-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3146-3149
doi:10.5923/j.ajmms.20251509.67
Received: Sep. 2, 2025; Accepted: Sep. 22, 2025; Published: Sep. 29, 2025

Clinical and Immunopathological Aspects of Microcirculatory Disorders in Children with Atypical Pneumonia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTashmatova Gulnoza Alayevna1, Obidova Baxtiyora Alijon qizi2
1DSc., Professor, Department of Pediatrics, Tashkent Medical University, Tashkent, Uzbekistan
2Assistant, Department of Propaedeutics of Children’s Diseases, Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Tashmatova Gulnoza Alayevna, DSc., Professor, Department of Pediatrics, Tashkent Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

According to the World Health Organization, pneumonia remains one of the leading causes of childhood mortality worldwide. Continuous efforts are being made to improve the etiological diagnosis and management of pediatric pneumonia. Objective: To identify the clinical and immunopathological features of microcirculatory disturbances in children with atypical pneumonia. Materials and Methods: A total of 57 children hospitalized in the pulmonology department of Tashkent State Medical University were examined. Depending on the etiological factor, patients with community-acquired pneumonia were divided into two groups: Group I – 27 children with atypical pneumonia of Mycoplasma pneumoniae etiology, and Group II – 30 children with typical bacterial pneumonia. Results: Comparative analysis revealed that the majority of Mycoplasma pneumoniae cases occurred in children older than 6 years (56.7%, p < 0.05), while typical bacterial pneumonia was more common in younger children under 6 years (p < 0.05). Children in Group I exhibited a more gradual onset of disease, most frequently presenting with subfebrile fever (56.5% vs. 26.7% in Group II, p < 0.05), dry cough (73.9% vs. 41.7%, p < 0.05), and moderately expressed intoxication symptoms. Conclusions: In children with Mycoplasma pneumoniae pneumonia, the disease was significantly more frequent after the age of six, and was characterized by gradual onset, subfebrile temperature, prolonged cough, and a tendency toward bronchial obstructive syndrome.
Keywords: Mycoplasma pneumoniae, Atypical pneumonia, Children, Immune imbalance, Microcirculatory dysfunction
Cite this paper: Tashmatova Gulnoza Alayevna, Obidova Baxtiyora Alijon qizi, Clinical and Immunopathological Aspects of Microcirculatory Disorders in Children with Atypical Pneumonia, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3146-3149. doi: 10.5923/j.ajmms.20251509.67.
1. Introduction
- Pneumonia remains one of the most significant causes of childhood morbidity and mortality worldwide. According to WHO and UNICEF, in 2019 pneumonia caused over 740,000 deaths in children under five years, representing 14% of all under-five mortality [9]. Global incidence remains high, with approximately 1,400 cases per 100,000 children annually, disproportionately affecting low- and middle-income countries [9]. Despite advances in vaccination and antimicrobial therapy, pneumonia continues to be a leading reason for pediatric hospitalizations in both developing and developed countries [2,3].In recent years, increasing attention has been paid to the role of atypical pathogens, particularly Mycoplasma pneumoniae. CDC surveillance reported a sharp rise in M. pneumoniae infections in 2024, with pediatric hospitalizations increasing from 2.12 per 1000 hospitalizations (2018–2023) to 12.49 per 1000 in 2024 [11]. In July 2024, M. pneumoniae accounted for 53.8% of community-acquired pneumonia (CAP) cases in children, compared to <5% in previous years [11]. Notably, while historically more common in school-aged children, recent outbreaks have also affected younger pediatric groups [11]. Comparable observations were reported in Europe, where ECDC highlighted periodic epidemics of M. pneumoniae every 3–7 years, with resurgence patterns altered following the COVID-19 pandemic [12].Atypical pneumonia differs from classical bacterial pneumonia caused by Streptococcus pneumoniae or Haemophilus influenzae by its gradual onset, subfebrile fever, prolonged cough, and less pronounced inflammatory markers [1,4,5]. Furthermore, M. pneumoniae infections often lead to extrapulmonary complications, including dermatological, neurological, and cardiovascular manifestations, reflecting its systemic impact [5,6]. Recent clinical reports emphasize that post-COVID epidemiological shifts have modified seasonal and age-related distribution, as well as radiological patterns of MPP, complicating timely diagnosis [11,12].From a pathophysiological perspective, M. pneumoniae has unique biological properties, enabling persistent colonization, modulation of host immunity, and induction of systemic inflammatory responses [5,6,8]. Immune dysregulation is characterized by T-cell imbalance, cytokine hyperproduction (IL-6, TNF-α), impaired IFN-γ responses, and sometimes elevated IL-17, which may serve as biomarkers of severe disease [12,13]. Importantly, these immune processes are linked with microcirculatory disturbances: endothelial dysfunction, capillary stasis, and impaired vascular tone regulation, which contribute to tissue hypoxia and chronic inflammation [7,8,13].Scientific novelty. While previous studies have described immune mechanisms in M. pneumoniae pneumonia, very few have simultaneously assessed immune dysregulation and microcirculatory abnormalities in children. The present study is among the first in our region to integrate clinical, immunological, and vascular assessments—including lymphocyte subpopulations, immunoglobulin levels, cytokine profiles, capillaroscopy, and laser Doppler flowmetry. This comprehensive approach provides novel insights into the systemic nature of atypical pneumonia in children, with potential implications for early diagnosis, prognostic evaluation, and targeted therapeutic strategies.
2. Materials and Methods
- A total of 57 pediatric patients hospitalized in the pulmonology department of Tashkent State Medical University were examined. Depending on the etiological factor, patients with community-acquired pneumonia were divided into two groups: Group I – 27 children with atypical pneumonia caused by Mycoplasma pneumoniae; Group II – 30 children with typical bacterial pneumonia.To establish reference laboratory values, an additional control group of 20 practically healthy children was examined. Among the 57 patients in the main cohort, there were 19 girls (33.3%) and 38 boys (66.7%), with a mean age of 7.08 ± 1.15 years (range 5–12 years).The following methods were employed: clinical examination (anamnesis, physical assessment, evaluation of respiratory insufficiency); laboratory tests (complete blood count, biochemical analysis, immunological profiling of lymphocyte subpopulations, immunoglobulins, and cytokines); instrumental studies (chest radiography/CT, spirometry, pulse oximetry, capillaroscopy, and laser Doppler flowmetry). Statistical analysis was performed using SPSS and Statistica software packages.
3. Results and Discussion
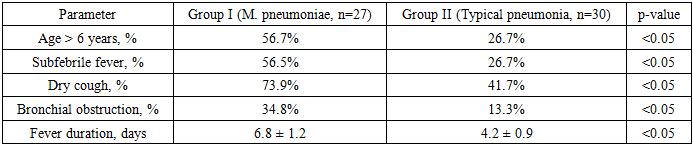
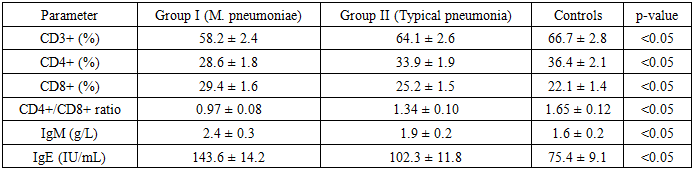
- Our comparative study of 57 pediatric patients with community-acquired pneumonia revealed significant clinical, laboratory, immunological, and microcirculatory differences between children with Mycoplasma pneumoniae pneumonia (Group I) and those with typical bacterial pneumonia (Group II). In addition, the results were benchmarked against 20 healthy controls, allowing us to identify deviations that are specific to atypical pneumonia and to interpret their pathogenetic implications.Clinical characteristics.The majority of M. pneumoniae cases occurred in children older than 6 years (56.7%, p < 0.05), whereas typical bacterial pneumonia was more frequent in children under 6 years of age (p < 0.05). This age-related distribution aligns with previous epidemiological observations that atypical pneumonia tends to dominate in school-aged populations, reflecting both exposure patterns and immune maturation [3,11].In terms of clinical presentation, children in Group I showed a more gradual onset of disease compared to the acute presentation in Group II. Subfebrile temperature was present in 56.5% of Group I versus 26.7% of Group II patients (p < 0.05), while dry cough was observed in 73.9% versus 41.7%, respectively (p < 0.05). These findings are consistent with the “walking pneumonia” concept, where M. pneumoniae infection often manifests with prolonged but relatively mild systemic symptoms [5].Notably, bronchial obstruction was diagnosed in 34.8% of Group I patients compared to 13.3% in Group II (p < 0.05). This supports the hypothesis that M. pneumoniae may act as a trigger of airway hyperreactivity and asthma exacerbations, as emphasized in the GINA guidelines [7]. The fever duration was also significantly longer in atypical cases (6.8 ± 1.2 days vs. 4.2 ± 0.9 days, p < 0.05), suggesting a more protracted disease course.Radiological features.Radiographic imaging provided further differentiation between groups. Focal–interstitial infiltrates predominated in Group I (59.3%), whereas segmental and lobar infiltrates were characteristic of Group II (63.4%, p < 0.05). This pattern is consistent with earlier reports that atypical pneumonia causes diffuse interstitial involvement, often misdiagnosed as viral infection [2,11]. In post-COVID-19 studies, radiological variability of MPP has become even more pronounced, with atypical patterns mimicking viral pneumonia [11].Laboratory findings.The inflammatory response in M. pneumoniae pneumonia was milder compared with typical bacterial pneumonia. ESR and CRP were elevated but significantly lower in Group I (ESR 19.4 ± 2.3 vs. 28.6 ± 3.1 mm/h; CRP 9.8 ± 1.4 vs. 18.6 ± 2.2 mg/L; p < 0.05). Leukocytosis was observed in 11.2 ± 1.5 ×10⁹/L in Group II compared with 7.8 ± 1.3 ×10⁹/L in Group I (p < 0.05). These differences confirm that routine inflammatory markers are not always reliable for diagnosing atypical pneumonia [4]. This diagnostic challenge has been highlighted in large cohort studies, which emphasize the need for alternative biomarkers [12,13].Immunological profileChildren with atypical pneumonia demonstrated pronounced immune dysregulation. CD3+ lymphocytes were reduced (58.2% vs. 66.7% in controls, p < 0.05), CD4+ levels decreased (28.6% vs. 36.4%, p < 0.05), CD8+ levels increased (29.4% vs. 22.1%, p < 0.05), and the CD4+/CD8+ ratio was significantly lower (0.97 vs. 1.65 in controls, p < 0.05). Such imbalance suggests T-cell exhaustion and skewing toward cytotoxic responses.Elevated IgM (2.4 ± 0.3 g/L vs. 1.6 ± 0.2 g/L, p < 0.05) and IgE (143.6 ± 14.2 IU/mL vs. 75.4 ± 9.1 IU/mL, p < 0.05) reflected hyperactivation of humoral and allergic pathways. This may explain the high frequency of bronchial obstruction in our cohort, as IgE-mediated hypersensitivity plays a role in airway inflammation.Cytokine analysis revealed hyperproduction of IL-6 (27.8 vs. 11.6 pg/mL) and TNF-α (35.4 vs. 14.3 pg/mL), coupled with decreased IFN-γ (7.9 vs. 15.6 pg/mL, p < 0.05). These results are in agreement with earlier findings that M. pneumoniae induces a proinflammatory cytokine storm while impairing antiviral defense [5,8]. Moreover, recent evidence suggests that IL-17 is also elevated in severe cases of MPP, further supporting the concept of Th17-driven inflammation [12].Microcirculatory disturbances.Capillaroscopy and Doppler flowmetry revealed profound microvascular abnormalities in Group I: dilated and tortuous capillaries, stasis zones, reduced microcirculation index (7.8 vs. 12.6 in controls, p < 0.05), prolonged circulation time, and increased amplitude of slow oscillations. In contrast, Group II exhibited only mild, reversible changes. These findings suggest that vascular dysfunction is central to MPP pathogenesis.This aligns with observations by Duan et al. [13], who reported altered cytokine and vascular patterns in pediatric CAP of various etiologies. Our study adds to the evidence that endothelial dysfunction is not simply a secondary effect but a primary mechanism linking immune imbalance and clinical severity.Comparative analysis with literatureThe integration of our results with recent studies highlights several key points:Age dependence: MPP is more frequent in school-age children, consistent with both earlier epidemiology [3] and recent post-COVID reports [11].Immune dysregulation: Reduced CD4+/CD8+ ratio and cytokine imbalance (IL-6, TNF-α, IFN-γ, and IL-17) are consistent with global data [5,8,12].Vascular involvement: Our microcirculatory findings mirror current evidence that endothelial biomarkers correlate with disease severity [13].Taken together, these findings underscore that M. pneumoniae pneumonia should be considered a systemic disease rather than a purely respiratory infection.Clinical implications.The diagnostic challenge of MPP lies in its atypical clinical course and weak inflammatory response. Our findings suggest that incorporating immunological (T-cell subsets, cytokines) and vascular (flowmetry indices) markers could improve early recognition of severe cases. Such biomarkers could also guide adjunctive therapies, including antioxidants, endothelial stabilizers, and immunomodulators. This personalized approach aligns with precision medicine principles in pediatric infectious diseases [7,11–13].
|
|

|

|
4. Conclusions
- The present study demonstrated that atypical pneumonia of Mycoplasma pneumoniae etiology in children is characterized by distinct clinical, immunological, and microcirculatory features compared with typical bacterial pneumonia. The disease was more frequent in school-aged children and manifested with gradual onset, subfebrile fever, prolonged cough, and a tendency toward bronchial obstruction, whereas typical bacterial pneumonia was marked by acute onset and stronger inflammatory markers.Laboratory findings confirmed lower leukocytosis and CRP in M. pneumoniae pneumonia, but profound immune dysregulation was observed, including decreased CD3+ and CD4+, increased CD8+, altered CD4+/CD8+ ratio, and a cytokine profile dominated by IL-6 and TNF-α hyperproduction with reduced IFN-γ. Microcirculatory assessment revealed endothelial dysfunction, capillary stasis, and reduced microcirculation index, indicating systemic vascular involvement beyond local pulmonary inflammation.Clinically, these findings emphasize that reliance solely on classical inflammatory markers may delay diagnosis. Incorporating immune (lymphocyte subsets, cytokine profiling) and vascular (capillaroscopy, Doppler flowmetry) parameters into diagnostic protocols could improve early recognition and prognostic evaluation. Therapeutically, the observed immune and endothelial dysfunctions highlight the need for adjunctive treatments — including immunomodulators, antioxidants, and endothelial protectors — in addition to antibiotics, particularly for high-risk children with asthma, allergy, or immunodeficiency.Thus, M. pneumoniae pneumonia should be considered a systemic disease requiring a differentiated approach to diagnosis, treatment, and prevention. The integration of immune and vascular assessments into clinical practice may contribute to more accurate diagnosis, personalized therapy, and improved outcomes in pediatric patients.