-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3092-3096
doi:10.5923/j.ajmms.20251509.53
Received: Sep. 6, 2025; Accepted: Sep. 26, 2025; Published: Sep. 29, 2025

Optimization of Early Detection of Cervical Intraepithelial Neoplasia Based on a Comprehensive Analysis of Biomolecular and Structural Parameters
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLM. Х. Kattakhojayeva1, E. E. Karshiyeva2
1M.D. Professor, Department of Obstetrics and Gynaecology №1, Tashkent State Medical University, Tashkent, Uzbekistan
2Candidate of Medical Sciences, Department of Obstetrics and Gynecology №1, Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Cervical cancer remains one of the leading causes of cancer morbidity and mortality in women of reproductive age worldwide. According to the International Agency for Research on Cancer (IARC), there are more than 570,000 new cases of cervical cancer and about 311,000 deaths from the disease each year. In the Republic of Uzbekistan, cervical cancer ranks second in the structure of cancer incidence in women after breast cancer, with a standardized incidence rate of 12.8 per 100,000 female population. The modern concept of cervical carcinogenesis is based on the idea of a multi-stage process of malignancy, including successive stages: persistent infection with high-risk human papillomavirus (HPV BP) → cervical intraepithelial neoplasia (CIN) of varying severity → invasive cancer. This process takes an average of 10-15 years, which creates ample opportunities for effective prevention and early detection of precancerous changes.
Keywords: Cervical cancer, Cervical intraepithelial neoplasia, CIN, Precancerous changes, p16^INK4a, Ki-67, Morphometry, Biomarkers, Diagnosis, HPV, Cytology, Immunocytochemistry
Cite this paper: M. Х. Kattakhojayeva, E. E. Karshiyeva, Optimization of Early Detection of Cervical Intraepithelial Neoplasia Based on a Comprehensive Analysis of Biomolecular and Structural Parameters, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3092-3096. doi: 10.5923/j.ajmms.20251509.53.
Article Outline
1. Introduction
- Cervical cancer remains one of the most significant problems of modern oncogynecology, ranking fourth in the structure of cancer incidence among women worldwide. According to the World Health Organization, more than 570,000 new cases of the disease are registered annually, with a mortality rate of about 311,000 cases per year [1]. Of particular concern is the fact that the highest incidence occurs in women of reproductive age (25-45 years), which determines not only the medical, but also the socio-economic significance of this pathology. The development of cervical cancer is a multi-stage process characterized by the sequential transformation of normal epithelium through the stages of precancerous changes of varying severity to invasive carcinoma. A key role in this process belongs to persistent infection with highly oncogenic types of human papillomavirus (HPV), which is detected in 99.7% of cases of invasive cervical cancer [2]. The modern screening system for precancerous diseases of the cervix is based on cytological examination (Pap test) and detection of HPV of high carcinogenic risk. In recent years, the role of molecular and structural markers as additional diagnostic tools for detecting precancerous changes in the cervix has been actively studied [3]. The development and implementation of a comprehensive method for detecting molecular and structural markers of precancerous changes in the cervix is an urgent task of modern oncogynecology aimed at improving the effectiveness of diagnosis and optimizing management tactics for patients with cervical pathology. Precancerous changes of the cervix, combined by the term cervical intraepithelial neoplasia (CIN), are classified into three degrees: CIN I (mild dysplasia), CIN II (moderate dysplasia) and CIN III (severe dysplasia and carcinoma in situ). The risk of progression of CIN I to invasive cancer is 1%, CIN II - 5%, and CIN III - 12-40%. At the same time, CIN I often undergoes spontaneous regression (up to 60% of cases), whereas CIN II-III require active treatment [4].Existing screening programs based on cytological examination (PAP test) and HPV testing have certain limitations. The sensitivity of the cytological method for detecting CIN II+ is 53-77%, the specificity is 96-98%. HPV testing demonstrates a higher sensitivity (88-97%), but the specificity decreases to 89-96% due to the high prevalence of transient HPV infections, especially among young women [5]. The main problem of modern diagnostics is the inability to accurately predict the course of precancerous changes based on existing research methods. A significant proportion of women with HPV-positive status and even with cytological abnormalities will never develop invasive cancer, which leads to overtreatment with corresponding psychological, economic and medical consequences [6]. In recent years, the role of molecular biomarkers in the diagnosis and prognosis of precancerous changes in the cervix has been actively studied. Special attention is paid to the proteins p16 INK4a and Ki-67, the expression of which reflects cell cycle disorders characteristic of neoplastic transformation. The p16^INK4a protein is a surrogate marker of the functional activity of oncogenes E6 and E7 of highly oncogenic HPV types, and Ki-67 reflects the proliferative activity of cells [7]. The immunocytochemical determination of p16^INK4a/Ki-67 (CINtec PLUS test) showed high efficiency in detecting CIN II+ with a sensitivity of 86-100% and a specificity of 43-87%. However, the interpretation of the results is often difficult due to the subjectivity of the assessment and the lack of standardized criteria [8]. A promising direction is the study of structural changes in the nuclei of the cells of the squamous epithelium of the cervix during neoplastic transformation. Morphometric analysis makes it possible to objectify the assessment of nuclear atypia, which is a key diagnostic criterion for dysplasia. Modern computer image analysis systems open up new possibilities for automated morphometry and reduce the subjectivity of interpretation of the results [10]. The integration of molecular and morphometric approaches can significantly improve the accuracy of the diagnosis of precancerous changes and improve the prediction of their course. A comprehensive assessment of biomarker expression combined with quantitative characterization of cell structural changes will create a more objective and reproducible diagnostic system.The problem becomes particularly relevant in the conditions of the Republic of Uzbekistan, where there is a relatively high incidence of cervical cancer with insufficient coverage of the population by screening programs. Improving the methods of early diagnosis of precancerous changes is a priority for reducing cancer morbidity and mortality in the female population.The aim of the study was to improve the diagnosis of precancerous changes in the cervix by developing a comprehensive method for assessing molecular and structural markers.
2. Research Materials and Methods
- A prospective single-center study was conducted at the Department of Oncology and Medical Radiology of Tashkent State Medical University in cooperation with the Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology of the Ministry of Health of the Republic of Uzbekistan in the period from January 2022 to December 2025. The study included 185 women aged 25 to 65 years who applied for a preventive examination or for pathological changes in the cervix.Inclusion criteria:• Age 25-65 years• The presence of a cervix• Informed consent to participate in the study• The possibility of dynamic monitoring for 12 monthsExclusion criteria:• Pregnancy• Previous operations on the cervix• The use of immunosuppressive therapy• Malignant neoplasms of any localization in the anamnesis• Pelvic inflammatory diseases in the acute stageGroup distribution:• Group 1 (control group): 95 women with normal cytology and negative HPV test• Group 2: 78 women with CIN I• Group 3: 67 women with CIN II• Group 4: 45 women with CIN IIIThe material was taken using Cervex-Brush® brushes, followed by preparation of preparations using liquid cytology (ThinPrep®). The staining was carried out using the Papanicolaou method. The interpretation of the results was carried out according to the Bethesda system (2014). Determination of HPV DNA of high oncogenic risk (types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68) using the real-time polymerase chain reaction method using the AmpliSens® HPV WRC genotype-FL test system. It was performed on all patients with abnormal cytology. The sampling of the material was carried out by the method of punch biopsy under colposcopic control. The histological classification was carried out according to WHO recommendations (2020). The expression of p16^INK4a and Ki-67 was determined on cytological preparations using ready-made cocktails of primary antibodies: Antibodies to p16^INK4a (clone E6H4, Roche), Antibodies to Ki-67 (clone 30-9, Roche). Visualization was performed using the OptiView DAB IHC Detection Kit. The results were evaluated according to the CINtec PLUS atlas. Morphometric measurements were performed using the ImageJ image analysis system (NIH, USA) at magnification ×1000. At least 100 cell nuclei of the surface and intermediate layers of the squamous epithelium were analyzed for each sample. Statistical data processing was carried out using the SPSS 26.0 program. Descriptive statistics methods, correlation analysis (Pearson coefficient), and ROC analysis were used to evaluate diagnostic effectiveness. The differences were considered statistically significant at p<0.05.
3. The Results of the Study
- The endometrium in CIN, as in normal and pathological conditions, formed the inner layer of the uterine walls. It consisted of a layer of cylindrical epithelium lining the surface of both the gland and its own plate of connective tissue associated with the myometrium. The latter was permeated by simple tubular glands that opened onto the surface of the epithelium, and their deepest parts reached the myometrium. Groups of ciliated cylindrical cells are scattered among the secretory cells. The endometrium consisted of two layers: a superficial, thick, functional layer, and a deeper, basal layer. The mucous membrane was represented by a cylindrical epithelium. In the presence of CIN, both its thickness and topography changed. In addition, we noted the following changes in its morphology, depending on the severity of the disease. The histological gradation of lesion severity depended on the number and location of immature undifferentiated cells in the epithelial stratum – its stratification. Thus, at CIN 1, the thickness of the endometrium did not significantly differ from the norm and had slight differences in its topography. At the same time, morphological changes in dysplasia of this severity included: a violation of the stratification of the squamous epithelium mainly in the basal regions, a change in cell polarization relative to the basement membrane, single dividing cells, minor dyskariosis, as well as signs of viral damage — coilocytic atypia in the superficial epithelium, dyskeratosis, para- and hyperkeratosis of the epithelium. Characteristic of this stage of pathology were undetected changes in the structure of the epithelium with moderate proliferation of cells of the basal layer. Coilocytosis and dyskeratosis were found only in isolated samples. Undifferentiated cells occupied the lower third of the epithelial layer. Minor epithelial dysplasia was observed, which was localized mainly in the basal part of the epithelium and occupied no more than a third of the area. In addition, cystic growths were detected in tissues with altered epithelial cells, and in some fragments with cystic growths. Some of them contain accumulations of red blood cells, with stasis, up to the formation of blood clots (Fig.1,2,3,4). The relative content of arterial vessels in the endometrium decreased. Along with this, some of them were expanded and full-blooded. As well as the content of individual cysts, where accumulations of red blood cells were observed, often with hemolysis, up to the formation of blood clots.
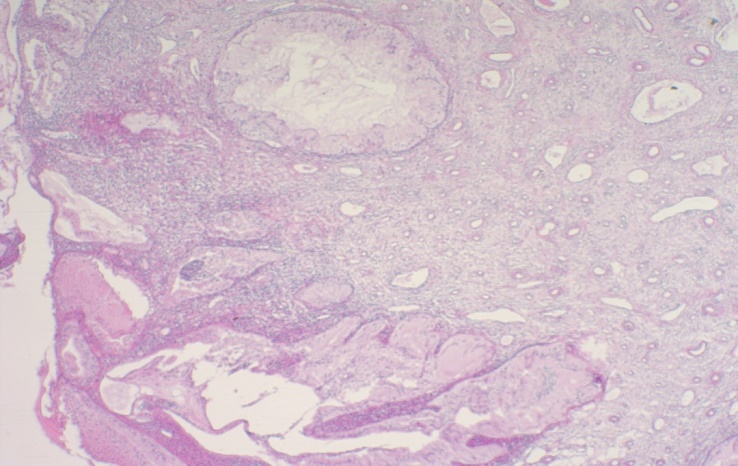 | Figure 1. Fragment of the cervix. CINI. Chronic cervicitis. A polypoid fragment of the cervix covered with endocervical epithelium. It forms an uneven layer in thickness. Squamous intraepithelial lesions of low severity. Severe lymphoplasmocytic infiltration of the stroma. Small retention cysts with clusters of neutrophils. Light microscopy. Hematoxylin and eosin staining (x100) |
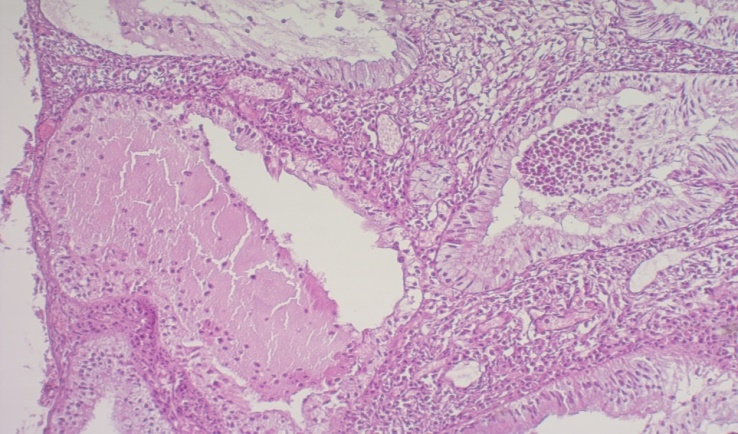 | Figure 2. (fragment of fig.1). Fragment of the cervix. CINI. Chronic cervicitis. A polypoid fragment of the cervix, covered with endocervical epithelium, with pronounced lymphoplasmocytic infiltration of the stroma, small retention cysts. Focal areas of necrosis. Accumulations of neutrophils. Changes in the structure of the epithelium with moderate proliferation of cells of the basal layer.Light microscopy. Hematoxylin and eosin staining (x 400) |
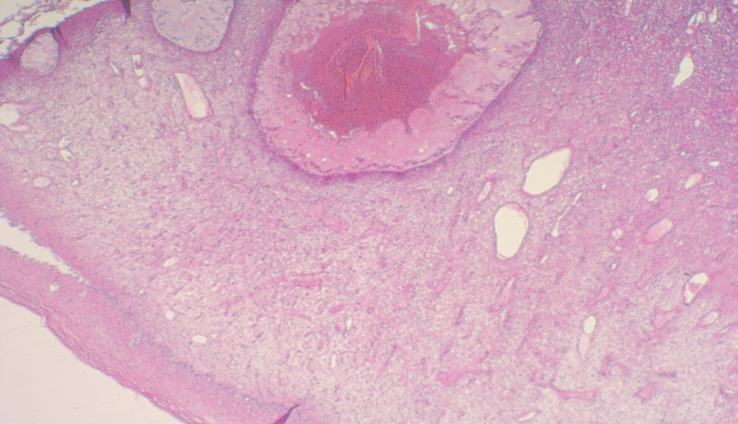 | Figure 3. Fragment of the cervix. CINI. A fragment of the cervix covered with multilayered squamous epithelium, in places with parakeratosis and mild acanthosis, with retention cysts in the underlying stroma and hemorrhage in one of them. Light microscopy. Hematoxylin and eosin staining (x 100) |
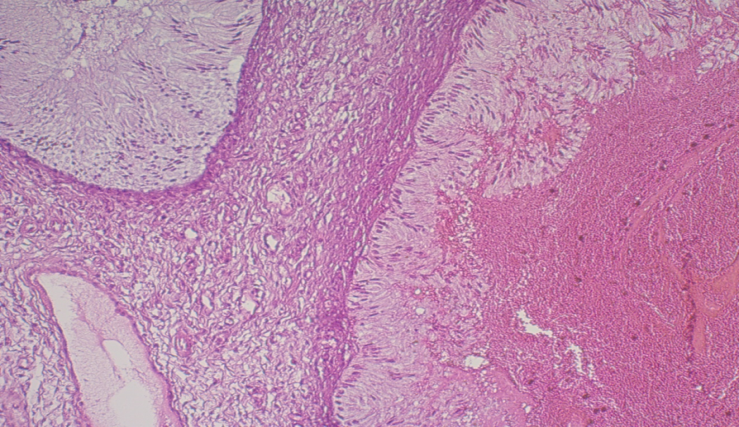 | Figure 4. (fragment of fig.3). Fragment of the cervix. CINI. A fragment of the cervix with retention cysts in the underlying stroma and hemorrhage in one of them with the onset of thrombus formation. Sclerosis of the stroma. Light microscopy. Hematoxylin and eosin staining (x 400) |
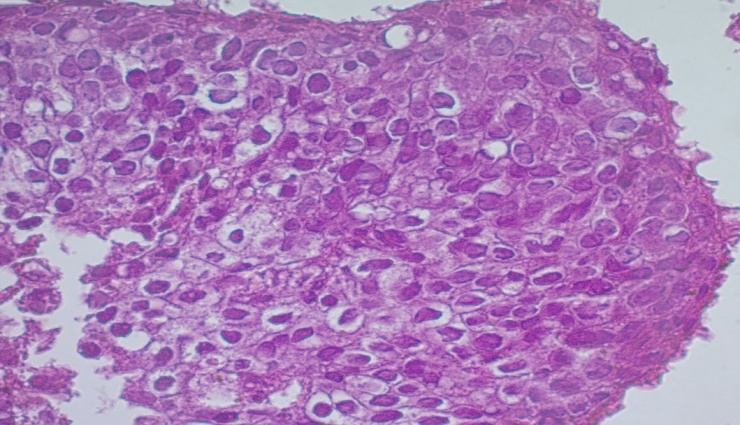 | Figure 5. Fragment of the cervix. CINIII. Fragments of squamous epithelium without underlying stroma with structural features of HSIL: lack of maturation throughout the epithelial layer, few mitoses in the surface sections, nuclear polymorphism and hyperchromia. Necrosis of the nuclei. Light microscopy. Hematoxylin and eosin staining (x400) |
4. Conclusions
- Thus, changes in the endometrium in CIN progressed sequentially as the severity of the disease increased. The pathomorphological changes were based on a violation of the topography of the layer. In addition, the content of tissue sites with alterative processes increased (up to necrosis and desquamation). The area occupied by cystic formations with desquamation of the epithelium and accumulation in individual blood structures increased, up to thrombosis. Nuclear polymorphism and hyperchromia gradually formed. In CINIII, squamous intraepithelial lesion of high severity has already been detected. The stroma of the superficial sections was often marked by lymphoplasmocytic infiltration. Tangles of thick-walled vessels were observed.