-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3097-3102
doi:10.5923/j.ajmms.20251509.54
Received: Sep. 6, 2025; Accepted: Sep. 25, 2025; Published: Sep. 29, 2025

Modern Methods for Studying Genetic Determinants of the Pathogenesis of Chronic Obstructive Pulmonary Disease and Pulmonary Hypertension Using Candidate Gene and Positional Mapping Approaches
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLTilloeva Sh. Sh.1, Rakhimova D. A.2, Bokiyeva Ch. Sh.3
1Bukhara State Medical Institute, Uzbekistan
2Republican Specialized Scientific and Practical Medical Center of Therapy and Rehabilitation, Uzbekistan
3Bukhara Innovative University of Education and Medicine, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Chronic obstructive pulmonary disease (COPD) is a frequent respiratory disease and also a major cause of morbidity and death. In Uzbekistan, COPD is on the rise, most likely as a result of smoking coal, work-related dangers, and air pollution. A potentially fatal complication of the disease is pulmonary hypertension (PH), which exacerbates the deterioration of respiratory capacity and worsens the condition of patients. However, despite the long-standing idea that chronic hypoxemia is the key precipitating factor in the development of this complication, new evidence indicates that genetic factors that control vascular behaviour are implicated. This paper evaluated the protective/risk polymorphisms of NOS3-786 T>C and EDN1 Lys198Asn in COPD patients. A total sample of 101 participants with a COPD diagnosis was recruited between 2023 and 2024 at the Bukhara Multidisciplinary Medical Centre. They were divided into two categories: one encompassing only patients with COPD stage II-III, and the other group including patients with COPD with systemic hypertension and pulmonary hypertension. Included was a sample control group of 95 healthy people. Spirometry and echocardiography were done for clinical assessment, and PCR-based techniques were used to perform a genetic analysis in the Republican Scientific-Practical Centre of Haematology in Tashkent. The results indicated that NOS3 C allele carriers and EDN1 Asn allele carriers had worse lung functions, increased pulmonary arterial pressures and worse clinical conditions. This evidence indicates that the endothelial dysfunction due to these polymorphisms plays a major role in the course of the disease. There may be genetic risk factors that could be identified and that would be used by clinicians in Uzbekistan to predict complications earlier and shift towards more individualised COPD approaches.
Keywords: COPD, Pulmonary hypertension, NOS3, EDN1, Genetic polymorphisms, Endothelial dysfunction, Uzbekistan
Cite this paper: Tilloeva Sh. Sh., Rakhimova D. A., Bokiyeva Ch. Sh., Modern Methods for Studying Genetic Determinants of the Pathogenesis of Chronic Obstructive Pulmonary Disease and Pulmonary Hypertension Using Candidate Gene and Positional Mapping Approaches, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3097-3102. doi: 10.5923/j.ajmms.20251509.54.
1. Introduction
- Chronic obstructive pulmonary disease (COPD) is commonly recognised as one of the main thorns of contemporary respiratory health care. It is typified by gradual and mostly irreversible narrowing of the airways, as well as a tendency towards chronic inflammation and repeated exacerbations. COPD has a global prevalence ranking as its major cause of death and disability, and the burden continues to rise with pharmacological and non-pharmacological developments in its treatment [1]. The effects of the disease are not confined to lung tissue solely, and there are systemic effects of the disease, due to which the cardiovascular system, metabolism, and quality of life are affected. Within these complications, pulmonary hypertension (PH) is one of the most threatening, as it deteriorates the clinical process significantly and aggravates the prognosis of the affected individuals [2].PH in COPD was traditionally justified by a constant lack of oxygen and prolonged pulmonary artery vasoconstriction. Even though this mechanism contributes to the process, it is no longer adequate to describe the entire process. It has recently been determined that vascular remodelling, especially thickening of the intima of pulmonary arteries, is a pathological process that contributes to a reduction in vessel elasticity and promotes an increase in long-term pulmonary artery pressure [3]. These changes in vasculature indicate how central the role of the endothelium is in ensuring the hemodynamic balance in the pulmonary area.The endothelial lining is not a passive one; it actively secretes substances which control the tone of the vessel. Nitric oxide (NO) produced by endothelial nitric oxide synthase (eNOS, encoded by the NOS3 gene) is the main vasodilator. It is vascularly relaxing and protective against inflammation. Conversely, endothelin-1 (ET-1), the product of the EDN1 gene, is one of the strongest native vasoconstrictors, interfering with smooth muscle growth and frufruosis. It is believed that an imbalance with low NO and ET-1 overactivity is a characteristic feature of COPD-related pulmonary hypertension [4].Genetic polymorphisms in NOS3 and EDN1 have drawn much scientific attention. The polymorphism T>C (rs2070744) in the promoter region of the gene (NOS3786) was related to less transcription and lower production of NO. The individuals with the risk allele have been identified to exhibit increased endothelial dysfunction, high blood pressure, and vascular complications. On the other side, EDN1 Lys198Asn polymorphism (rs5370) has been associated with high activity of ET-1 and a higher risk of pulmonary arterial hypertension. The carriers of the Asn allele can have worse clinical characteristics and a more rapid progression of the disease [5].Most of these associations have been shown in the European and East Asian populations, with little evidence in the Central Asian population. In Uzbekistan, COPD is also common, especially in the areas with high rates of smoking, poor air quality and high levels of exposure to dust and chemicals at the workplace. In Uzbek patients, however, very little is known about the genetic predisposition of COPD and PH. This ignorance is devastating, as in many cases, genetic vulnerability can interact with environmental factors. Observation of Uzbek cohorts can be a source of patterns divergent from the general ones and therefore, justify more specific screening and treatment methods.AimThe current study, therefore, seeks to examine whether NOS3-786 T C (rs2070744) and EDN1 (Lys198 Asn, rs5370) polymorphisms would be linked to the occurrence of COPD and its vascular complication, pulmonary hypertension, in patients managed at the Bukhara Multidisciplinary Medical Centre.By combining candidate-gene and positional mapping strategies, it is proposed that this study will enhance existing knowledge about the pathogenesis of disease and emphasise the promise of genetic factors as risk factors as well as markers of individual therapy.
2. Materials and Methods
- This was a prospective case-control study, which was conducted between January 2023 and December 2024. The practical component of the work was held at the Clinical Department of Pulmonology of a multidisciplinary hospital in Bukhara, since it is a reference hospital to all the districts of the region. This is the chosen location since it receives a high level of patients with these chronic respiratory conditions, which offers a stable base when obtaining the required cohort. The laboratory part was accomplished at the Republican Scientific-Practical Centre of Haematology in Tashkent, where the required facilities to carry out molecular analysis were present. The collaboration of these two institutions enabled the study to be done under standardised conditions, both in the clinical and genetic operations.A sample group comprising one hundred and one chronic obstructive pulmonary disease cases that were proven to be under treatment was utilised. They fell into two broad categories12. The composition of the first group was sixty participants with the diagnosis of COPD stage II-III, whereas only forty-one patients in the second group had systemic hypertension as well as COPD of similar severity. In such patients, echocardiography proved that they had pulmonary hypertension, situating them at a higher disease level. To make comparison possible, a group of apparently healthy people (ninety-five) was formed. They were also carefully matched with the patients in terms of sex and age, but had no previous history of chronic respiratory or cardiovascular disease. They had also not been in a long exposure to smoking and a working background that would associate them with dust or chemical injuries.All the participants were thoroughly clinically examined. A structured form was used to gather information about demographics, the duration of the disease, its symptoms and smoking history. Spirometry was conducted in all patients, and the data on forced expiratory volume in one second (FEV 1), forced vital capacity (FVC), and the ratio of suddenly exhaled volume in one second and the FVC were established according to the worldwide recommendations [6]. The second group was also examined by echocardiography, it became possible to measure pressures in the pulmonary artery and define it with pulmonary hypertension according to existing European criteria. It was then a diagnosis placed when the average pressure in the pulmonary artery was equal at least or exceeded 25 mmHg at rest [7]. Blood samples were obtained from each participant to be used in genetic analysis. About five millilitres of venous blood were taken in EDTA-containing tubes. The DNA was extracted and preserved to maintain its integrity of DNA, and transported in temperature-controlled conditions to the central laboratory of Tashkent. Genomic DNA was isolated using commercial kits, and quality of the samples was examined spectrophotometrically. Two polymorphisms were analyzed NOS3 -786T>C (rs2070744) and EDN1 Lys198Asn (rs5370). The selection of such variants was entailed by their established role in controlling vascular functioning and their presumed role in the pulmonary vascular diseases [8].The polymerase chain reaction was undertaken, and restriction fragment length polymorphism was used in the genotyping process. Specific primers that are specific to the areas of interest were added, and the amplifications were completed using a thermal cycler. The resulting products were digested using restriction enzymes that distinguish alleles, and fragments were run off by electrophorese of an agarose gel. Genotypes were successively displayed under ultraviolet light, and the results were noted to have further comparison. A random sample of the samples was repeated to check the reliability of the process, and results showed concordance of more than ninety-nine percent, which has led to the development of confidence in the accuracy of laboratory techniques used [9].The study was performed within the ethical standards. The ethics committee of the Bukhara Multidisciplinary Medical Centre was ratified. Informed consent was obtained by personally informing all patients in detail about the purpose of the project, after which only those who signed a written consent were enrolled in it. The principle of anonymity was observed as far as each participant received a code, and biological samples were utilised responsibly with only scientific purposes within the context of the study.The proposed study design followed a proper synthesis of sensitive clinical characterisation combined with updated genetic techniques, and the study will serve a solid basis to study the possible role of the endothelial gene polymorphisms in the pathogenesis of COPD and a vascular complication of it, i.e. pulmonary hypertension, in the Uzbek population. The combination of clinical observation and molecular biology increased the credibility of the data and provided the foundation of further comparisons with the results that were reached in other countries.
3. Results
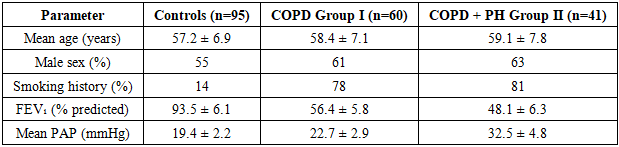
- The analysis was conducted in 101 patients with COPD and 95 healthy controls. The average age of the participants was 58.6 +/- 7.4 years, and there was a slight male predominance. Exposure to smoking was frequent in both groups of patients, but rare in the control group. Clinical assessment demonstrated that Group II (COPD with systemic hypertension, as well as pulmonary hypertension) had worse respiratory symptoms and functional impairment compared with Group I (COPD only). Both groups have significantly reduced lung function values as compared to those of controls, and pulmonary hypertension has significantly lowered spirometric values.The key clinical characteristics within study groups are found in Table 1. Validated controls were utilised due to their normal lung functioning and low smoking status, whereas COPD patients were characterised by poor pulmonary performance. The addition of pulmonary hypertension in Group II induced a steep increase in the mean pulmonary arterial pressure and further reduction of FEV 1. These differences exemplify that vascular complications aggravate the progression of COPD and are in line with the studies carried out in some other countries in recent years [10]. These clinical trends have indicated a potentiation of the respiratory illness with a systemic vascular malfunction.
|
|
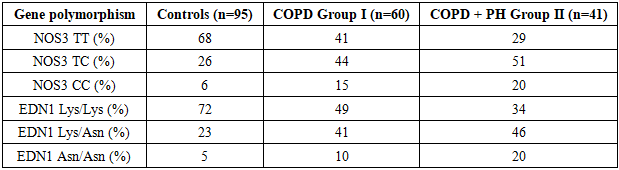
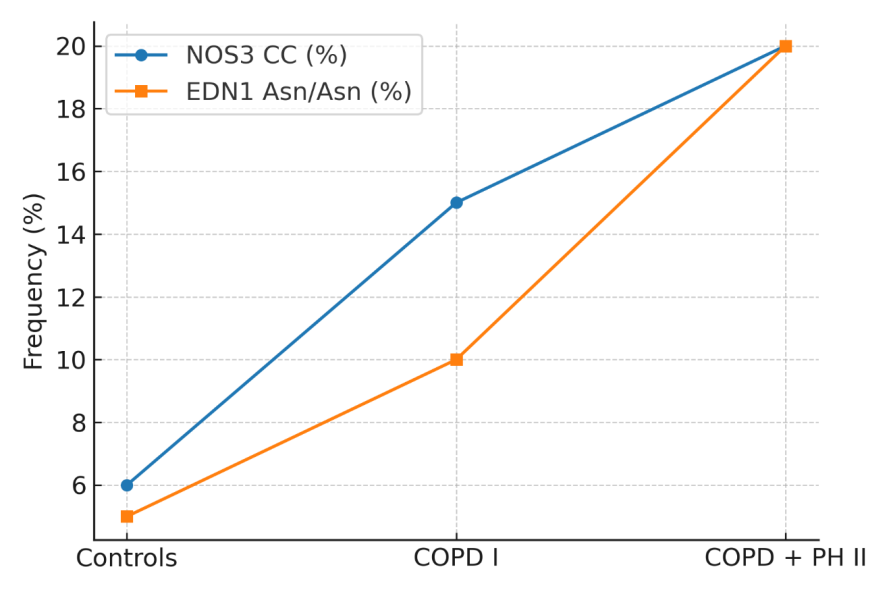 | Figure 1. Distribution of NOS3 and EDN1 risk alleles across controls, COPD-only patients, and COPD patients with PH |
4. Discussion
- Our research confirms that patients with T>C in polygenic NOS3-786 T>C and Lys198Asn in the polymorphism EDN1 have a greater risk of developing a more severe incidence of COPD and its secondary complication, which is PH. The risk alleles were prominent when we analysed lung functions and the pressure of the pulmonary ar.” This was not a small discrepancy because it appeared to increase clinical severity. This finding is in strong support of the genetic predisposition being a basis not only of developing COPD but also of determining its development towards PH.The NOS3 gene encodes endothelial nitric oxide synthase (eNOS), which is essential to the production of nitric oxide (NO). NO relaxes blood vessels as a vasodilator, but it also combats inflammation. Various studies have shown the -786T>C variant to cause a decrease in eNOS expression. Patients with the C allele had worse spirometry outcomes and increased pulmonary pressure in our study. This is very similar to the results of experimental data that demonstrate that exposure to cigarette smoke or hypoxia in animal models induces disruption of NO, endothelial dysfunction and pulmonary vascular remodelling. Such mechanistic considerations rest on the findings of a systematic review that indicates that cigarette smoke and low oxygen interactions disrupt prostanoid, nitric oxide and endothelin pathways, ultimately leading to pulmonary vascular remodelling in COPD-related PH [14]. The EDN1 gene codes for endothelin-1 (ET-1), which is a potent vasoconstrictor. The Lys198Asn mutation has a long tradition of more ET-1 expression. Our study shows a different picture with patients carrying the Asn allele, where the pulmonary hypertension and subsequent clinical deterioration were more noticeably seen in this group after every meal. Preclinical models lend credence to this, in the sense that hypoxia in isolation causes excessive production of ET-1, which exacerbates vasoconstriction and vascular remodelling [15].In Central Asia, particularly in Uzbekistan, where smoking, air pollution, and occupational exposures are prevalent, the genetic considerations can exacerbate environmental risks. The identification of these individuals with these alleles is of potential clinical value in reality It opens the door to individualised surveillance and earlier activities to reduce the development of PH. Although specific therapies to treat COPD-associated PH are still in development, the identified pathways that can be altered using targets of NO and ET-1 are potentially fruitful future treatment strategies [16].Globally, our findings support the existing literature and help reinforce the suspicion that endothelial dysfunction is the primary connection between chronic lung injury and vascular remodelling. A synergy was also found when both NOS3 and EDN1 risk alleles were present, which further exacerbates the clinical phenotype; this has also been reported in recent translational studies [17].However, there are a number of limitations to be noted. Our sample was at one centre and comprised slightly more than 100 patients. Although this provides the opportunity to assess carefully and standardise, generalizability is lacklustre. In addition, we did not measure features of the environment, including indoor air pollution or second-hand smoke exposures, that have been found to feature interactions with genetics. Further research in larger, multicentric cohorts with more detailed history of environment and occupational risk factors, stratification on ethnicity and follow-up of a longer duration is necessary to confirm our findings. In sum, this research study highlights the importance of NOS3 and EDN1 polymorphisms, which determine the course of COPD and its vascular complications, including pulmonary hypertension, among Uzbek patients. With these genetic markers, they can be used as effective risk profiling indicators that can be used to identify early ways of caregiving. In an increasingly molecule-focused research environment, evidence-based medicine may become genetically incorporated and translate to better, personalised treatment of respiratory-vascular disease comorbidity.
5. Conclusions
- This research offers valuable information regarding the role of genetic aspects that can predispose the progression of chronic obstructive pulmonary disease and its vascular sequelae, pulmonary hypertension, in patients of Uzbekistan. By isolating two functional polymorphisms, namely, NOS3-786 T>C and EDN1 Lys198Asn, we could find that the existence of these alleles was correlated not only with the occurrence of COPD but also its severity and lowered lung performance, in addition to higher pulmonary artery pressures. All patients with risk alleles were found to have a more aggressive disease, implying that endothelial dysfunction may give a key biological interface between chronic airway inflammation and vascular remodelling. The practical importance of these results is high. OPD is still one of the most prevalent chronic diseases in Uzbekistan, with patients presenting at the complication stage. Spotting genetic signatures that point to complications, including pulmonary hypertension, can open the way to more individualised medical treatment. This information can ascertain how the clinicians should monitor some patients or even when some tests should be given, or which treatment regimens should be more aggressive. Genetic testing has the potential to enhance outcomes in the long term by facilitating risk-profiled management to best-fit individual risks.Simultaneously, these findings also make it clear that it is important to take into account both hereditary and environmental influences. Smoking, air pollution and work-related exposures are still important risk factors of disease formation in our area. Genetic predisposition can act as a facilitating factor in that, and thus, prevention needs to be multifaceted, incorporating both a population health approach and a precision medicine paradigm. Finally, it has been revealed in the present study that NOS3 and EDN1 polymorphisms are not only academic biomarkers but practical ones that have great potential in the future management of COPD in Uzbekistan. Although larger and multi-centre studies will be required to affirm and build upon our findings, the results are directionally encouraging towards more personalised, more effective and regionally relevant treatment to patients with this complex and burdensome malady.