-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3107-3109
doi:10.5923/j.ajmms.20251509.56
Received: Aug. 26, 2025; Accepted: Sep. 21, 2025; Published: Sep. 29, 2025

Clinical and Laboratory Features of Nephropathy in Type 2 Diabetes Mellitus
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLB. Kh. Shagazatova, Z. A. Rakhimberdieva
Department of Internal Diseases and Endocrinology, Tashkent Medical University, Tashkent, Uzbekistan
Correspondence to: B. Kh. Shagazatova, Department of Internal Diseases and Endocrinology, Tashkent Medical University, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Background: Diabetic kidney disease (DKD) is a major microvascular complication of type 2 diabetes mellitus (T2DM) and a leading cause of end-stage renal disease. According to KDIGO 2024 and ADA 2025 guidelines, even early chronic kidney disease (CKD) stages are associated with increased cardiovascular and renal risk, warranting proactive detection and intervention. Objective: To compare clinical, biochemical, and coagulation parameters between patients with T2DM and CKD stage 1 versus CKD stage 2. Methods: In this cross-sectional study (n = 30 per group), demographic, metabolic, renal function, lipid profile, and coagulation indices were compared. Independent t-tests, mean differences with 95% confidence intervals (CIs), p-values, and Cohen’s d effect sizes were calculated. Results: CKD stage 2 patients were older (mean diff. 9.94 years, 95% CI 8.98–10.90, p = 1.3 × 10⁻²⁷, d = 5.22) and had longer diabetes duration (mean diff. 2.29 years, 95% CI 2.00–2.58, p = 1.5 × 10⁻²¹, d = 3.96) compared to stage 1. They exhibited higher serum creatinine (mean diff. 16.20 μmol/L, p = 2.1 × 10⁻³³, d = 6.80), blood urea, and total cholesterol, alongside a modest but significant reduction in HbA1c. Coagulation changes in stage 2 included elevated fibrinogen, shortened activated partial thromboplastin time, and increased prothrombin index. Conclusions: Even at CKD stage 2, T2DM patients demonstrate substantial metabolic, lipid, and coagulation disturbances in addition to reduced renal function. These findings align with KDIGO 2024 and ADA 2025 recommendations for early, multidomain intervention to mitigate renal, cardiovascular, and thrombotic risks.
Keywords: Type 2 diabetes mellitus, Chronic kidney disease, Diabetic nephropathy, Dyslipidemia, Coagulation, Renal function
Cite this paper: B. Kh. Shagazatova, Z. A. Rakhimberdieva, Clinical and Laboratory Features of Nephropathy in Type 2 Diabetes Mellitus, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3107-3109. doi: 10.5923/j.ajmms.20251509.56.
1. Introduction
- Diabetic kidney disease (DKD) [1,2] is one of the most frequent and severe complications of type 2 diabetes mellitus (T2DM), affecting up to 40% of patients over the course of their disease and accounting for a major proportion of end-stage renal disease cases worldwide. According to the KDIGO 2024 [3] Clinical Practice Guideline for the Evaluation and Management of CKD, early CKD stages—defined by preserved estimated glomerular filtration rate (eGFR) but with other markers of kidney injury—are associated with increased risk for cardiovascular events, faster renal decline, and mortality, especially in patients with diabetes. Similarly, the ADA Standards of Care in Diabetes—2025 recommend systematic annual screening for eGFR and albuminuria in all adults with T2DM, beginning at diagnosis, with risk-factor modification initiated at the earliest evidence of CKD.The pathophysiology of DKD is multifactorial, involving chronic hyperglycemia [5], intraglomerular hypertension, oxidative stress, and systemic inflammation. Beyond glycemic derangements, patients often exhibit dyslipidemia [2,6], endothelial dysfunction, and abnormalities in coagulation and fibrinolysis—even in early CKD—which contribute to accelerated atherosclerosis [6] and thrombotic risk. These extra-renal alterations are increasingly recognized as important therapeutic targets alongside glucose and blood pressure control.This study aimed to perform a detailed comparative analysis of demographic, clinical, biochemical, and coagulation parameters in T2DM patients with CKD stage 1 and stage 2, contextualizing findings within the KDIGO 2024 [3] and ADA 2025 [4] frameworks to inform earlier and more targeted interventions.
2. Materials and Methods
- Study design and setting: This was a cross-sectional, comparative observational study conducted at the Department of Internal Diseases and Endocrinology, Tashkent Medical University, Tashkent, Uzbekistan, between November 2024 and March 2025, following STROBE guidelines.Study population: Sixty adult patients with T2DM were equally divided into two groups: CKD stage 1 (n = 30) and CKD stage 2 (n = 30), classified according to KDIGO 2024 criteria.Inclusion criteria: Age 40–70 years; diagnosis of T2DM per ADA 2025; stable therapy ≥ 3 months.Exclusion criteria: CKD stage ≥ 3, acute kidney injury in prior 3 months, severe comorbidities or anticoagulant use, pregnancy/lactation.Data collection: Parameters included age, diabetes duration, BP, HR, serum creatinine, urea, HbA1c, daily glycemic profile, total cholesterol, triglycerides, INR, fibrinogen, APTT, PTI.Ethics: Approved by the Local Ethics Committee of Tashkent Medical University (protocol № [XXX/2024]); informed consent obtained.Statistical analysis: Data reported as mean ± SD. Welch’s t-test was used; mean differences, 95% CIs, and Cohen’s d were calculated; p < 0.05 considered significant.
3. Results
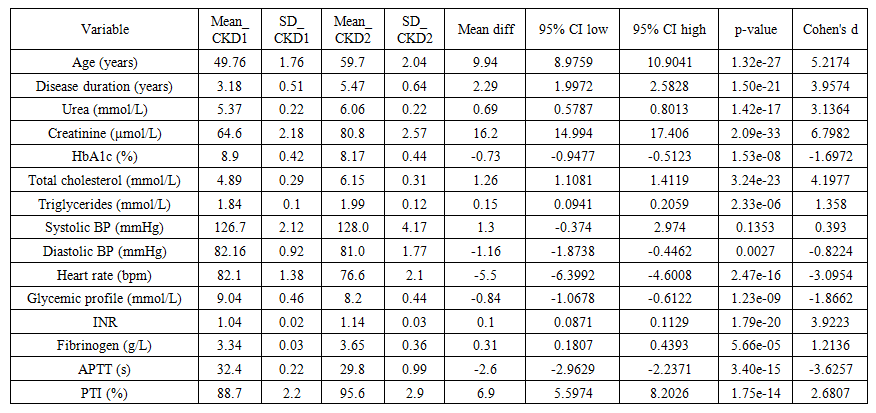 | Table 1. Comparative results between CKD stage 1 and stage 2 in T2DM |
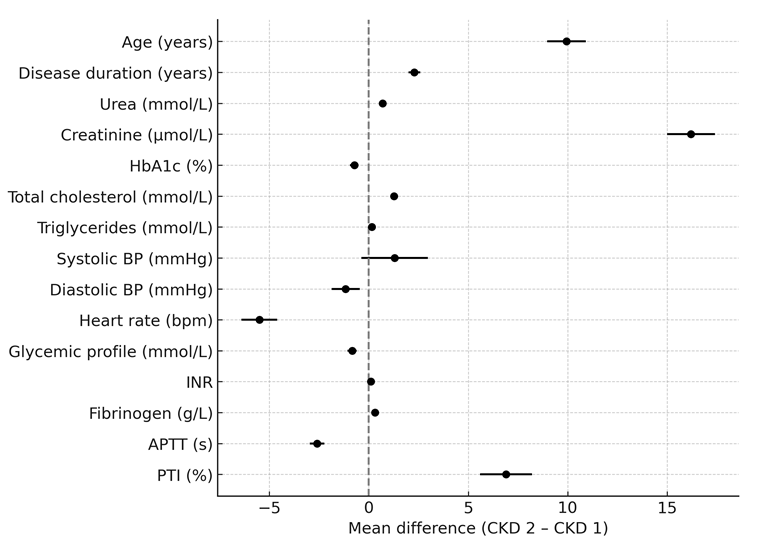 | Figure 1. Forest plot of mean differences with 95% CI |
4. Discussion
- Our results demonstrate that the transition from CKD stage 1 to stage 2 in T2DM is accompanied by significant metabolic, lipid, and coagulation changes. Very large effect sizes for age, creatinine, and diabetes duration indicate clinically meaningful differences. The lipid profile in stage 2 reflected CKD-associated dyslipidemia [2,6], while the coagulation profile suggested a pro-thrombotic [7,8] shift. Despite slightly lower HbA1c in stage 2, glycemic control remained suboptimal in both groups.These findings reinforce KDIGO 2024 [3] and ADA 2025 [4] recommendations for early, multidomain intervention to slow CKD progression and reduce cardiovascular events.
5. Conclusions
- Even at CKD stage 2, T2DM patients exhibit significant renal, lipid, and hemostatic abnormalities beyond those seen in stage 1. Early identification and management of these changes are essential to prevent further renal deterioration and cardiovascular complications.