-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3158-3160
doi:10.5923/j.ajmms.20251509.70
Received: Aug. 22, 2025; Accepted: Sep. 23, 2025; Published: Sep. 29, 2025

Early Prognosis and Prevention of Neonatal Disorders Associated with Maternal Endotoxicosis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMamarizaev Ibrokhim Komiljonovich1, Ibragimova Marina Fedorovna2, Shavazi Nargiz Nuralievna3
1Assistant, Free Applicant of the Department of 1-Pediatrics and Neonatology, Samarkand State Medical University, Samarkand, Uzbekistan
2PhD, Associate Professor of Department №1-Pediatrics and Neonatology, Samarkand State Medical University, Samarkand, Uzbekistan
3DSc, Associate Professor, Head of the Department of Obstetrics and Gynecology N 3, Samarkand State Medical University, Samarkand, Uzbekistan
Correspondence to: Mamarizaev Ibrokhim Komiljonovich, Assistant, Free Applicant of the Department of 1-Pediatrics and Neonatology, Samarkand State Medical University, Samarkand, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Relevance. Endotoxicosis in pregnant women poses a serious threat to the fetus and newborn, provoking hypoxia, metabolic disturbances, and neurovegetative dysfunctions. In the context of the high prevalence of inflammatory diseases and gestosis, the importance of preventing neonatal complications is steadily increasing. Aim. To evaluate prognostic and therapeutic approaches for preventing neonatal complications in newborns born to mothers with endotoxicosis. Materials and Methods. The study included 138 newborns divided into three groups: those receiving standard and additional antioxidant therapy (n=50), those receiving only standard therapy (n=48), and a control group (n=40). The levels of neuron-specific enolase (NSE) and uric acid in umbilical cord blood, neurosonographic findings, and Apgar scores were assessed. Statistical analysis was conducted using the Mann–Whitney test and ANOVA (p<0.05). Results. NSE and uric acid levels were significantly higher in newborns without additional therapy, correlating with increased frequency of hypoxia and neurological disorders. Combined therapy significantly reduced metabolic stress and improved both clinical and instrumental parameters. A biomarker-based risk stratification algorithm for neonatal complications was developed. Conclusion. Maternal endotoxicosis markedly increases the risk of neonatal complications. NSE and uric acid serve as reliable biomarkers for early diagnosis and prognosis. Combined therapy and risk stratification algorithms enhance the effectiveness of prevention and early treatment in high-risk newborns.
Keywords: Endotoxicosis, Newborns, Neuron-specific enolase, Uric acid, Prevention, Complications, Hypoxia, Perinatal pathology
Cite this paper: Mamarizaev Ibrokhim Komiljonovich, Ibragimova Marina Fedorovna, Shavazi Nargiz Nuralievna, Early Prognosis and Prevention of Neonatal Disorders Associated with Maternal Endotoxicosis, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3158-3160. doi: 10.5923/j.ajmms.20251509.70.
1. Introduction
- Endotoxicosis during pregnancy is a pathological condition caused by the accumulation of lipopolysaccharides (LPS) in the systemic circulation structural components of Gram-negative bacterial cell walls. These molecules activate the innate immune response and trigger cascades of inflammatory reactions. Given the physiological immunodepression in pregnant women, even minor translocation of endotoxins from the gut or chronic infection foci can induce systemic inflammation and exert a pronounced effect on the fetoplacental complex. [1,3] Recent studies have shown that endotoxicosis is associated with impaired placental barrier function, increased vascular permeability, hypoxic-ischemic changes, oxidative stress activation, and disturbances in purine metabolism. These processes contribute to intrauterine growth restriction, preterm birth, perinatal infections, and neonatal neurological disorders. The issue is particularly urgent in the context of widespread chronic inflammatory diseases, obesity, gestosis, and related conditions that exacerbate endotoxicosis. [4,5,6]Despite accumulated knowledge about its pathogenesis, early prediction of neonatal risk and the development of individualized preventive protocols remain unresolved. Identifying reliable biochemical markers that reflect systemic inflammation and oxidative stress is an important direction in modern perinatology. Such markers include neuron-specific enolase (NSE), which indicates neuronal damage, and uric acid (UA), associated with purine metabolism activation under hypoxia. [1,2,10] The aim of this study was to develop effective strategies for prevention and monitoring of neonatal complications in newborns of mothers with endotoxicosis, using prognostic biomarkers and differentiated therapeutic approaches. [7,9]
2. Materials and Methods
- The study was conducted at the Samarkand Branch of the Republican Specialized Scientific-Practical Medical Center of Motherhood and Childhood. A total of 138 newborns were examined and distributed into three groups:- Group I (n=50): newborns of mothers with endotoxicosis receiving standard and additional antioxidant therapy.- Group II (n=48): newborns of mothers with endotoxicosis receiving only standard therapy.- Group III (n=40): healthy newborns from healthy mothers (control).Clinical-anamnestic data, biochemical markers (NSE and uric acid levels), and neurosonography were used. Biomarkers were measured in umbilical cord serum by ELISA. Statistical processing employed the Mann–Whitney U test and ANOVA, with significance set at p<0.05.
3. Results
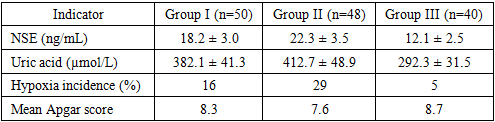
- Comparative analysis revealed significant differences between groups (p<0.001). NSE levels were markedly elevated in Groups I and II versus controls, reflecting neuroinflammation and hypoxic injury. Within the endotoxicosis cohort, NSE was lower in the combined-therapy group compared with standard therapy alone (18.2 ± 3.0 vs. 22.3 ± 3.5 ng/mL, p<0.01), indicating the therapeutic efficacy of antioxidant correction.Umbilical cord uric acid levels correlated with severity of endotoxicosis:- Group II: 412.7 ± 48.9 µmol/L- Group I: 382.1 ± 41.3 µmol/L- Control: 292.3 ± 31.5 µmol/LThe incidence of hypoxia (Apgar <7 at 1 min):- Group II: 29%- Group I: 16%- Control: 5% (p<0.01 between Groups I and II).Neurosonography demonstrated higher prevalence of periventricular leukomalacia (14.6%) and ventricular dilatation (18.7%) in Group II, compared with Group I (8% and 10%, respectively). Control values remained within physiological limits.Logistic regression confirmed that NSE >20 ng/mL and UA >400 µmol/L are independent predictors of severe neonatal complications. (Table 1)
|
4. Discussion
- These findings confirm the high pathogenic significance of maternal endotoxicosis in the formation of neonatal complications. NSE and uric acid demonstrated high sensitivity and specificity in early diagnosis of neurovegetative dysfunction and metabolic stress. Elevated levels correlated with hypoxia, lower Apgar scores, and neurological abnormalities, consistent with previous reports linking systemic inflammation and oxidative stress to fetoplacental insufficiency and intrauterine growth restriction.Particularly noteworthy is the therapeutic effect of combined therapy with antioxidants and purine metabolism correctors. In newborns receiving additional therapy, marked improvements were observed across all indicators: lower NSE and UA, improved neurosonographic findings, and higher adaptation scores. This underscores the potential for active modulation of pathogenetic mechanisms underlying neonatal complications.The developed biomarker-based risk stratification algorithm also demonstrated clinical potential, offering a tool for personalized neonatal monitoring. Its integration into clinical practice may enhance primary prevention and timely initiation of intensive therapy.
5. Conclusions
- Maternal endotoxicosis exerts a profound impact on fetal development, contributing to hypoxia, growth restriction, and neonatal complications. NSE and uric acid in umbilical cord blood are informative biomarkers reflecting intrauterine injury and predicting adverse neonatal outcomes. Combined therapy incorporating antioxidants and purine metabolism regulators significantly lowers biomarker levels, improves neonatal condition, and enhances adaptation. The proposed risk stratification algorithm provides an individualized preventive approach and can be effectively implemented in perinatal medicine.