-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3110-3113
doi:10.5923/j.ajmms.20251509.57
Received: Sep. 2, 2025; Accepted: Sep. 27, 2025; Published: Sep. 29, 2025

Assessment of the Main Causes and Degrees of Speech Disorders in Children Aged 3 to 5 Using Various Scales and Tests
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKosimova Zarrina Aslonovna
Tashkent Medical Academy, Uzbekistan
Correspondence to: Kosimova Zarrina Aslonovna, Tashkent Medical Academy, Uzbekistan.
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article presents the results of an assessment of the main causes and degrees of speech disorders in children aged 3 to 5 using various scales and tests. A total of 80 children were included in the study, and their speech development was thoroughly analyzed based on the ELOLA, Wechsler, and Bezrukova-Kalenkova methods. The children were divided into groups according to mild, moderate, and severe speech disorders. The results revealed that severe speech impairments were often associated with neurological and auditory factors, as well as a lack of speech stimulation in the environment. Gender differences were also observed, with speech problems being more frequently recorded among boys. The study highlights the importance of a comprehensive approach to speech therapy diagnosis and rehabilitation.
Keywords: Speech disorder, Preschool age, Speech assessment, ELOLA test, Wechsler test, Bezrukova-Kalenkova method, Verbal IQ, Phonetic development, Cognitive development, Gender differences
Cite this paper: Kosimova Zarrina Aslonovna, Assessment of the Main Causes and Degrees of Speech Disorders in Children Aged 3 to 5 Using Various Scales and Tests, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3110-3113. doi: 10.5923/j.ajmms.20251509.57.
Article Outline
1. Introduction
- Speech disorders (SD) are common among children aged 3 to 5 years and represent a significant issue in the developmental trajectory of this age group. Identifying the causes and degrees of these disorders is crucial, as it greatly influences children’s future development. According to global epidemiological studies, approximately 10–15% of children suffer from speech development delays [1]. Such delays often lead to setbacks in physical and cognitive development, resulting in challenges with learning and social adaptation later in life. These issues not only contribute to delays in social and psychological development but also cause difficulties in family and preschool education environments [2].Early detection and proper treatment of speech disorders support children's social development and help them achieve successful outcomes in educational settings [3]. Early identification and analysis of speech disorders are therefore essential stages of child development. Delays or disruptions in speech development are influenced by a wide range of factors, including genetic predispositions, environmental exposures, family dynamics, and neurological conditions. In a study by Adams (2020), it was emphasized that delays in speech development are often linked to alterations in brain function, adverse environmental influences, and the child’s psychological state [4–5]. Adams also noted that social influences—such as a child’s role within the family and changes in the home’s linguistic environment—play a significant role [6]. These factors impact speech development, as children depend heavily on social environments to acquire language skills (Adams, 2020).Tests and scales play a critical role in detecting and analyzing speech development disorders. A study by Smith et al. (2019) emphasized the importance of analyzing social and genetic factors when diagnosing speech disorders [7]. Their findings indicated that developing accurate diagnostic and therapeutic methodologies for early detection of speech disorders can positively influence children's development. Their work demonstrated the effectiveness of timely interventions in addressing language and speech delays. Furthermore, Smith and colleagues highlighted the role of specialized exercises, psychological approaches, and educational strategies in supporting speech development and designing effective intervention methods [8].The effectiveness of various diagnostic methodologies and tests is especially important in the identification and treatment of speech disorders. According to Patel (2020), delays in speech development may stem from the child’s adaptation to the environment, the influence of the family setting, and the cultural context in which the child is raised. Patel suggested implementing broader approaches and methods in the speech training process to foster children’s social communication skills. These inclusive approaches, which consider social and cultural factors, can help detect speech delays and disorders, leading to the development of effective therapeutic interventions [9].Epidemiological studies on speech delays and disorders indicate that the rising incidence of these conditions is strongly tied to social and cultural factors. In a study by Tufan (2019), it was revealed that delays in speech development are not solely caused by neurological conditions but are also significantly influenced by social and cultural environments. Tufan emphasized the need to reassess educational settings and strengthen family interactions to enable earlier detection of speech development delays. As a result, this could lead to improvements in children’s speech development [10].In conclusion, studying speech disorders—especially identifying developmental delays and various degrees of impairment in children—is critical. Effective approaches and methodologies must be developed to address this issue, as the proper development of speech is essential for ensuring the child’s social and psychological well-being.Research Objective. The aim of this study is to identify the main causes and degrees of speech disorders in children aged 3 to 5 and to perform diagnostics using various scales and tests.
2. Materials and Methods
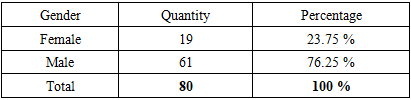
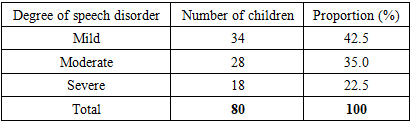
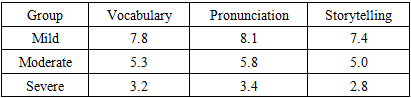
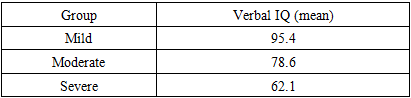
- This prospective observational study involved 80 children aged between 3 and 5 years. Among them, 19 (23.75%) were girls and 61 (76.25%) were boys. The study was conducted in local family polyclinics (CTMP), preschool institutions (kindergartens), and speech therapy centers. Oral and written informed consent was obtained from each child's parents.Initially, the children underwent a general pediatric examination, and their somatic and neurological status was assessed. Then, the level of speech development was determined using specialized tests, and each child's phonetic-phonemic, grammatical, and semantic abilities were evaluated separately.The following methods were used in the study:• Bezrukova-Kalenkova Method: a comprehensive assessment tool for evaluating phonemic hearing, grammar, vocabulary, and cognitive abilities;• Wechsler Test: adapted for children to determine verbal intelligence levels;• ELOLA Test: a logopedic analyzer aimed at assessing pronunciation, storytelling ability, and vocabulary development.Based on the assessment results, the children were divided into three main groups:1. Mild speech disorder (34 children);2. Moderate speech disorder (28 children);3. Severe speech disorder (18 children).Each group underwent individual testing. The assessment considered pronunciation, vocabulary, grammatical structure, storytelling ability, auditory differentiation, verbal and nonverbal intelligence, and cognitive development levels. The collected data were subjected to statistical analysis.
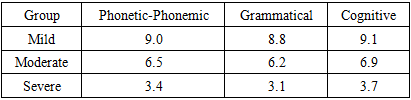
3. Results
- The study revealed that the forms and degrees of speech disorders in children aged 3–5 vary and are closely related to their intellectual and auditory functions, family environment, medical history, and psychological factors. In line with the study’s objective, the use of multiple assessment tools made it possible to identify each child’s individual issues and determine the severity of their condition.The following tables present data on the children’s gender distribution, levels of speech disorders, scores from various tests, and developmental indicators.
|
|
|
|
|
4. Discussion
- The analysis of the study results shows that the development of speech disorders in children aged 3 to 5 is influenced by multiple factors, including neurological, auditory, social-environmental, and pedagogical aspects. In particular, noticeable developmental delays in phonetic, grammatical, and cognitive domains were observed in children with a history of perinatal asphyxia and hearing impairments.The test results indicate that the ELOLA, Wechsler, and Bezrukova-Kalenkova methodologies are effective as complementary diagnostic tools. These assessments enable targeted evaluation of speech issues and support the development of individualized therapeutic approaches.In cases of mild speech disorders, children tend to adapt more quickly, and speech therapy yields faster results. However, moderate to severe cases require long-term psycho-pedagogical approaches, improvements in the family environment, and structured speech therapy rehabilitation.The study also highlighted the relevance of gender differences in speech disorders. It was found that speech disorders are more prevalent in boys than in girls, which may be attributed to differences in neurological development.Overall, early detection and accurate diagnosis of speech disorders, along with the development of individualized speech therapy programs, can significantly support healthy speech development in children.
5. Conclusions
- Based on the findings of this study, speech disorders in children aged 3 to 5 are associated with a variety of internal and external factors. The research employed a combination of methodological approaches—ELOLA, Wechsler, and Bezrukova-Kalenkova tests—to conduct a comprehensive assessment of each child’s speech and cognitive development.The results show that children with mild speech disorders are generally more likely to achieve positive progress quickly. In contrast, those with moderate to severe disorders require specialized speech rehabilitation and a multi-stage intervention approach. Factors such as hearing impairment, perinatal neurological damage, and a lack of linguistic stimulation in the family environment contribute significantly to the development of severe speech pathologies.The study also emphasized the importance of gender-based differences in speech disorders, noting a higher prevalence among boys. This highlights the need for preventive measures and early diagnostic strategies, particularly targeted at male children.
6. Recommendations
- 1. Implement mandatory speech development screenings for all children at the preschool (kindergarten) stage;2. Expand access to speech therapy services in outpatient clinics;3. Provide pedagogical consultations for parents on how to create a linguistically stimulating environment at home;4. Systematically apply comprehensive test batteries and assessment scales for diagnosing speech disorders.