-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3015-3019
doi:10.5923/j.ajmms.20251509.36
Received: Aug. 26, 2025; Accepted: Sep. 20, 2025; Published: Sep. 23, 2025

Morphometric and Immunohistochemical Analysis of Congenital Bronchial Malformations in Newborns
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShevketova Lilia Shevketovna1, Mahkamov Nosirjon Jūrayevich2
1PhD, Andijan State Medical Institute, Andijan, Uzbekistan
2DSc, Associate Professor, Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Shevketova Lilia Shevketovna, PhD, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Congenital bronchial malformations in newborns are associated with dysontogenetic disruptions in airway development, complicating early diagnosis and clinical management. Morphometric and immunohistochemical analyses provide critical information on structural and cellular alterations, including bronchial wall layers, capillary networks, myofibroblast activity, and endothelial cell distribution. Morphometric measurements allow quantitative and statistically robust evaluation of cell number and distribution patterns, while immunohistochemistry identifies tissue-specific markers such as CD31, CD34, and SMA, elucidating angiogenesis, fibrogenesis, and smooth muscle activity. The integration of these approaches holds translational significance by linking microscopic tissue changes to clinical outcomes, supporting early detection, prognostic assessment, and the development of individualized therapeutic strategies. This integrative approach enhances the understanding of the pathogenesis of congenital bronchial malformations and informs evidence-based neonatal care.
Keywords: Congenital bronchial malformations, Newborns, Morphometry, Immunohistochemistry, Translational significance, Bronchial development
Cite this paper: Shevketova Lilia Shevketovna, Mahkamov Nosirjon Jūrayevich, Morphometric and Immunohistochemical Analysis of Congenital Bronchial Malformations in Newborns, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3015-3019. doi: 10.5923/j.ajmms.20251509.36.
Article Outline
1. Introduction
- Congenital bronchial malformations (CBM) in neonates represent disontogenetic disturbances of the respiratory system, with an estimated incidence ranging from 1 in 25,000 to 1 in 35,000 live births [1,2]. These malformations are often detected prenatally through ultrasound screening or postnatally when infants present with respiratory distress [3,4]. Histopathological evaluation is essential for accurate classification; however, morphology alone is frequently insufficient to distinguish between subtypes [5,6]. Immunohistochemistry has therefore become an indispensable tool, allowing for the detection of tissue-specific markers such as CD31, CD34, and SMA, which provide insight into endothelial cells, myofibroblasts, and smooth muscle activity [5,6].Morphometric analysis enables objective and quantitative assessment of bronchial wall layers, capillary networks, and cell distribution [7]. Combined application of morphometry and immunohistochemistry holds translational significance, facilitating the understanding of CBM morphogenesis, linking microscopic findings to clinical outcomes, and supporting the development of individualized therapeutic strategies [8,9]. Recent molecular genetic studies have further clarified the pathogenic mechanisms, including KRAS mutations in mucinous cell clusters, which may indicate potential malignant transformation [10,11]. Proteomic and transcriptomic profiling of CBM subtypes has revealed differential gene expression, suggesting that these lesions result from complex molecular events rather than simple developmental arrest [10,11].
2. Purpose of the Study
- The purpose of this study is to investigate congenital bronchial malformations in neonates using morphometric and immunohistochemical approaches in order to elucidate their morphogenesis and pathogenic characteristics. Within the study, structures such as bronchial wall layers, capillary networks, and cellular distribution will be quantitatively assessed through morphometric analysis, while the expression of tissue-specific markers including CD31, CD34, and SMA will be evaluated to characterize endothelial cells, myofibroblasts, and smooth muscle layers. This integrated approach aims to provide a comprehensive understanding of CBM at both microscopic and cellular levels, clarify mechanisms underlying their clinical course, and support the development of individualized diagnostic and therapeutic strategies.
3. Materials and Methods
- The object of the study consisted of bronchial tissues obtained from deceased neonates between 2021 and 2024. These tissues exhibited dysontogenetic bronchiectatic alterations. The collection of each sample was ethically approved by the local ethics committee, and written informed consent was obtained from the parents or legally authorized representatives. The bronchial tissues were fixed in 10% formalin for 24–48 hours and subsequently embedded in paraffin blocks. Sections of 4–5 µm thickness were prepared using a microtome and served as the basis for histological analysis. The prepared sections were stained with DAB chromogen, and the following morphologic parameters were assessed in each sample: bronchial wall layers, capillary networks, myofibroblasts, and endothelial cells. Morphometric analysis was performed using the NanoZoomer system (REF C13140-21, S/N000198, Hamamatsu Photonics, Japan), allowing quantification of cell numbers and the percentage of endothelial and myofibroblast expression. Immunohistochemical analysis was conducted using CD31 (PECAM-1), CD34, and SMA (Smooth Muscle Actin) markers. CD31 was employed to evaluate transendothelial migration, angiogenesis, and mechanosensory activity of endothelial cells. CD34 was used to identify mesenchymal cells and endothelial angiogenesis, whereas SMA was applied to assess the activity of smooth muscle layers and myofibroblasts in fibrogenesis.
4. Results and Discussion
- Morphometric analysis was performed on various forms of bronchial anomalies. Prepared micro-samples were scanned using the HAMAMATSU PHOTONICS scanner, and at least 10 regions per sample were evaluated based on digital measurements.For the bronchial segments affected by atresia, sections were obtained at 0.5 cm intervals and scanned using the Nano-Zoomer microscope. Morphometric measurements encompassed the bronchial wall, including the smooth muscle layer, submucosa, epithelial cells, fibrous structures, and blood vessels (Figure-1).
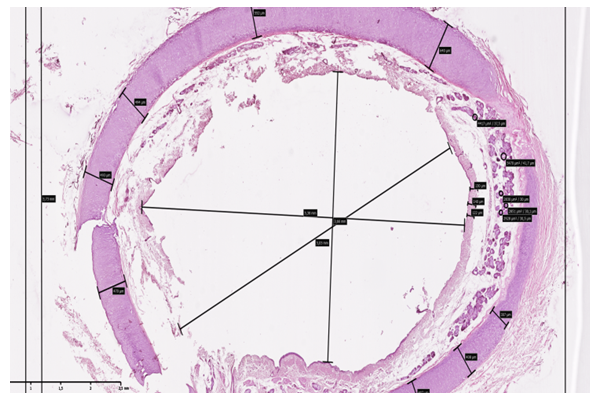 | Figure 1. Morphogram illustrating the thickness of the anatomical layers of the bronchial wall in tracheomalacia. Scanned using NanoZoomer (REF C13140-21.S/N000198/ HAMAMATSU PHOTONICS/431-3196 JAPAN). Staining: H&E. Magnification: 10×10 |
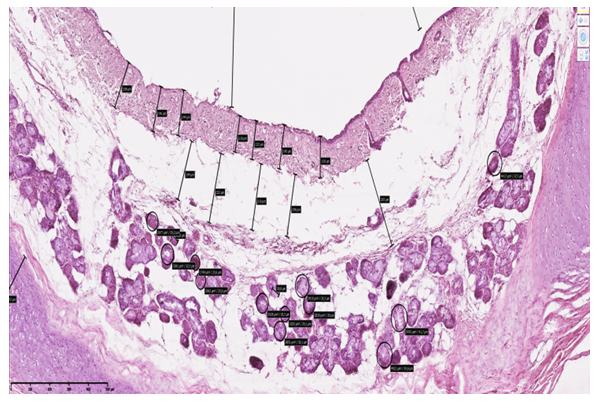 | Figure 2. Morphogram showing the thickness of the anatomical layers of the bronchial wall in the middle segment in cystic fibrosis. Scanned using NanoZoomer (REF C13140-21.S/N000198/ HAMAMATSU PHOTONICS/431-3196 JAPAN). Staining: H&E. Magnification: 10×10 |
 | Table 1. Morphometric parameters of the bronchial wall thickness (in µm) across different clinical and morphological variants of bronchial anomalies |
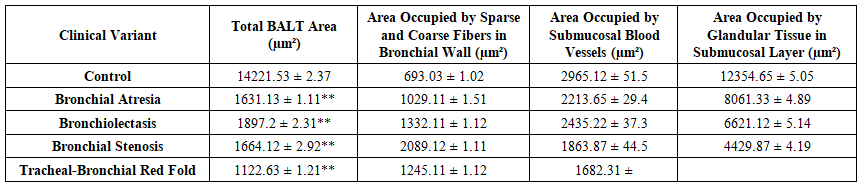 | Table 2. Morphometric parameters of bronchial wall layers, including the submucosal muscular layer and blood vessels, in various clinical morphological types of bronchial anomalies are presented in µm and µm² (up to 64,000 µm²) in an organized manner |
 | Figure 3 |
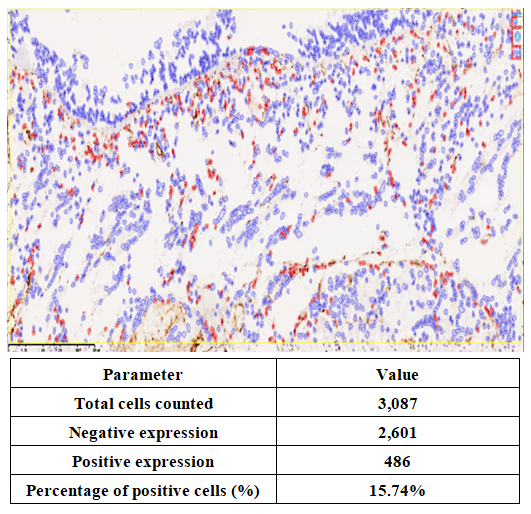 | Figure 4 |
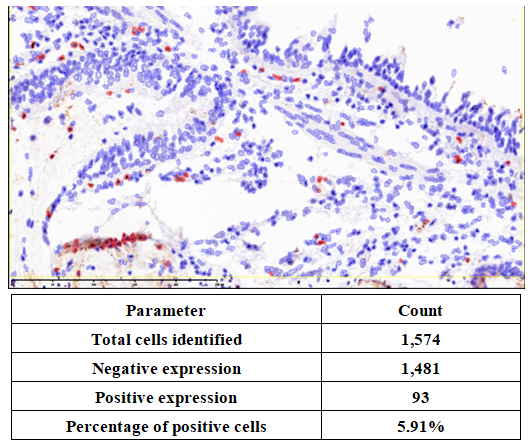
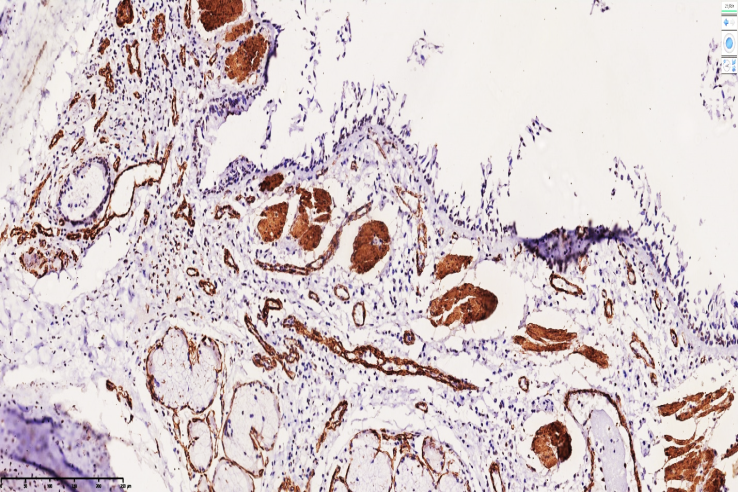 | Figure 5. High positive expression of the SMA marker in the smooth muscle layer of the bronchial wall in tracheobronchomalacia. Most smooth muscle bundles appeared irregular, with wavy texture and markedly altered relief. Staining: DAB chromogen. Magnification: 10×10 |
 | Figure 6. In tracheobronchomalacia, the bronchial wall smooth muscle layer shows high positive expression of the SMA marker. Most myofibroblasts around glandular structures are visualized as dark brown linear staining. Stain: DAB chromogen. Magnification: 10×10 |
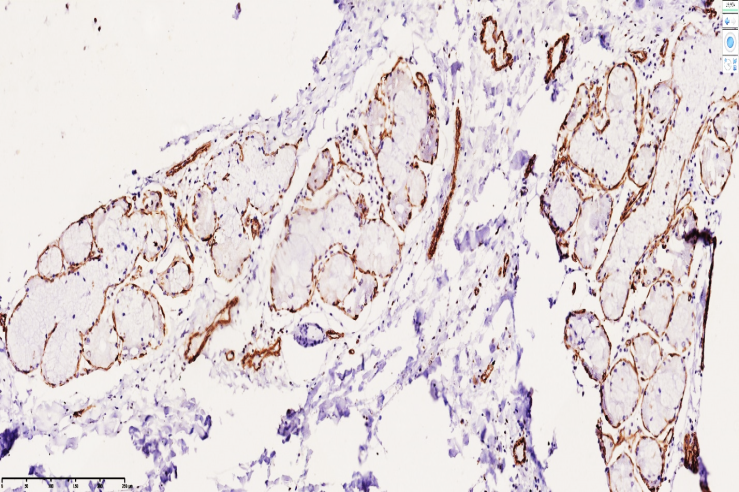
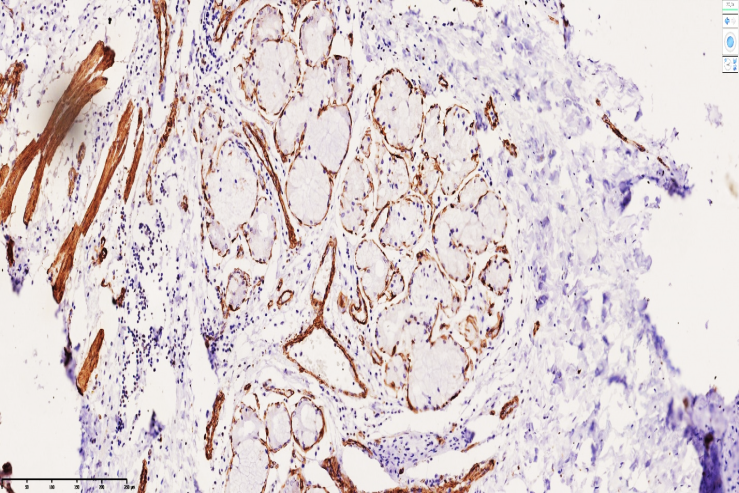 | Figure 7. Positive SMA expression in tracheobronchomegaly (Mounier-Kuhn syndrome). Most smooth muscle fibers appear irregular, with wavy texture and markedly altered relief. Staining: DAB chromogen. Magnification: 10×10 |
5. Conclusions
- Our comprehensive morphometric and immunohistochemical analyses provide novel insights into the structural and cellular alterations associated with congenital bronchial anomalies. Morphometric evaluation revealed significant thinning of the bronchial wall and substantial reductions in BALT structures across different clinical variants, with the most pronounced changes observed in bronchiolectasis. These findings confirm the presence of developmental dysplasia and indicate a predominance of tissue damage in affected bronchi.Immunohistochemical assessment further elucidated the role of vascular and mesenchymal components in bronchial anomalies. CD31 (PECAM-1) expression highlighted endothelial remodeling and mechanotransduction responses, serving as a reliable marker of endothelial integrity and vascular adaptation. CD34 analysis demonstrated active microangiogenesis and mesenchymal proliferation, particularly during the proliferative phase of inflammation, and correlated with bronchial hypoplasia and delayed development.Evaluation of α-SMA expression in bronchial smooth muscle and myofibroblasts revealed high prevalence of myofibroblast-driven fibrogenesis, with marked alterations in muscle bundle organization and perimysial and myofascial membranes. Elevated α-SMA expression in bronchial stenosis, bronchiectasis, tracheobronchomalacia, and tracheobronchomegaly underscores ongoing intramural fibrosis, myofibroblast-to-fibroblast transformation, and collagen deposition, reflecting the pathological progression of these anomalies.Collectively, these findings provide a comprehensive morphofunctional characterization of bronchial developmental anomalies. The integration of morphometric and immunohistochemical data offers predictive value for identifying areas of structural vulnerability, potential complications, and the extent of reparative fibrosis, thereby contributing to improved diagnostic, prognostic, and therapeutic strategies in congenital bronchial disorders.