-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3187-3191
doi:10.5923/j.ajmms.20251509.77
Received: Aug. 29, 2025; Accepted: Sep. 25, 2025; Published: Sep. 29, 2025

Laparoscopic Native Tissue Repair for Post-Hysterectomy Apical Prolapse: A Prospective Comparative Study of Clinical Outcomes and Safety
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLYuldashev Sanjar Keldiyarovich
Republican Specialized Scientific and Practical Medical Center for Maternal and Child Health, Tashkent, Uzbekistan
Correspondence to: Yuldashev Sanjar Keldiyarovich, Republican Specialized Scientific and Practical Medical Center for Maternal and Child Health, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article presents the results of a prospective study evaluating the efficacy of laparoscopic treatment of apical prolapse after hysterectomy using patients’ own tissues. The aim of the study was to assess clinical outcomes, safety, and functional recovery within an organ-preserving approach. The study included patients who underwent laparoscopic fixation of the vaginal vault without the use of synthetic materials. Anatomical and functional outcomes, recurrence rates, and postoperative quality of life were evaluated. The findings demonstrate high efficacy of the method, a low complication rate, and satisfactory functional results. The use of autogenous tissues avoided risks associated with implants and ensured a stable clinical effect. The results support the feasibility and advisability of this approach in the surgical correction of prolapse.
Keywords: Apical prolapse, Post-hysterectomy prolapse, Laparoscopic treatment, Autogenous tissues, PFIQ-7 (Pelvic Floor Impact Questionnaire), PFDI–20 (Pelvic Floor Distress Inventory), Prospective study, Pelvic floor
Cite this paper: Yuldashev Sanjar Keldiyarovich, Laparoscopic Native Tissue Repair for Post-Hysterectomy Apical Prolapse: A Prospective Comparative Study of Clinical Outcomes and Safety, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3187-3191. doi: 10.5923/j.ajmms.20251509.77.
1. Introduction
- Pelvic organ prolapse (POP) remains one of the most pressing issues in contemporary gynecology, exerting a substantial impact on women's quality of life, as well as their physical and psycho-emotional well-being. [12] Apical prolapse, which includes vaginal vault descent following hysterectomy, represents one of the most complex forms of this pathology and necessitates advanced, organ-preserving therapeutic approaches. [2]According to global epidemiological studies, the prevalence of pelvic organ prolapse among women ranges from 3–6% in the general population to as high as 50% among parous women. [7] Data from the Global Burden of Disease Study 2021 indicate that in 2021, the age-standardized prevalence rate of POP was 2,769.4 per 100,000 women, with the number of years lived with disabling symptoms reaching 8.5 per 100,000. [10] The absolute number of women affected by POP continues to rise—from 8.4 million in 1990 to 14 million in 2021. [4] Projections suggest that by 2036, the global number of women with POP will reach 156 million, a trend driven by population aging and increased life expectancy.Post-hysterectomy apical prolapse occupies a distinct position within the spectrum of POP. [9] Following uterine removal, the risk of vaginal vault prolapse increases significantly, particularly in women with pre-existing connective tissue weakness, a history of multiple childbirths, and concomitant pelvic floor disorders. International registry data show that the incidence of apical prolapse after hysterectomy ranges from 11–20% within ten years postoperatively, with a subset of patients requiring repeat surgical intervention. [14]Conventional methods for correcting apical prolapse often involve the use of synthetic implants. [5] While these materials offer high mechanical strength, their application is associated with risks such as erosion, infectious complications, and chronic pelvic pain. In recent years, there has been a discernible shift away from synthetic materials toward organ-preserving techniques utilizing the patient’s own (native) tissues. [13] This approach aims to reduce the incidence of complications, enhance biocompatibility, and ensure long-term functional outcomes.Laparoscopic access in prolapse surgery has gained widespread adoption due to its minimally invasive nature, reduced hospitalization and recovery times, and the ability to achieve precise anatomical reconstruction of the pelvic floor. [3] However, prospective studies evaluating the clinical efficacy of laparoscopic correction of post-hysterectomy apical prolapse using native tissues remain limited—particularly in low- and middle-income countries, where access to advanced synthetic materials is restricted. [1]Thus, investigating the outcomes of laparoscopic vaginal vault suspension using autologous tissues in patients with post-hysterectomy apical prolapse represents a pertinent objective in modern gynecology. The data obtained may contribute to the optimization of surgical strategies, reduction in complication rates, and improvement in patients’ quality of life.Objective of the Study. To evaluate the clinical efficacy and safety of laparoscopic correction of apical prolapse using autologous tissues in post-hysterectomy patients within the framework of a prospective study.
2. Materials and Methods
- We conducted a comparative longitudinal study involving 245 female patients aged 29 to 76 years (mean age: 46.66 ± 11.81 years) diagnosed with pelvic organ prolapse (POP), who underwent inpatient treatment at the Department of Operative Gynecology of the Republican Specialized Scientific and Practical Medical Center for Obstetrics, Gynecology, and Neonatology between 2022 and 2024. The patients were divided into two groups based on the surgical correction method employed:• The main group (MG) comprised 123 patients aged 29 to 75 years (mean age: 46.02 ± 11.05 years; median [Me] = 44 years; mode [Mo] = 41 years) diagnosed with POP.• The comparison group (CG) included 122 patients aged 29 to 76 years (mean age: 47.29 ± 12.57 years; Me = 43.5 years; Mo = 37 years) also diagnosed with POP.All patients in the study underwent a novel laparoscopic technique for apical prolapse correction utilizing autologous tissues. No synthetic materials were used in this group. In contrast, patients in the comparison group received conventional surgical treatment for POP, including pectopexy and sacrocolpopexy.Outcome assessment was conducted using the following parameters:• Anatomical outcomes based on the Pelvic Organ Prolapse Quantification (POP-Q) system at 6 and 12 months postoperatively.• Functional outcomes assessed via validated questionnaires: the Pelvic Floor Distress Inventory (PFDI-20) and the Pelvic Floor Impact Questionnaire (PFIQ-7).• Postoperative complications classified according to the Clavien–Dindo system.It is noteworthy that no intraoperative complications were observed in either study group. All patients in both cohorts were managed in accordance with the Enhanced Recovery After Surgery (ERAS) protocol.
3. Results and Discussion
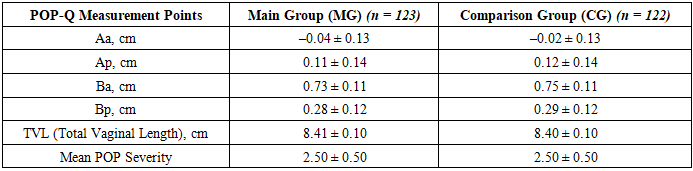
- Prior to surgery, all patients in both groups underwent assessment of prolapse severity and localization of measurement points according to the POP-Q classification system. In the main group (MG), the average degree of pelvic organ prolapse was 2.50 ± 0.50. Of these, 62 women (50.41%) were diagnosed with stage II prolapse, while the remaining 61 women (49.59%) presented with stage III prolapse. In the comparison group (CG), the average degree of prolapse was likewise 2.50 ± 0.50, with an equal distribution: 61 women (50.00%) had stage II prolapse and 61 (50.00%) had stage III prolapse (see Table 1).
|
|
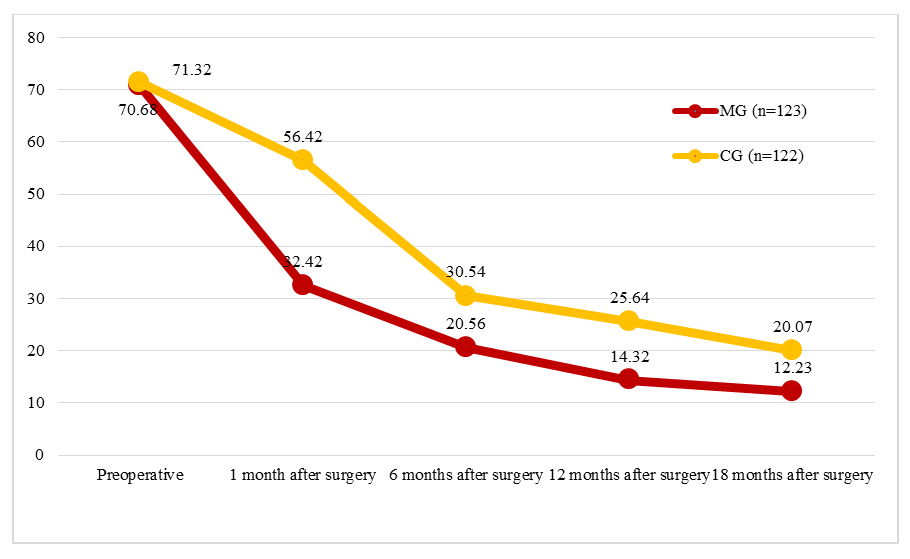 | Figure 1. Dynamics of Subjective Symptom Scores Before and After Surgery According to the PFIQ-7 Questionnaire |
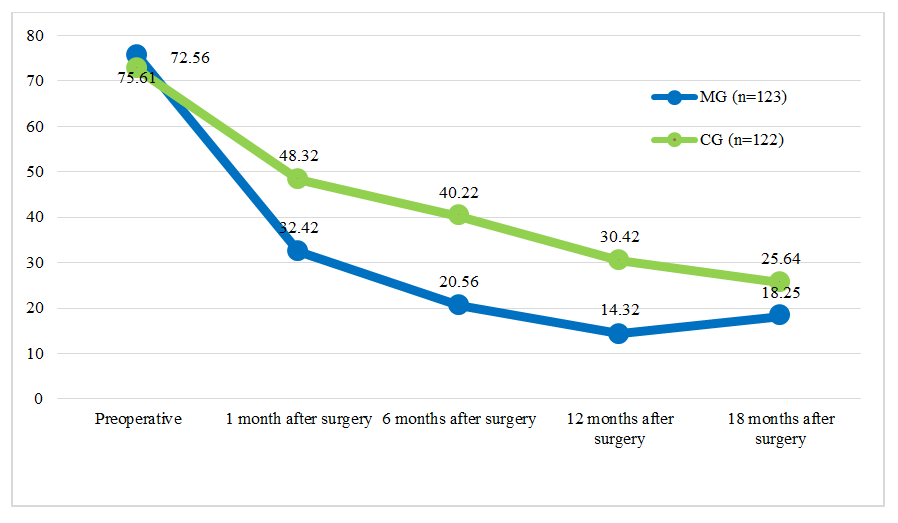 | Figure 2. Dynamics of Subjective Symptom Scores Before and After Surgery According to the PFDI-20 Questionnaire |
4. Conclusions
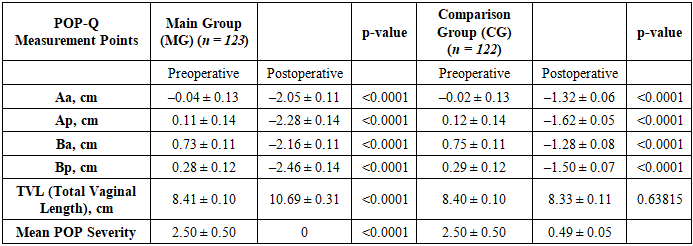
- 1. Preoperative indicators based on the POP-Q classification and subjective quality of life assessments (PFIQ-7 and PFDI-20 questionnaires) were comparable between both groups, with no statistically significant differences identified (p ≥ 0.05).2. Six months after surgery, complete anatomical restoration was achieved in all patients of the main group (MG), with a mean POP severity of 0. In contrast, 48.36% of patients in the comparison group (CG) retained stage I prolapse.3. Laparoscopic vaginal vault suspension using autologous tissues (MG) resulted in significantly greater improvement in anatomical parameters according to POP-Q compared to the comparison group (p < 0.0001).4. Both groups demonstrated statistically significant improvements in quality of life based on PFIQ-7 and PFDI-20 scores (p < 0.001). However, the MG showed a greater difference in pre- and postoperative PFIQ-7 scores (58.45 ± 0.95 vs. 51.25 ± 0.81 points), indicating a more pronounced clinical effect.5. The technique applied in the MG exhibited high efficacy and safety, with no recurrence of prolapse and a minimal rate of complications in the early postoperative period.Conclusion. The results of this prospective study clearly demonstrate that the laparoscopic technique we developed for treating post-hysterectomy apical prolapse using native (autologous) tissues is a highly effective and safe surgical method for correcting this pathology. The organ-preserving approach enabled complete resolution of prolapse in all patients in the main group, as confirmed by objective POP-Q classification data and the absence of recurrence during the follow-up period.Significant improvements in functional outcomes and quality of life were observed, reflected in the marked reduction of scores on the PFIQ-7 and PFDI-20 questionnaires. These changes indicate not only anatomical restoration of the pelvic floor but also a substantial reduction in clinical symptoms, enhanced physical activity, and improved psycho-emotional well-being among patients.Avoiding the use of synthetic implants eliminated the risk of specific complications such as erosion, chronic pelvic pain, and infectious processes—an especially important consideration in the context of minimizing invasiveness and enhancing biocompatibility of surgical interventions. The laparoscopic approach ensured minimal tissue trauma, shorter hospitalization, and rapid recovery, increasing the appeal of the method for both patients and surgeons.Comparison with the control group revealed clear advantages of the proposed technique in terms of anatomical outcomes, recurrence rates, and patient satisfaction. These findings support the consideration of laparoscopic vaginal vault suspension using autologous tissues as the preferred method for patients with post-hysterectomy apical prolapse, particularly in cases where synthetic materials are contraindicated or undesired.