-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3010-3014
doi:10.5923/j.ajmms.20251509.35
Received: Aug. 25, 2025; Accepted: Sep. 17, 2025; Published: Sep. 23, 2025

Distinctive Pathomorphological and Morphometric Features of Various Forms of Pneumopathies
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAbdullaeva Nurjaxon Juraboy qizi1, Mamataliev Avazbek Ruziyevich2
1Assistant, Andijan State Medical Institute, Andijan, Uzbekistan
2PhD, Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Abdullaeva Nurjaxon Juraboy qizi, Assistant, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study investigated the dynamics of pathomorphological and morphometric changes, as well as dysfunctional alterations, in the development of various clinical and morphological manifestations of pneumopathies in fetuses and newborns of different gestational ages. The research utilized forensic histological and pathohistological archival materials (107 cases) of lung tissues obtained from autopsies of stillborns and infants who died during the intranatal, early, and late neonatal periods in maternity complexes and perinatal centers of the Andijan region between 2021 and 2024. The frequency, prevalence, and severity of pulmonary pathomorphological and morphometric changes in pneumopathies generally depended on the gestational age of the newborn, prematurity or maturity, and the degree of lung tissue differentiation. Hemodynamic disturbances in the lungs were found to cause damage to alveolocytes and alveolar capillaries, disruption of the alveolo-capillary (air-blood) barrier, and transudation of serum proteins, thereby blocking the respiratory surface of the lung parenchyma.
Keywords: Gestational age, Fetus, Newborn, Pneumopathy, Pathomorphology, Morphometry, Atelectasis, Hyaline membrane, Edema, Hemorrhage, Acute respiratory distress syndrome
Cite this paper: Abdullaeva Nurjaxon Juraboy qizi, Mamataliev Avazbek Ruziyevich, Distinctive Pathomorphological and Morphometric Features of Various Forms of Pneumopathies, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3010-3014. doi: 10.5923/j.ajmms.20251509.35.
Article Outline
1. Introduction
- According to the World Health Organization, respiratory system diseases represent one of the most common pathologies and leading causes of mortality among newborns [5,6,7]. Respiratory distress syndrome (RDS), acute respiratory distress syndrome (ARDS), and other pneumopathies are reported to occur at a frequency ranging from 1.5 to 78.9 cases per 100,000 populations in different countries. UNICEF data (2017) indicate that in Central Asian countries, ARDS is among the primary causes of stillbirth and neonatal mortality [1,2].These neonatal pathologies are considered non-inflammatory processes of the lungs and are manifested by atelectasis, edema, hemorrhagic changes, hyaline membranes, and related morphologic features [3,4]. Therefore, investigating the pathomorphological and morphometric characteristics of pneumopathies in neonates, clarifying their pathogenetic mechanisms, and assessing their clinical manifestations remain highly relevant scientific and practical issues in perinatal medicine and neonatology [1–7]. Recent epidemiological data report that RDS accounts for 26% of all neonatal ICU admissions in Egypt, with hyaline membrane disease and pneumonia being the leading causes of neonatal mortality in this population [8]. Globally, over 40% of all childhood deaths occur in the neonatal period, especially among infants born before 32 weeks of gestation, highlighting prematurity as a critical driver of respiratory mortality [9]. In 2023, the incidence of neonatal ARDS (NARDS) was estimated at 1.44%, with pneumonia, perinatal asphyxia, and early-onset sepsis among the top etiologies [10]. Advances in imaging and machine learning now support the classification of neonatal lung pathologies—such as RDS, TTN, and pneumonia-via automated analysis of lung ultrasound images, offering promise for rapid diagnosis in resource-limited settings [11]. Moreover, in new forms of bronchopulmonary dysplasia (BPD), current histopathological understanding reveals alveolar simplification, reduced septation, and persistent hyaline membranes indicating long-term structural impairment [12].
2. Purpose of the Study
- To investigate the distinctive pathomorphological and morphometric features of various forms of pneumopathies.
3. Materials and Methods
- The objects of the study consisted of archival materials of 107 cases of lung tissue samples obtained during autopsies of fetuses and newborns who died from pneumopathies in the perinatal period at maternity complexes of the Andijan region between 2020 and 2024. The study materials included cases of different gestational ages and perinatal periods. Pathomorphological and morphometric parameters were examined in accordance with gestational and neonatal age. The obtained data were analyzed using statistical methods.
4. Results and Discussion
- It is of great importance to accurately identify the specific pathomorphological and morphometric features of alveolar structures in lung tissue affected by pneumopathies in fetuses of different gestational ages and in newborns. In fetuses at 22–28 weeks of gestation, macroscopic and microscopic examinations revealed immaturity of the lungs, characterized by total atelectasis, failure of alveoli to expand, or the presence of only narrow slit-like openings. The respiratory epithelium of the alveolar compartments appeared flattened; arterioles were short; interalveolar connective tissue septa were wide; type I alveocytes were more frequently damaged compared to type II alveocytes; and cellular lysis occurred more rapidly (Figure 1).
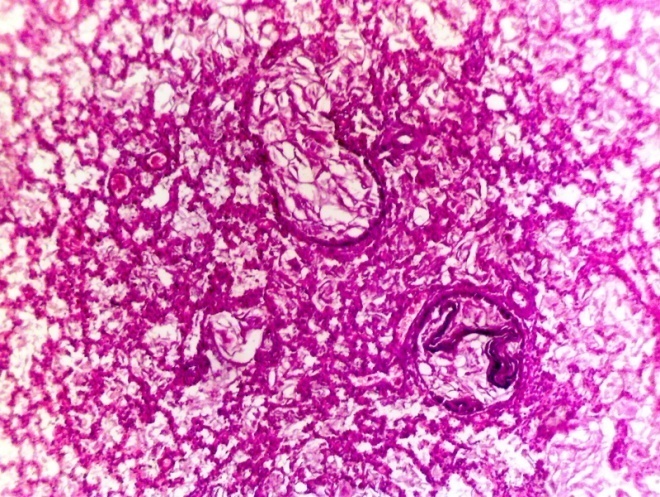
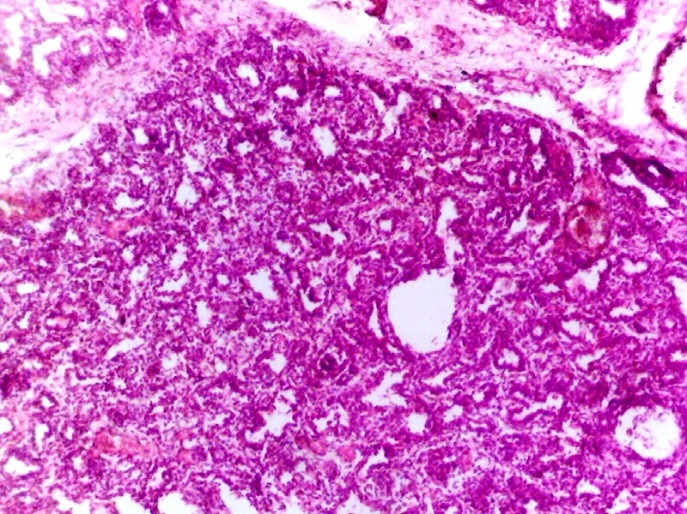 | Figure 1. In immature lung tissue, respiratory bronchioles and some alveoli are partially opened, irregular in shape; stromal edema is present along with foci of primary atelectasis; alveocytes are not yet developed; moderate venous congestion and focal diapedetic hemorrhages are observed. Hematoxylin–eosin staining. Magnification ×4 ×12.5 |
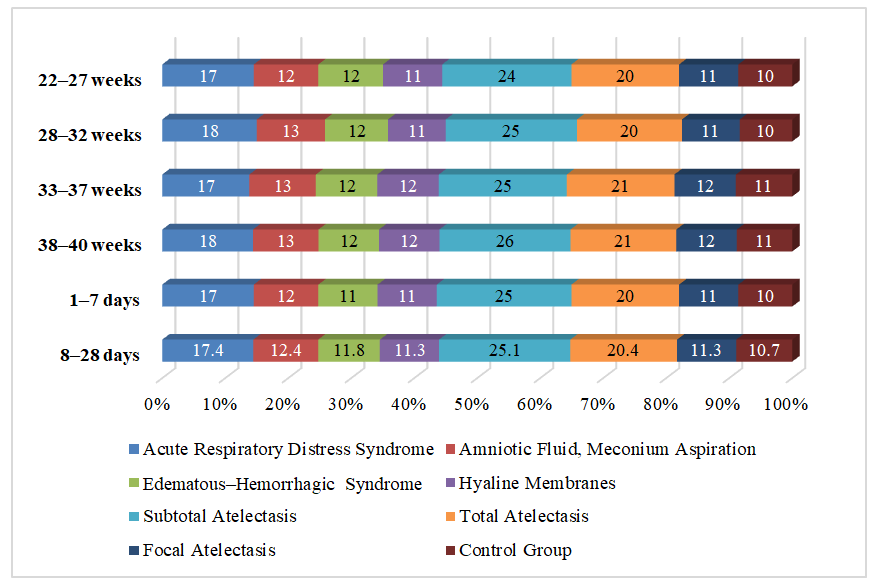
 | Figure 2. Changes in the diameters of type I alveocytes (µm) in various forms of pneumopathies |
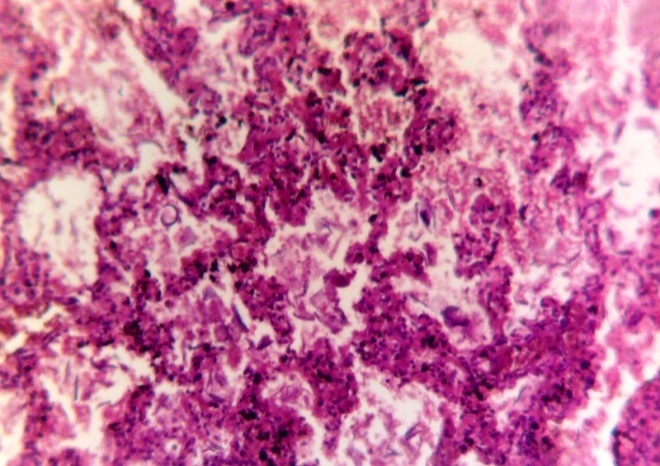
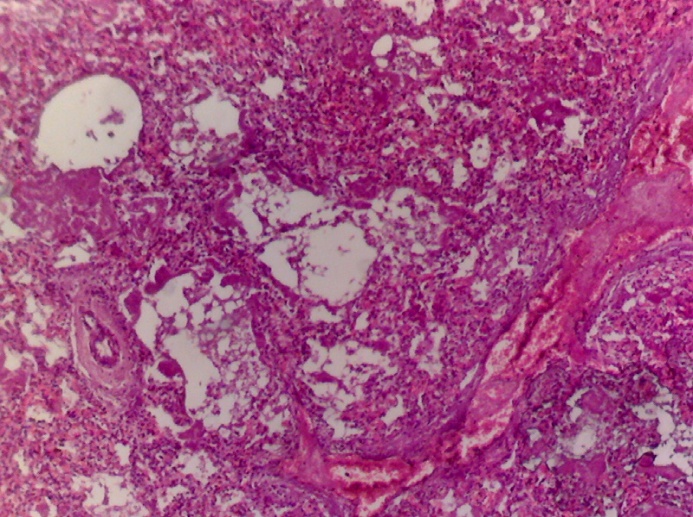 | Figure 3. Partially opened bronchioles and alveolar spaces containing desquamated epithelium and amniotic fluid; initial formation of alveoli; moderate venous congestion; primary atelectasis; diapedetic hemorrhages; stromal edema. Hematoxylin–Еosin staining. Magnification 4×12.5 |
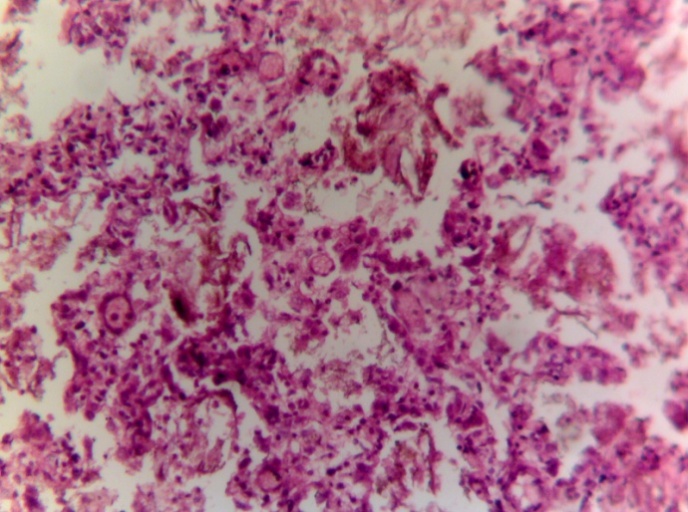 | Figure 4. Formation of respiratory bronchioles and acini; alveoli are open, varying in size and shape; the number of type I alveocytes is increased, appearing hyperchromatic, round, and oval; type II alveocytes are fewer in number, larger in size, and hyperchromatic. Hematoxylin–eosin staining. Magnification A–B, 10*12.5 |
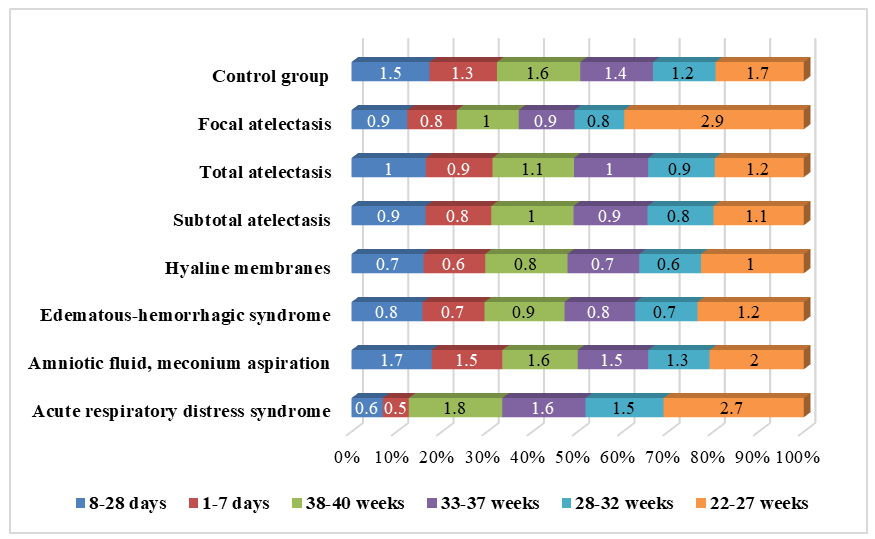
 | Figure 5. Changes in the diameters of type II alveocytes (µm) in various forms of pneumopathies |
 | Figure 6. Respiratory bronchioles and alveoli are open; their lumens contain amniotic fluid and keratinized epithelium. Desquamation of the bronchiolar, alveolar epithelium, and alveocytes is observed, along with moderate venous congestion and interstitial edema. Hematoxylin–eosin staining. Magnification 10*12.5 |
 | Figure 7. Desquamation of the mucosal lining of the respiratory bronchioles and alveoli; presence of serous–hemorrhagic fluid within the lumen; thickening of the interalveolar septa; edema; and infiltration of the stroma with lymphoid cells. Hematoxylin–Eosin staining. Magnification 10×12.5 |
 | Figure 8. Changes in the alveolar lumen activity coefficient in various forms of pneumopathies |
5. Conclusions
- The frequency, distribution, and severity of pathomorphological and morphometric alterations in pneumopathies are strongly dependent on the gestational age of the newborn, the degree of prematurity or maturity, and the level of differentiation of lung tissue. The findings demonstrate that hemodynamic disturbances within the lungs contribute to significant injury of alveocytes and alveolar capillaries, resulting in disruption of the integrity of the alveolo-capillary barrier. This, in turn, promotes transudation of serum proteins, particularly fibrinogen, into the alveolar lumen, which blocks the respiratory surface and impairs gas exchange.Moreover, morphometric analysis revealed that in pneumopathies of varying forms, type I alveocytes undergo a disproportionate enlargement compared to controls, while type II alveocytes also increase but to a lesser extent. Concurrently, thinning of the alveolar stroma and dilation of terminal airways reflect compensatory remodeling processes, whereas thickening of hyaline membranes signifies irreversible damage and altered barrier function.These structural and functional alterations collectively indicate that the pathogenesis of pneumopathies is multifactorial, involving immaturity of lung tissue, surfactant deficiency, circulatory disturbances, and inflammatory–proliferative reactions. In premature infants, the predominance of atelectatic, hyaline membrane, and edematous–hemorrhagic forms underscore the critical role of lung immaturity and surfactant insufficiency, while in later gestational stages, compensatory processes and inflammatory responses contribute more prominently to the disease pattern.Therefore, the study emphasizes that the pathomorphological and morphometric features of pneumopathies not only provide insight into the underlying mechanisms of neonatal respiratory disorders but also highlight their clinical significance. Understanding these changes is essential for improving diagnostic accuracy, guiding therapeutic interventions, and developing preventive strategies to reduce neonatal morbidity and mortality associated with pneumopathies.