-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3143-3145
doi:10.5923/j.ajmms.20251509.66
Received: Sep. 5, 2025; Accepted: Sep. 27, 2025; Published: Sep. 29, 2025

Features of the Development of Chronic Kidney Disease in Patients with Contrast-Induced Nephropathy
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMustafayeva M. R., Akhmedova N. Sh.
Bukhara State Medical Institute named after Abu Ali ibn Sina, Bukhara, Uzbekistan
Correspondence to: Mustafayeva M. R., Bukhara State Medical Institute named after Abu Ali ibn Sina, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The rapid development of contrast instrumental diagnostic methods leads to the widespread occurrence of renal dysfunction. In 112 patients included in the study, who underwent contrast angiography, although acute kidney damage was not observed, after 6 months in 22.1%, after 12 months in 37.2%, and after 24 months in 43.1% of patients, chronic kidney disease of degrees 3a and 3b developed. This indicates that intravenous contrast agents are a high risk factor for the development of nephropathy.
Keywords: KIN, Nephrinuria, CKD, ESUR, ARD, Including mortality
Cite this paper: Mustafayeva M. R., Akhmedova N. Sh., Features of the Development of Chronic Kidney Disease in Patients with Contrast-Induced Nephropathy, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3143-3145. doi: 10.5923/j.ajmms.20251509.66.
Article Outline
1. Introduction
- Examinations with contrast agents (computer tomography and invasive angiographic procedures) have become an integral part of fast and accurate diagnosis in modern medicine. At the same time, acute renal damage (ARD) occurring after contrast implantation and its long-term consequences - the risk of transition to chronic kidney disease (CKD) - is a pressing issue for practice. The updated manual of the European Society of Urogenital Radiology (ESUR) recommends the use of the term "post-contrast acute kidney injury" (post-contrast acute kidney injury), since the resulting disorder is not always explained by the direct causal effect of contrast. This approach requires caution and evidence-based decision-making in clinical assessment (ESUR Guidelines on Contrast Agents, 2018). According to the 2024 manual of the American College of Radiology and its updated web publication for the public, in patients with creatinine-based renal glomerular filtration rate (RGFR) ≥30 ml/min/1.73 m2, the independent risk of OBS due to intravenous contrast application is very low, the risk is mainly relevant in the category with RGFR <30 or existing OBS. Therefore, the correct organization of screening around GFR, the application of preventive measures to high-risk patients, and the rational planning of contrast volume minimize clinical risk [2].Nevertheless, clinical experience and numerous studies confirm that in patients with episodes of OBSH in the long term, new or progressive CKD is associated with the transition to renal failure and an increase in complications (including mortality) in general [1]. A large meta-analysis in 2019 showed that the risk of new/progressive CKD was 2.7 times higher, the risk of terminal renal failure was 4.8 times higher, and the risk of death was 1.9 times higher in patients who had CKD. The updated system review for 2025 also once again noted an increased risk of adverse renal outcomes after OBSH. Consequently, even short-term functional impairment can worsen kidney function in the following months and years [5].Another reason for the urgency of this issue is the problem of early detection. For timely awareness of the risk of progressing to CKD, the level of creatinine in the classical urogenital tract changes late; therefore, it is believed that markers such as cystatin C, neutrophil gelatinase-associated lipocalin (NGAL), kidney damage molecule-1 (KIM-1), and interleukin-18 can provide early information [3]. Although recent scientific reviews confirm the early predictive value of cystatin C and NGAL, the issues of standardization of value limits and their full implementation in the clinical algorithm remain open [4].Purpose of the study assessment of the risk of CKD development after contrast-induced nephropathy (CIN) based on clinical and laboratory factors.
2. Materials and Methods of Research
- The study involved 112 patients who underwent a directed contrast examination for CABG surgery: 62 men (55.4%), 60 women (44.6%). To assess kidney function, the following laboratory parameters were used: GFR - calculated by cystatin C. The amount of daily microalbumin (MAU) in the urine and nephrinuria - the amount of nephrin in the urine (a marker of damage to the renal glomerular barrier) were determined. The analyses were determined before surgery, after surgery (up to 3 days), at 3, 6, 12, 18, and 24 months.The analyses were conducted in the scientific laboratory of the Bukhara State Medical Institute.Statistical analysis was carried out in the Microsoft Excel program based on Student's and Pearson's criteria. The principle of evidence-based medicine was used in the organization and conduct of the study.
3. Analysis of the Results
- Before contrast studies, GFR was determined based on the cystatin C indicator. The indicator averaged 88.2±14 ml/min/1.73m2. In 8.9% of patients, grade 3b CKD was detected, and the GFR averaged 36.9 ml/min/1.73m2 (max 39.2; min 30.2). Since patients with GFR ≤30 ml/min/1.73m2 were not identified, it was concluded that there were no patients in the high-risk group for KIN. CKD levels were determined depending on GFR indicators. In this case, stage 1 CKD was detected in 28.6±2.8% of patients, stage 2 CKD in 33.9±2.7%, stage 3a CKD in 28.6±2.8%, and stage 3b CKD in 8.9±1.7% of patients.In all patients after surgery (up to 3 days), GFR was assessed and observed in dynamics at 3, 6, 12, 18, and 24 months (Fig. 1).
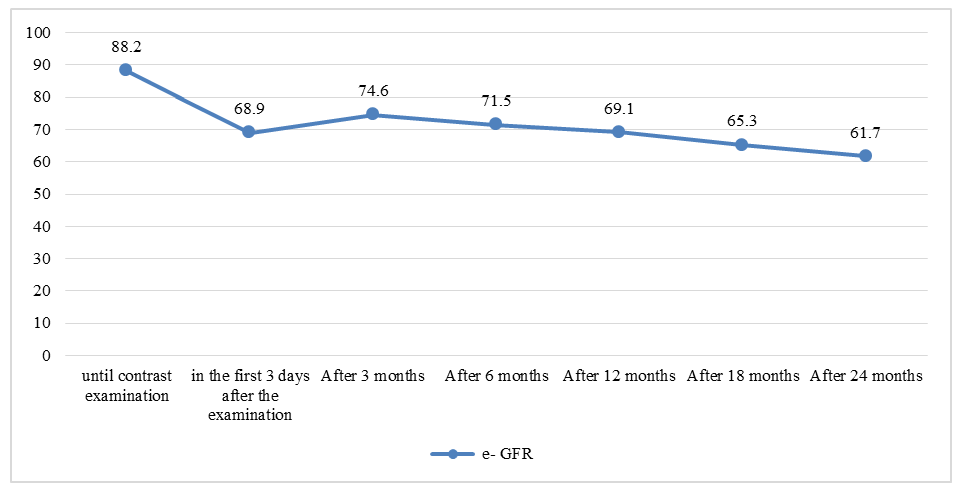 | Figure 1. Dynamics of GFR indicators in the periods after contrast examination (%) |
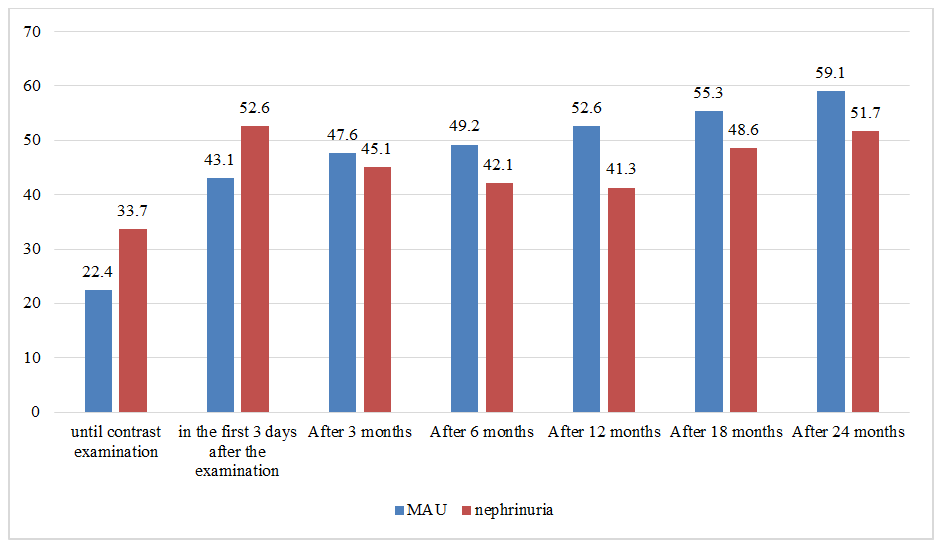 | Figure 2. Dynamics of MAU and nephrinuria within 24 months after contrast examination (%) |
4. Conclusions
- Patients who have undergone KIN have a high risk of developing CKD within 24 months, which can be detected early using biomarkers. Cystatin C, MAU, and nephrinuria are biomarkers with high sensitivity in assessing the development of CKD. Based on these parameters, early detection of CKD and initiation of pathogenetic treatment can slow down the progression of CKD.