-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3124-3127
doi:10.5923/j.ajmms.20251509.61
Received: Aug. 28, 2025; Accepted: Sep. 26, 2025; Published: Sep. 29, 2025

Possibilities of Minimally Invasive Technologies in Early Postoperative Complications of the Biliary Tract
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIsmailov Uktam Safayevich1, Abdurakhmanov Shodiyor Shavkatovich2, Madatov Kurbonboy Aminboyevich3, Matmuratov Seyilkhon Kuronboyevich4
1Professor, Head of the Department of Surgical Diseases No. 1 at Tashkent State Medical University, International Faculty, Tashkent, Uzbekistan
2Doctoral Candidate, Department of Surgical Diseases No. 1 of Tashkent State Medical University, International Faculty, Tashkent, Uzbekistan
3PhD, Senior Lecturer, Department of Surgical Diseases No. 1 of the International Faculty, Tashkent State Medical University, Tashkent, Uzbekistan
4Candidate of Medical Sciences, Senior Lecturer, Department of Surgical Diseases No. 1 of the International Faculty, Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article presents the results of diagnosing and treating early postoperative bile duct complications in 92 patients. Following minimally invasive surgical interventions, the number of postoperative complications decreased from 16 (33.3%) to 3 (6.8%), and the average length of hospital stay reduced from 15.8±2.32 days to 8.41±0.32 days. Additionally, postoperative mortality declined from 12.5% to 2.3%. These findings demonstrate the effectiveness of the performed minimally invasive surgical interventions.
Keywords: Biliary fistula, Peritonitis, Duct surgeries, Abdominal complications
Cite this paper: Ismailov Uktam Safayevich, Abdurakhmanov Shodiyor Shavkatovich, Madatov Kurbonboy Aminboyevich, Matmuratov Seyilkhon Kuronboyevich, Possibilities of Minimally Invasive Technologies in Early Postoperative Complications of the Biliary Tract, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3124-3127. doi: 10.5923/j.ajmms.20251509.61.
1. Introduction
- The achievements in abdominal surgery over the past decade have not diminished the relevance of issues related to the tactics and strategies for treating patients with early postoperative abdominal complications. This is due to the challenges of timely diagnosis and adequate treatment of abdominal complications in the early postoperative period, their high incidence rate, and mortality that shows no tendency to decrease [1,3,5,8].Despite all the advancements in modern surgery, operations associated with postoperative abdominal complications are performed late, and sometimes unnecessarily, in a significant number of patients. This is largely because objective criteria that emerge in the early postoperative period often make it difficult to recognize the clinical picture of complications against the background of intensive treatment in intensive care and anesthesiology units, especially after extensive open surgeries [2,4].Although patients and surgeons often express negative attitudes towards repeated interventions, the role of subjective aspects in the postoperative period is of considerable importance [6,7,8].Despite significant positive experiences from initial research in this field, many unresolved issues remain. For instance, optimal criteria for diagnosing and selecting treatment methods for early postoperative complications have not been developed, and the immediate and long-term consequences of using minimally invasive technologies have not been fully addressed. Moreover, there is currently a viewpoint questioning the applicability of these methods in clinical practice and the feasibility of using expensive technologies. All these factors underscore the relevance of the issue under study and the necessity of our scientific research.Purpose of the study: To improve treatment outcomes for early postoperative biliary tract complications through the rational use of minimally invasive diagnostic and treatment methods.
2. Materials and Methods
- The study is based on an analysis of examination and treatment results for 92 patients with early postoperative biliary complications following various bile duct surgeries. These patients were treated at the multidisciplinary clinic of the Center for Professional Development of Medical Workers in Tashkent.To address research objectives aimed at developing new treatment and diagnostic tactics, considering modern trends in emergency surgery, patients were divided into two groups. Group I (control group - patients from 2010 to 2016) included 48 (52.2%) patients with various complications from biliary tract surgeries, who received standard, generally accepted treatment approaches. Group II (main group - patients admitted after 2016) included 44 (47.8%) patients, for whom the therapeutic and diagnostic algorithm was based on enhanced recovery program (ERP) principles, with minimally invasive surgical interventions used as the primary surgical treatment methods.In the main group, women comprised 28 (63.6%) and men 16 (36.4%), while in the control group these figures were 31 (64.6%) and 17 (35.4%) respectively (χ2=0.0089; p=0.92). The ratio of women to men was 2:1, which corresponds to the average statistical data on the incidence of cholelithiasis. The age of patients ranged from 21 to 81 years, with a mean age of 51.2±13.8 years in the main group and 49.7±9.72 years in the control group (t=0.09; df=90; p=0.93). The compared groups were representative in terms of gender and age (p>0.05). Statistical analysis of the obtained results was conducted using the STATISTICA 13 software package.
3. Results and Discussion
- Forty-eight patients with postoperative biliary peritonitis underwent emergency surgery. These patients constituted the control group. Clinical, laboratory, and instrumental signs of postoperative biliary peritonitis (n=38), hemoperitoneum (n=8), and combined biliary peritonitis and hemoperitoneum (n=2) served as indications for emergency surgery. In this group, postoperative biliary peritonitis developed in 11 patients due to cystic duct stump failure, in 4 patients due to biliodigestive anastomosis failure, in 6 patients due to aberrant bile ducts in the gallbladder bed, and in 17 patients after common bile duct injuries (n=7) and various drainage procedures (Kehr drainage - 7, Pikovsky drainage - 3). In 2 patients, both bleeding and biliary peritonitis were caused by biliodigestive anastomosis failure.In 8 patients, the causes of bleeding from the biliary tract were hemorrhages from the cystic artery (n=6) and the abdominal wall (2) (Figure 1).
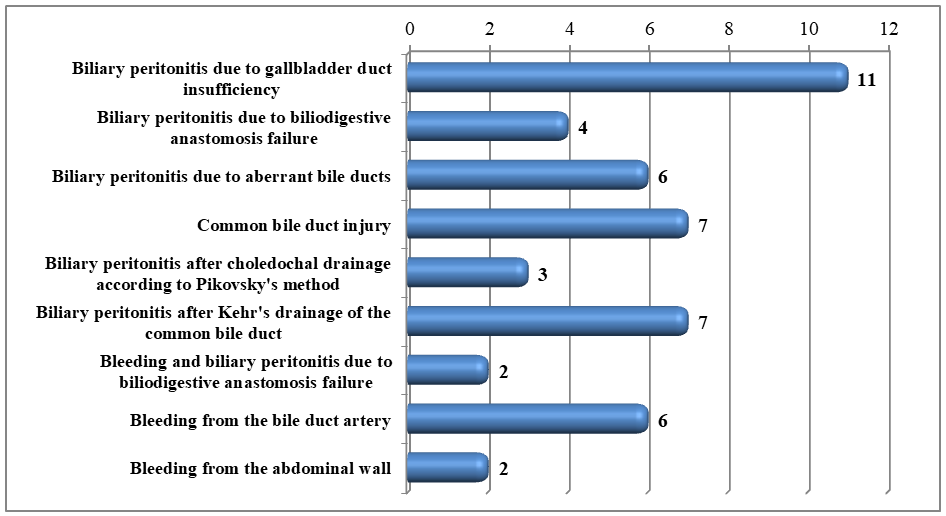 | Figure 1. Conditions causing biliary complications |
|
|
4. Conclusions
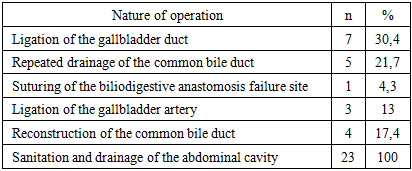
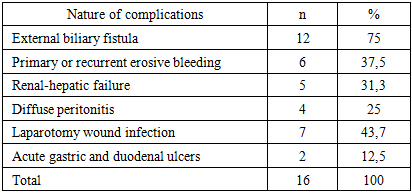
- Thus, biliary complications after bile duct surgeries occurred due to cystic duct stump insufficiency, biliodigestive anastomosis failure, presence of aberrant bile ducts in the gallbladder bed, and after various types of extrahepatic duct drainage (according to Kehr, Pikovsky, Vishnevsky) due to common bile duct injuries and Mirizzi syndrome. Bleeding and biliary peritonitis were caused by biliodigestive anastomosis failure, and isolated bleeding from the cystic artery and abdominal wall was also observed. In the control group of 48 patients, active surgical tactics were employed in 43 cases, and active-expectant tactics in 5. This group underwent relaparotomy, cystic duct suturing, repeated common bile duct drainage, suturing of failed biliodigestive anastomosis, cystic artery ligation, reconstructive operations on the common bile duct, and abdominal cavity lavage and drainage. In the main group, minimally invasive methods were used in all cases: relaparoscopy for cystic duct stump failure with repeated clipping, relaparoscopic suturing of common bile duct injuries with Kehr and Vishnevsky drainage, relaparoscopic lavage of the gallbladder bed with coagulation of bile leakage source in aberrant ducts, relaparoscopic repeated drainage of the common bile duct in biliary peritonitis after drainage for Mirizzi syndrome, relaparoscopic lavage and drainage of the abdominal cavity (subhepatic space and pelvis) in limited biliary peritonitis, relaparoscopic hemostasis for bleeding from the gallbladder bed, and percutaneous drainage for limited bile leakage from biliodigestive anastomosis. ERCP with EST was performed in 5 patients after bile leakage through drains ceased.After minimally invasive surgical interventions, postoperative complications decreased from 16 (33.3%) to 3 (6.8%) (χ2=9.85; p=0.002), and the length of hospital stay decreased from 15.8±2.32 to 8.41±0.32 days (t=3.16; df= 49; p=0.003). Postoperative mortality decreased from 12.5% to 2.3% (10%) (χ2=3.4; p=0.032). This indicates the feasibility of using the performed minimally invasive surgical interventions.