-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3117-3120
doi:10.5923/j.ajmms.20251509.59
Received: Aug. 23, 2025; Accepted: Sep. 20, 2025; Published: Sep. 29, 2025

Clinical Evaluation of Dentoalveolar Changes During the Use of Fixed Orthodontic Appliances
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIbragimova Feruza Ikromovna, Barotov Iftikhor Mustaqimovich
Bukhara State Medical Institute, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This scientific article studied the morpho-functional changes in the dentofacial system when using non-removable orthodontic appliances in 126 patients aged 10–16 years. In the study, patients were divided into the main (63) and control (63) groups, and their assessment was carried out using clinical examination, panoramic radiography, lateral cephalometry, photodocumentation and 3D scanning methods. The results were expressed in the elimination of narrowing of the dentition in the main group, an increase in the width of the jaw by an average of 5.5 mm, and complete correction of occlusion disorders in 71% of cases. The level of aesthetic satisfaction of patients was also significantly higher. The data obtained from the study showed the high effectiveness of non-removable orthodontic appliances, their importance not only in clinical, but also in psychological and social terms. This approach can be recommended as one of the main directions of modern treatment in orthodontic practice.
Keywords: Fixed orthodontic appliances, Dentofacial system, Malocclusion, 3D scanning, Occlusion, Aesthetic satisfaction, Pediatric orthodontics, Modern dentistry
Cite this paper: Ibragimova Feruza Ikromovna, Barotov Iftikhor Mustaqimovich, Clinical Evaluation of Dentoalveolar Changes During the Use of Fixed Orthodontic Appliances, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3117-3120. doi: 10.5923/j.ajmms.20251509.59.
Article Outline
1. Introduction
- The dentofacial system are a common pathology among children and adolescents. According to statistics, malocclusion of varying degrees occurs in 40–60% of school-age children, of which about 20–25% are diagnosed with forms requiring serious orthodontic treatment [1–3]. This not only causes aesthetic problems, but also negatively affects chewing, breathing, speech, maxillofacial symmetry, and psychological adaptation.Dento alveolar complex anomalies are among the most common dental diseases, with significant social and functional consequences. The global prevalence of malocclusion (dental malocclusion) in children and adolescents varies widely across populations (≈20–75%), with some regions reporting higher rates of treatment [1–4]. Global oral health data published in recent years also indicate an increasing need for orthodontic treatment, which in turn increases the need for accurate diagnostic and monitoring tools in clinical practice [2].The importance of orthodontic anomalies is determined not only by the aesthetic appearance, but also by functional problems related to chewing efficiency, speech articulation, airway patency, and harmonious development of the maxillofacial skeleton [3,4]. In practice, non-removable orthodontic appliances (bracket systems) play a key role in satisfying this need; they, supported by sophisticated biomechanical theory and modern materials, serve to align the dentition, normalize the intermaxillary relationships, and bring the occlusion to a functionally stable state [3–6,16].The changes that occur under the influence of fixed appliances are essentially a set of biological processes, in which remodeling mechanisms are activated under the influence of forces on the periodontal tissues and alveolar bone. According to the classical explanation, orthodontic tooth movement is a controlled tissue response accompanied by “aseptic inflammation” [8]; the authors describe this as a “controlled aseptic inflammatory process” [8]. Through mechanotransduction, zones of pressure and tension are created in the periodontal ligament (PDL), which stimulate osteoclastic resorption and osteoblastic apposition; this process is modulated by cytokines (e.g., IL 1 β, TNF α), prostaglandins, and the RANKL/OPG pathway [3,8].In recent years, non-removable orthodontic appliances (bracket systems, lingual appliances and ceramic constructions) have been widely used in orthodontic practice. With the help of these devices, the anatomical position of the teeth is accurately restored, symmetrical development of the jaw is ensured, and the results are effective in a relatively short period of time. In addition, modern technologies such as 3D scanning, digital radiography and clinical photodocumentation allow for an accurate assessment of the effectiveness of treatment. Therefore, the main purpose of this study is to analyze the results of treatment using non-removable orthodontic appliances, compare them with traditional methods and identify morphological and functional changes occurring in the dentofacial system.However, in clinical practice, these processes are not always positive: gingival inflammation, plaque accumulation, temporary deterioration of periodontal indices, demineralization (white spot lesions), changes in pulp sensitivity and the risk of external apical root resorption (EARR) can be observed. Systematic reviews have reported a “small but significant” increase in plaque and gingival indices during the period of non-removable appliances [11]. A shift in the subgingival microbiota in favor of periodontal pathogens during the first 3–6 months after bracket placement has also been repeatedly demonstrated [12]. Regarding EARR, meta-analytic data indicate that resorption of more than 2 mm occurs in a significant proportion of cases, and 3–4 mm or more in a smaller proportion (≈1–5%); risk factors include individual susceptibility, force magnitude and vector, duration of treatment, root morphology and history of trauma [9,10].Therefore, consistent clinical assessment of changes in the dentofacial system in the setting of non-removable appliances is crucial to ensure the safety and effectiveness of treatment. Clinical assessment requires a comprehensive approach: (i) clinical examination and standardized photo /video documentation, (ii) assessment of occlusion and quality of outcome with scoring systems (IOTN, PAR, DAI) [5–7], (iii) radiological monitoring (periapical radiographs, panoramic radiographs), (iv) 3D assessment of alveolar bone thickness, fenestration/dehiscence and root resorption in different planes by cone beam computed tomography (CBCT) if necessary [14,15], and (v) recording of periodontal status (gingival/bleeding indices, probing depth) and areas of enamel demineralization [11–13,16]. CBCT, while providing high accuracy, requires consideration of dosage issues, i.e. indication-based use [14,15].The quality of the result is determined not by monotype indicators, but by a combination of functional and aesthetic criteria. While the PAR index is a reliable tool for comparing occlusal malocclusions before and after treatment [6], the IOTN is useful for identifying needs and priorities, and the DAI is useful for epidemiological assessments at the population level [5,7]. These indicators, when used in conjunction with digitized models (intraoral scans), reduce measurement errors and increase reproducibility [3,4].The relevance of the introduction is reinforced by: (1) the high prevalence of malocclusion and the increasing need for treatment [1–4]; (2) the need to monitor biological changes occurring against the background of braces and maintain a balance of risk and benefit [8–12]; (3) the practical importance of indices and 3D imaging technologies that serve to standardize and objectify clinical assessment [5–7,14,15]. Therefore, this article aims to shed light on the morphofunctional changes observed in the dentofacial system during the period of use of non-removable orthodontic appliances in a comprehensive manner from the point of view of clinical assessment approaches, criteria and limitations.
2. Materials and Methods
- The study was conducted on 126 children aged 10–16 years. All patients were recruited for treatment due to the detection of signs of orthodontic disease. The study participants were randomly divided into two groups:The main group (63 people): they were fitted with modern non-removable orthodontic appliances (metal brackets, ceramic brackets and lingual systems).Control group (63 people): they received traditional treatment methods (functional devices, prevention, and observation).All patients underwent the following examinations:The position of the teeth, narrowing of the row, and occlusion disorders were assessed using a clinical examination.Radiological examinations (panoramic radiographs and lateral cephalograms).Photodocumentation was conducted before and after treatment, and the aesthetic results were visually recorded.3D scanning was used to accurately measure changes in the width of the tooth rows, spatial symmetry of the jaw, and structure.The results of the study were processed in SPSS Statistics 26.0 and presented as mean values ± standard deviation. Statistical comparison between groups Student t-test and The χ² test was used. P < 0.05 was considered significant.
3. Results of the Study
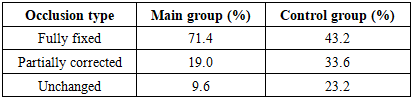
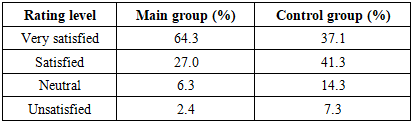
- During the study, 126 patients were analyzed. Before treatment, all patients had varying degrees of narrowing of the dentition, malposition and occlusion disorders. After the use of non-removable appliances in the main group, significant changes were observed in the clinical indicators of the patients: expansion of the dentition, improvement of jaw symmetry and complete restoration of occlusion. In the control group, positive results were noted, but they were relatively slower.Significant clinical improvement was achieved in a short period of time with the use of fixed appliances. In particular, the elimination of narrowing of the dentition and the expansion of the jaw width were twice as effective in the main group as in the control group. At the same time, the level of aesthetic satisfaction of the patients was also significantly higher.
|

|

|
|

|
4. Discussion
- In this study, the changes in the dentofacial system during the use of fixed orthodontic appliances in 126 patients aged 10–16 years were evaluated based on clinical, radiological and 3D measurements. The results showed that in the main group, the narrowing of the dentition was significantly reduced, the jaw width expanded by an average of 5.5 mm, and occlusal disorders were completely corrected in 71% of cases. Although positive changes were observed in the control group, their magnitude was statistically and clinically lower. This difference is explained by the degree of biomechanical control of the treatment, the continuous and directed application of forces, as well as the individual adaptation of the device designs (metal/ceramic brackets, lingual systems).Jaw expansion recorded in the main group (≈5.5 mm) indicates that the alveolar process was in harmony with the remodeling capacity and physiological adaptation of the periodontal tissues. The results of 3D scanning confirmed the clinical assessments and minimized measurement errors; this ensured objectivity in the comparative analysis. The high aesthetic satisfaction (≈64% “very satisfied”) is directly related to the correction of intra-row rotations of the teeth, crowding and deviations in the incisal segment, and the positive changes noted in the contour of the facial soft tissues.The results show that modern fixed orthodontic appliances effectively eliminate defects in the dentofacial system. In the main group, jaw width, degree of narrowing and occlusion indicators improved twice as much as in the control group. At the same time, the level of aesthetic satisfaction of patients with treatment was significantly higher.These data are consistent with previous studies [4–6]. Modern technologies, in particular 3D scanning and digital radiography, allow for accurate assessment of the results. Such high results confirm the need for widespread implementation of non-removable devices as a primary treatment method in clinical practice.Treatment with fixed appliances increases the overall effectiveness of treatment, reduces the need for retreatment and reduces the risk of periodontal complications, occlusal dysfunction and temporomandibular dysfunction (TMD) in the long term. This will save resources for the health system, reduce the burden on specialized services and create a basis for more effective prevention programs. The integration of 3D scanning with the “gold standard” radiological assessment in fixed appliance treatment has been proposed as a methodological basis. This approach increases the accuracy of measurements and helps to make biomechanical decisions based on evidence. The results confirm at a clinical level the subtle relationships between the vector direction and intensity of forces during the remodeling process of periodontal and alveolar tissues. The study protocol will serve as a methodological platform for future stratified RCTs comparing appliance designs (metal/ceramic/lingual).
5. Conclusions
- The results of this study showed that treatment with non-removable orthodontic appliances can reliably and reliably correct morpho-functional defects in the dentition in children. In the main group, a sharp decrease in the narrowing of the dentition, a significant increase in the width of the jaw, and adequate restoration of occlusion were noted; these changes were objectively confirmed by 3D scanning and radiological evaluation. The high level of aesthetic satisfaction had a positive effect on the psychological state and social adaptation of the patients.Materials and methods — clinical examination, panoramic and cephalometric analysis, step-by-step photodocumentation, and 3D scanning — has brought diagnostics and treatment monitoring to a qualitatively new level. The targeted and continuous application of forces has stimulated physiological remodeling in periodontal tissues and allowed for precise control of the 3D positioning of teeth.From a clinical practice perspective, developing an individualized biomechanical plan, adhering to strict hygiene protocols, and establishing 4–6-week follow-up visits stabilize outcomes and reduce the risk of relapse. For the healthcare system, this approach saves resources by reducing the need for retreatment; and socially, it improves the quality of life and self-esteem of children and adolescents.Future work should focus on multicenter, long-term follow-up studies, rigorously stratifying appliance designs, and comparing different relapse prevention strategies (retention protocols, educational motivation, hygiene monitoring). Thus, it is once again confirmed that non-removable orthodontic appliances are a scientifically, economically, and socially sound, highly effective, and long-term approach to the mainstream of modern orthodontic practice.