-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3153-3157
doi:10.5923/j.ajmms.20251509.69
Received: Sep. 5, 2025; Accepted: Sep. 23, 2025; Published: Sep. 29, 2025

Molecular-Genetic Status of Colorectal Cancer
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIslamov Khurshid Jamshidovich
Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology, Tashkent, Uzbekistan
Correspondence to: Islamov Khurshid Jamshidovich, Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology, Tashkent, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study was conducted on the basis of the Department of Coloproctology of the Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology in Tashkent. The study included 78 patients with colorectal cancer (CRC) of stage II-IV of the disease who underwent surgical treatment in the department of Coloproctology of the Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology. Performing cytoreductive surgery on patients with colorectal cancer with liver metastases may help improve the quality of life of these patients in the long term.
Keywords: Colorectal cancer, Metastases, Cytoreductive surgery, Polychemotherapy
Cite this paper: Islamov Khurshid Jamshidovich, Molecular-Genetic Status of Colorectal Cancer, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3153-3157. doi: 10.5923/j.ajmms.20251509.69.
1. Introduction
- In the Republic of Uzbekistan, according to official statistics, 1,818 patients with colorectal cancer were identified in 2022, of which 290 patients (16.0%) were diagnosed with stage IV of the disease. 936 patients died from colorectal cancer in the country. The ratio of deaths to patients remains high, reflecting the effectiveness of ongoing anti-cancer measures, including diagnostic and treatment measures, at 51.5% in 2022 [3,7].Surgical treatment, as an independent method, is effective for colon cancer in stages I-II. In colon cancer of the I stage of the disease, the effectiveness of surgical intervention as an independent treatment method has been proven, in other cases - a preoperative course of radiation therapy is necessary. Approximately 25-40% of patients who received CRP treatment according to the radical program (stages I-II) develop disease recurrence or develop distant metastases [2]. Distant metastases, among patients with stage III of the disease, appear in almost 35% of cases after potentially radical treatment. In this case, the progression of the disease is due to the activation of tumor cells that migrated from the primary tumor site before surgery. To address this issue, adjuvant chemotherapy is prescribed worldwide [4,5,6].Thus, the increase in CRP morbidity worldwide, including in the Republic of Uzbekistan, and the high frequency of disease progression after treatment determine the relevance of this issue for the oncological service. Studying and identifying prognostic factors that influence long-term treatment outcomes will allow for individualized treatment of patients.Purpose of the research. Improvement of a multidisciplinary approach to the timely diagnosis of metastatic colorectal cancer.
2. Material and Methods
- This study was conducted on the basis of the coloproctology department of the Republican Specialized Medical Scientific and Practical Center of Oncology and Radiology in Tashkent.The retrospective group included data on 360 patients with stage II-IV colorectal cancer who received surgical treatment in the coloproctology department of the Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology (RSMPMCOR). The study did not include patients with primary multiple synchronous/metachronous malignant neoplasms, patients receiving surgical treatment for colorectal malformation in other medical institutions of the Republic of Uzbekistan.The diagnosis was made based on complaints, medical history, physical examination, morphological examination of tumor material, and data from instrumental and laboratory examination methods. Patients received adjuvant/non-adjuvant treatment in accordance with the current algorithms for the diagnosis and treatment of colorectal cancer patients, approved by the Ministry of Health of the Republic of Uzbekistan. The study material was: patients' peripheral blood, paraffin blocks of tumor tissue, fresh frozen tumor and normal colon tissue, isolated circulating tumor cells.The prospective group included data from 78 patients with metastatic colorectal cancer II-IV.The material for the study was fixed with 10% neutral formalin for 24 hours, poured into paraffin, and 3-4 μm thick sections were prepared on an Accu-Cut SRM 200 rotary microtome from the Sakura (Japan) company. The cuts were applied to highly adhesive glass and dried vertically in a thermostat at a temperature of 55-56°C for 10 hours.Extraction of total RNA preparations. Fragments of the colon tissue removed during the surgical intervention were crushed with a disposable sterile scalpel and placed in test tubes containing a lysing solution containing guanidine isothiocyanate, sodium citrate, sarcosil, and DTT.Analysis of multiple parallel microRNA sequencing data. Determining the expression level of microRNA using NGS technology involves comparing the nucleotide sequence of sequencing cDNA molecules in each sample with known microRNA nucleotide sequences presented in miRBase/mirGeneDB databases.When processing the initial research materials, IBM SPSS Statistics 23 (Stat Soft, USA) and MedCalc 19.3.0 (MedCalc Software bv, USA) programs were used.
3. Results
- The prospective study group included 78 patients (27 men and 51 women) diagnosed with metastatic colorectal cancer (stage IV of the disease), who underwent molecular genetic studies. The study included patients aged 26 to 74 years, with an average age of 59.2 years and a median age of 60.0 years. The average age of the men included in the study was 60.4 years, the median was 62.0 years, and the women were 58.6 and 60.0 years, respectively (p=0.352).In the vast majority of cases, colon cancer was diagnosed in 57 patients (73.1%), and rectosigmoid joint cancer in 21 patients (26.9%). The degree of tumor differentiation corresponded to 2-3 in 66 patients: 2 - 45 patients (57.7%), 3 - 21 (26.9%). Lymphovascular invasion was detected in 74 patients (94.9%), perineural invasion - in 71 (91.0%).The size of the primary focus (according to TNM classification category T) in 34 patients corresponded to T3 (43.6%), T4 - in 41 (52.6%) (Figure 1). Only in 11 patients were regional lymph nodes not affected, in 31 (39.7%) patients - regional lesion corresponded to the N1 category, in 36 (46.2%) - N3.
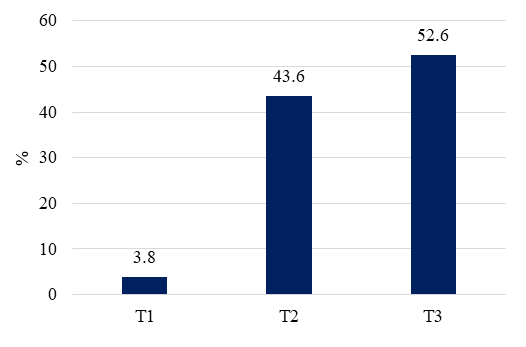 | Figure 1. Distribution of patients with metastatic colorectal cancer depending on the size of the primary focus |
|
|

|
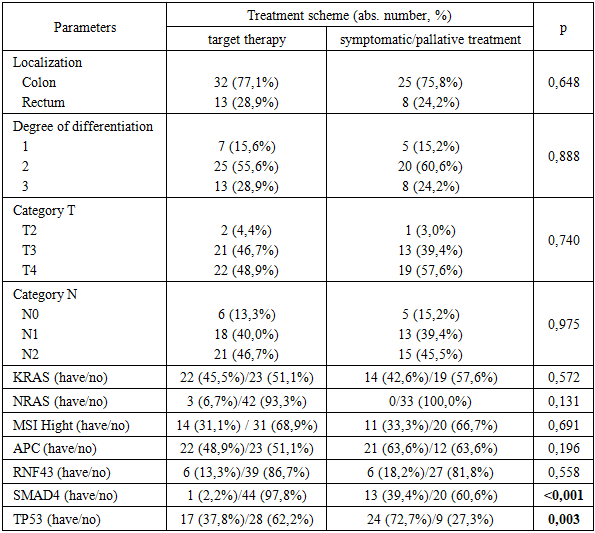
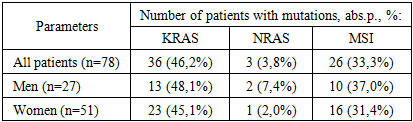
4. Conclusions
- Conducting a molecular genetic study among patients with metastatic colorectal cancer in the Republic of Uzbekistan made it possible to determine the frequency of a wide spectrum of genetic changes (available on the NGFR panel), as well as to assess the frequency of KRAS, NRAS mutations, and microsatellite instability (the most characteristic genetic changes in metastatic colorectal cancer) among patients in the Republic of Uzbekistan. Thus, KRAS mutations were detected in 36 patients (46.2%), NRAS - in 3 (3.8%), microsatellite instability (MSI) was determined in 26 (33.3%), mutations in the TR53 gene were detected in 41 patients (52.6%), in 29 (37.2%) - APC, in 14 (17.9%) - SMAD4, in 12 (15.4) - RNF43, in 10 (12.8%) - ARID1A. BRAF mutation was detected in only 3 patients, and BRCA (BRCA1 and BRCA2) - in 7 patients. Most of the identified molecular genetic changes were in combination with mutations in several genes.Molecular genetic testing for metastatic colorectal cancer is primarily conducted to determine the possibility of using targeted drugs for the treatment of the pathology. Correct administration of expensive targeted drugs allowed for an increase in overall 3-year survival from 20.1±8.1% (in the group of patients receiving symptomatic/paliative treatment) to 38.7±8.5% (in the group of patients receiving targeted therapy prescribed based on molecular genetic testing results) and the median overall survival from 16.0 months (95% CI 5.2-26.8 months) to 32.0 months (95% CI 25.0-39.0 months).The conducted research allowed us to develop an algorithm for treating patients with metastatic colorectal cancer, the application of which allows for an increase in the proportion of resectable foci, thereby increasing the life expectancy of patients with metastatic colorectal cancer.