-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3131-3134
doi:10.5923/j.ajmms.20251509.63
Received: Sep. 6, 2025; Accepted: Sep. 26, 2025; Published: Sep. 29, 2025

Analysis of the Causes of Unsatisfactory Results of Traditional Methods for Diagnosing and Treating Various Forms of Necrotizing Fasciitis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLOkhunov А. О.1, Korikhonov D. N.2
1Professor, Doctor of Medical Sciences, Head of the Department of General and Pediatric Surgery-1, Tashkent Medical Academy, Tashkent, Uzbekistan
2Assistant of the Department of General and Pediatric Surgery-1, Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Okhunov А. О., Professor, Doctor of Medical Sciences, Head of the Department of General and Pediatric Surgery-1, Tashkent Medical Academy, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Relevance of the study is determined by the persistently high mortality rate in necrotizing fasciitis, which is associated with difficulties in early diagnosis, the polymicrobial nature of the infectious process, and the untimely initiation of radical treatment. The aim of the study is to analyze the causes of unsatisfactory results of traditional methods for diagnosing and treating various forms of necrotizing fasciitis and to identify the characteristics of the microbial factors influencing the course of the disease. The study included 120 patients with different forms of necrotizing fasciitis who were treated at the multidisciplinary clinic of the Tashkent Medical Academy between 2016 and 2024. Clinical, laboratory, instrumental, and microbiological methods were used to assess the patients' conditions. It was shown that the main reasons for unsatisfactory outcomes were late hospitalization (≥4 days from the onset of the disease), a high rate of incorrect preliminary diagnoses (55.9%), and insufficient sensitivity of standard imaging methods. Microbiological analysis revealed a predominance of mixed associations of facultative anaerobes with a high degree of wound contamination. The obtained data justify the need for a comprehensive diagnostic approach, including laboratory markers of inflammation, modern imaging techniques, and targeted antibacterial therapy considering the polymicrobial profile.
Keywords: Necrotizing fasciitis, Diagnosis, Microbial association, Surgical infection, Prognosis
Cite this paper: Okhunov А. О., Korikhonov D. N., Analysis of the Causes of Unsatisfactory Results of Traditional Methods for Diagnosing and Treating Various Forms of Necrotizing Fasciitis, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3131-3134. doi: 10.5923/j.ajmms.20251509.63.
1. Introduction
- Necrotizing fasciitis remains one of the most challenging problems in purulent surgery, characterized by a severe course, a high risk of septic complications, and extremely high mortality. Despite significant advances in the diagnosis and treatment of soft tissue infections, early verification of necrotizing lesions remains difficult, which leads to delayed adequate surgical interventions and worsens the disease prognosis [1].In modern practice, analyzing the causes of unsatisfactory results in the diagnosis and treatment of necrotizing fasciitis is relevant for optimizing therapeutic tactics and reducing the frequency of adverse outcomes.One of the key problems complicating the timely diagnosis of necrotizing fasciitis is the nonspecific nature of clinical manifestations in the early stages of the disease. The absence of clear visual symptoms of superficial tissue involvement, similarity to banal subcutaneous phlegmon, and insufficient informativeness of routine instrumental examination methods often lead to erroneous treatment strategies [2].Analyzing diagnostic errors and the structure of patient referrals with various forms of necrotizing fasciitis is a necessary step to identify critical points in existing diagnostic algorithms.The microbiological profile of necrotizing fasciitis pathogens also significantly contributes to the disease course and outcome. The formation of associative microbial complexes dominated by facultative anaerobes, gram-positive cocci, and gram-negative rods complicates the effective empirical antibacterial therapy, especially in the presence of hospital strains with broad resistance to standard antibiotic regimens [3].Studying the microbial characteristics of the wound process and its dynamics in the postoperative period allows for a deeper understanding of the mechanisms of necrotizing fasciitis progression and provides a rationale for adjusting therapeutic approaches.Results of previous studies indicate the necessity of an integrative approach to the assessment of patients suspected of having necrotizing fasciitis, including a combination of clinical vigilance, comprehensive laboratory tests, imaging methods, and mandatory early microbiological verification [4]. However, the practical application of such algorithms in multidisciplinary hospitals at various stages of the disease still requires detailed evaluation and adaptation.Thus, analyzing the causes of unsatisfactory results of traditional diagnostic and treatment methods for various forms of necrotizing fasciitis, as well as studying the features of microbial wound contamination, is an important task of modern surgical practice aimed at increasing the effectiveness of treatment, reducing complication rates, and improving prognosis in patients with this pathology.The aim of this study is to analyze the causes of unsatisfactory results of traditional methods for diagnosing and treating various forms of necrotizing fasciitis and to identify the characteristics of microbial factors influencing the course and outcome of the disease.
2. Materials and Methods
- This study was conducted at the Center for Purulent Surgery and Surgical Complications of Diabetes Mellitus at the multidisciplinary clinic of the Tashkent Medical Academy. A retrospective analysis included the examination and treatment results of 120 patients with various forms of necrotizing fasciitis who were hospitalized between 2016 and 2024. Patients were divided into two groups: the control group consisted of 62 patients who received treatment based on the traditional diagnostic and therapeutic methods for necrotizing fasciitis accepted at that time; the main group included 58 patients who underwent advanced methods for predicting disease progression and a fundamentally different approach to local wound treatment using ozone sanitation and vacuum therapy technologies. Inclusion criteria were age over 18 years and the presence of either complicated or uncomplicated forms of necrotizing fasciitis. The diagnostic algorithm included clinical, laboratory, microbiological, and instrumental methods of investigation. Standard general clinical examinations were performed (complete blood count, urinalysis, biochemical tests), coagulation profile, as well as assessment of inflammatory markers including C-reactive protein, lactate, D-dimer, and creatine phosphokinase activity. Instrumental diagnostics were performed using ultrasound, radiography, multi-slice computed tomography, and magnetic resonance imaging as indicated [5].Bacteriological analysis included bacterioscopy of wound discharge with Gram staining, as well as quantitative and qualitative cultures of exudate for aerobic and anaerobic flora. Identification of pathogens was conducted based on morphological and cultural characteristics, with mandatory determination of antibiotic sensitivity.Statistical data processing was carried out using Numbers and BioStat software, version 14.3. For quantitative indicators, the arithmetic mean (M), standard deviation (σ), and standard error of the mean (m) were calculated. Group comparisons were performed using the parametric Student’s t-test, provided data normality and homogeneity of variances were confirmed. Differences were considered significant at a p-value < 0.05.
3. Results
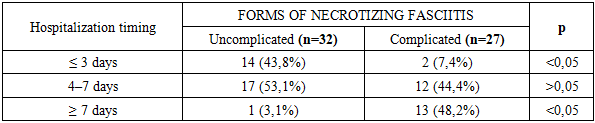
- The analysis of hospitalization timing showed that only 16 patients (25.8%) sought medical care within the first 72 hours from disease onset. The majority of patients (74.2%) were hospitalized at later stages of the pathological process. Among patients with complicated forms of necrotizing fasciitis, late hospitalization (≥4 days) was observed in 89.5% of cases, which was significantly higher than the corresponding rate in patients with uncomplicated forms of necrotizing fasciitis (p < 0.05) — see Table 1.
|
|
4. Discussion
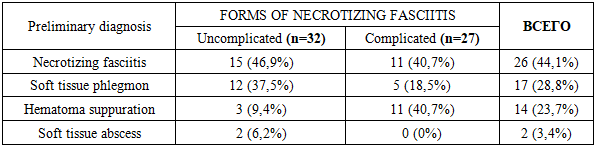
- The results obtained in this study confirm that delayed hospitalization of patients with necrotizing fasciitis is one of the leading factors contributing to the development of complicated forms of the disease. The predominance of late presentations (more than 72 hours from the onset of symptoms) significantly correlated with a worse prognosis and an increased frequency of septic complications, which is consistent with literature data highlighting the critical importance of early diagnosis and immediate initiation of surgical treatment [2].Analysis of the preliminary diagnoses revealed a high frequency of misinterpretation of the clinical presentation of necrotizing fasciitis as soft tissue phlegmon or hematoma suppuration. This finding emphasizes that traditional clinical and instrumental approaches, based on assessing external manifestations of inflammation and standard imaging techniques, are insufficient for early diagnosis verification. Comparable results were obtained in several studies where the rate of correct preoperative diagnosis of necrotizing fasciitis did not exceed 40-50% [1].The clinical-laboratory profile of patients with necrotizing fasciitis was characterized by a pronounced inflammatory response, hyponatremia, and signs of microcirculation disturbances, reflected in increased levels of D-dimer and lactate. These changes were particularly pronounced in patients with complicated forms of the disease. These findings support the hypothesis of the central role of the systemic inflammatory response and developing coagulopathy in the pathogenesis of severe forms of necrotizing fasciitis, as previously reported by M.R. Schmid et al. [6].The microbiological characteristics of the wound process are of particular importance. The presence of mixed microbial associations with a predominance of facultative anaerobes, as well as the frequent addition of hospital flora during the course of traditional treatment, led to a severe wound process, an increased number of repeat surgical interventions, and prolonged healing. Similar data on the polymicrobial nature of necrotizing fasciitis and its impact on prognosis were presented in the works of T. Goh et al. [4].The low sensitivity of traditional imaging methods (ultrasound, radiography) in detecting deep tissue changes, especially in the context of a concealed infection, also calls for a reassessment of diagnostic algorithms. According to our data, only the use of multi-slice computed tomography (CT) and magnetic resonance imaging (MRI) allowed for the reliable verification of signs of fascia damage and muscle destruction, which is consistent with the findings of M.G. Wysoki et al. [5].Thus, to improve the effectiveness of diagnosis and treatment of necrotizing fasciitis, an integrative approach is needed, including early clinical suspicion when a combination of nonspecific signs (pain, swelling, erythema) is present, mandatory evaluation of laboratory markers of inflammation and coagulation, extensive use of modern imaging techniques, and aggressive surgical tactics based on the principles of early sanitation of the infection focus and targeted antibacterial therapy considering the microbiological profile.
5. Conclusions
- The conducted study showed that the unsatisfactory results of traditional methods of diagnosis and treatment of various forms of necrotizing fasciitis are due to a combination of delayed hospitalization, insufficient clinical suspicion, low sensitivity of standard instrumental methods, and the complex polymicrobial nature of the infectious process. The identified features of clinical progression, laboratory, and microbiological changes emphasize the need for early integrative diagnosis based on a combination of clinical signs, laboratory markers of inflammation, and modern imaging technologies, as well as timely radical surgical intervention combined with targeted antibacterial therapy.Informed Consent - The study was conducted in accordance with the Declaration of Helsinki of the World Medical Association (2013) and approved by the local ethics committee of the Tashkent Medical Academy. All patients provided informed voluntary consent to participate in the study.Funding - The study was not funded. The authors conducted the work as part of their primary research activities.The authors declare that there is no conflict of interest. Author Contributions - All authors made equal contributions to the development of the research concept, data collection, analysis and interpretation, manuscript preparation, and approval of the final version for publication.