Study
- A single-center observational (prospective–retrospective) study was conducted during 2023–2025. The analysis included 140 young children (aged 1 month to 3 years) who underwent inpatient treatment with clinically confirmed antibiotic-associated diarrhea (AAD).Definition of AADA case of antibiotic-associated diarrhea (AAD) was established in the presence of the following:ü use of systemic antibacterial agents within the preceding 2–8 weeks;ü occurrence of liquid or watery stools ≥3 times per day;ü confirmation by laboratory and/or instrumental methods.Diagnostic approaches followed the ESPGHAN guidelines (2020).Inclusion criteriaü Age 1 month to 3 years;ü Hospitalization for treatment;ü Fulfillment of the AAD case definition.ü Exclusion criteriaCongenital gastrointestinal pathology:1. Severe somatic comorbidities;2. Viral or parasitic intestinal infections.Patient stratificationPatients were allocated into two main groups:- Infectious AAD, subdivided into:- Confirmed Clostridioides difficile infection;Predominance of opportunistic flora (Enterobacter spp., Klebsiella spp., Proteus spp., and others).Non-infectious AAD, defined as the absence of significant infectious etiology based on coprological and microbiological findings.Age stratificationFor analytical purposes, patients were grouped into three age intervals:ü 0–6 months,ü 7–12 months,ü 1–3 years.Data Collection and ExaminationClinical and anamnestic data: age, sex, type of feeding, information on current/previous antibiotic therapy (class, route of administration, duration, repeated courses), comorbidities, signs of dehydration and intoxication, and duration of diarrhea.Laboratory methods: complete blood count (leukocytosis, hemoglobin), C-reactive protein (CRP), coprological examination, bacteriological stool culture, and verification of Clostridioides difficile (toxin testing/PCR according to the local protocol).Severity assessment: a standardized clinical–laboratory severity scoring scale, adapted for inpatient settings, was applied to ensure comparability between subgroups.Outcomes and IndicatorsPrimary outcomes:1. Distribution of AAD by etiology (infectious vs. non-infectious) and clinical subtypes;2. Age distribution of cases within each subtype.Secondary outcomes:ü Intensity of clinical and laboratory inflammatory response;ü Severity by the standardized scale;ü Duration of diarrheal syndrome;ü Requirement for etiotropic therapy in infectious forms.
3. Analysis and Results
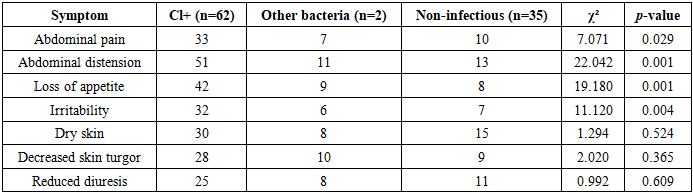
- Age distributionIn patients with Clostridioides difficile (Cl+), the peak incidence of AAD was observed at 6–12 months (37.1%) and 1–3 years (40.3%), with statistically significant differences compared to the non-infectious group at these ages (p < 0.05). In cases associated with other opportunistic flora (Enterobacter, Klebsiella, Proteus spp.), the highest prevalence was recorded at 3–6 months and 6–12 months, although significant differences were confirmed only in the youngest subgroup (p < 0.05).In the combined infectious group, incidence was also maximal at 6–12 months and 1–3 years, while in the non-infectious group AAD was most common in infants <3 months, with a decline in frequency at older ages.Temperature profileü Normal (36–37°C): less frequent in Cl+ (11.3%) vs. non-infectious (25.7%), showing a trend toward higher inflammatory activity (p = 0.067).ü Subfebrile (37–38°C): most common across all groups, especially non-infectious AAD (57.1%). A significant difference was found only in the subgroup with other flora (30.4% vs. 57.1%, p = 0.047).ü Febrile (38–39°C): markedly higher in infectious AAD (35.5–39.1%) vs. non-infectious (17.1%), significant in the combined group (p = 0.038).ü Hyperpyrexia (>39°C): paradoxically more frequent in non-infectious AAD (25.7%) vs. Cl+ (6.45%), p = 0.008, likely reflecting severe comorbid conditions rather than infectious activity.Clinical symptomatologyComparative χ²-analysis revealed significant intergroup differences:ü Abdominal pain: χ² = 7.071, p = 0.029ü Abdominal distension: χ² = 22.042, p < 0.001ü Loss of appetite: χ² = 19.180, p < 0.001ü Irritability: χ² = 11.120, p = 0.004The most frequent symptoms in Cl+ were abdominal distension (82.3%), loss of appetite (67.7%), and abdominal pain (53.2%), while in non-infectious AAD, dry skin (42.8%) was predominant, with lower frequency of other symptoms.InterpretationThese findings highlight:1. The age-specific distribution of AAD subtypes;2. The higher inflammatory response in infectious forms, especially Cl+;3. The diagnostic relevance of abdominal distension, anorexia, and abdominal pain as clinical indicators of infectious AAD in early childhood.
|
|

|
|

4. Conclusions
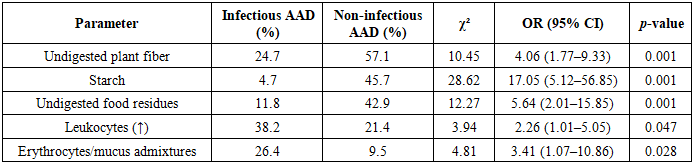
- Coprological profile clearly differed depending on the etiology of AAD:In infectious AAD, inflammatory signs predominated: leukocytes were present in 100% of cases versus 42.9% in non-infectious AAD (p < 0.001), consistent with a more pronounced neutrophilic response. In non-infectious AAD, markers of maldigestion and accelerated transit prevailed: significantly more frequent detection of fiber (57.1% vs. 24.7%; p = 0.001; OR = 4.06), starch (45.7% vs. 4.7%; p = 0.001; OR = 17.05), undigested residues (42.9% vs. 11.8%; p = 0.001; OR = 5.63), and crystals (94.3% vs. 72.9%; p = 0.009; OR = 6.12). Mushy stools were more frequent in non-infectious AAD (28.6% vs. 15.3%), but the difference did not reach statistical significance (p = 0.094). Yeast-like fungi were detected in 29.4% of infectious cases and were absent in non-infectious AAD (p = 0.001), reflecting possible secondary colonization under dysbiosis and antibiotic therapy.Fecal calprotectin proved to be a sensitive differential diagnostic marker of intestinal inflammation:ü Highest levels were found in Clostridioides difficile–associated AAD (393.65 ± 39.23 µg/g);ü Moderately elevated levels were recorded in AAD caused by other bacteria (195.45 ± 24.49 µg/g);ü Levels were substantially lower in non-infectious AAD (85.2 ± 11.7 µg/g);ü Healthy controls remained within normal limits (31.6 ± 3.82 µg/g);ü All intergroup differences were statistically significant (p ≤ 0.001), confirming the gradient of inflammation: Cl+ → other bacteria → non-infectious → control.Severity of AAD was not linearly dependent on the severity of the underlying disease. Severe forms of AAD, including toxigenic C. difficile colitis, developed even in children with relatively mild primary diagnoses (e.g., community-acquired pneumonia, tonsillopharyngitis). Conversely, in children with severe underlying conditions (e.g., sepsis, severe pneumonia, neuroinfection), AAD often presented with only mild to moderate severity. This highlights the necessity of independent risk and severity stratification for AAD, rather than extrapolation from the severity of the underlying illness.
5. Recommendations
- Diagnostic algorithm for stratification of AAD in children aged 1 month–3 years:• Step 1: Confirm antibiotic exposure (2–8 weeks) and ≥3 unformed stools/day.• Step 2: Perform baseline laboratory and coprological evaluation:Leukocytes → marker of inflammation.Fiber, starch, undigested residues, crystals → markers of maldigestion/accelerated transit.• Step 3: Fecal calprotectin as a triage test of inflammation:High values (e.g., >250 µg/g, per protocol) → priority exclusion of CDI (toxin/PCR testing) and other bacterial causes.Relatively low values in the presence of excess fiber/starch/residues → focus on maldigestion/accelerated transit (non-infectious etiology).