-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 3004-3009
doi:10.5923/j.ajmms.20251509.34
Received: Aug. 20, 2025; Accepted: Sep. 15, 2025; Published: Sep. 23, 2025

Predator-Prey Interactions of the Invasive Jellyfish Gonionemus Vertens: Feeding Trials and Ecological Implications
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAkhmedov Dilshod Bakhodirovich
Independent Researcher, Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Akhmedov Dilshod Bakhodirovich, Independent Researcher, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

According to experts from the World Health Organization (WHO), thyroid gland diseases rank second among endocrine pathologies, after diabetes mellitus. More than 665 million people worldwide suffer from thyroid pathologies, and 1.5 billion people are at risk of developing diseases caused by iodine deficiency. In 2008, on the initiative of the European Thyroid Association, World Thyroid Day was established (Won Sang Yoo and Hyun Kyung, 2016) [1].
Keywords: Autoimmune, Thyroid gland, Ultrasound, Humoral, Nodular goiter, Hypothyroidism
Cite this paper: Akhmedov Dilshod Bakhodirovich, Predator-Prey Interactions of the Invasive Jellyfish Gonionemus Vertens: Feeding Trials and Ecological Implications, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 3004-3009. doi: 10.5923/j.ajmms.20251509.34.
1. Introduction
- It has now been proven that structural and morphological features and changes play an important role in the development of most thyroid diseases. The progression of autoimmune pathology in the thyroid gland is accompanied by disorders at the humoral and cellular levels of immunity. The manifestation of the cardiorenal continuum, with subsequent damage to the cardiovascular system and kidneys, indicates the presence of an inflammatory process in thyroid hyperfunction (Gryaznova M.A., Khamnueva L.Yu., 2017) [2].In 1974, the Canadian researcher R. Volpe was the first to substantiate the theory of the autoimmune genesis of diffuse toxic goiter (DTG). According to this theory, a breakdown in the control over the number and function of autoreactive cells is observed in this pathology due to a defect in organ-specific T-suppressor cells.The prognosis for nodular thyroid formations depends on the stage of tumor development identified during the initial examination. Therefore, the issue of early diagnosis of focal thyroid formations is highly relevant (Campanozzi A. et al., 2019) [3,4].The evaluation of the echogenicity and echostructure of the thyroid parenchyma is also considered one of the important issues. In thyroid hyperplasia, echogenicity decreases due to increased tissue hydrophilicity, and a medium-to-large granular structure is observed (Barrea L. et al., 2021) [5].Endocrinological diseases, including thyroid pathologies, are widespread throughout the world, leading to complications, decreased quality of life, and reduced work capacity in patients. This has evolved into not only a medical but also a socio-economic problem. The ongoing research in this medical field shows that its relevance has not diminished [8,9].The purpose of the study was to evaluate the role of thyroid ultrasound examination in the early diagnosis of thyroid diseases by analyzing the results of this examination [12].
2. Materials and Methods
- A total of 139 adult patients diagnosed with thyroid diseases were included in the study, and all of them underwent an ultrasound examination (UE). Of these, 16 (11.51±2.71%) were men and 123 (88.49±2.71%) were women. Women were found to be 7.69 times more frequent than men. The age distribution of the patients was as follows: 20-29 years - 23.02±3.54% (n=32); 30-39 years - 28.78±3.84% (n=40); 40-49 years - 22.30±3.53% (n=31); 50-59 years - 16.55±3.15% (n=23); 60 years and older - 9.35±2.47% (n=13).The patients were also categorized based on the duration of their illness. It was found that 40.29±4.16% (n=56) of patients had a disease duration of 1-2 years, 24.46±3.65% (n=34) had a duration of 3-4 years, and 12.95±2.85% (n=18) had a duration of 5 years or more. A concerning 20.86±3.45% (n=29) were newly diagnosed upon first consultation for this condition, and 2 patients (1.44±1.01%) had a congenital thyroid pathology. The leading duration of illness was 1-2 years (40.29±4.16%). The high percentage of new diagnoses (20.86±3.45%) was also interpreted as a worrying trend.Based on the ultrasound conclusions for thyroid diseases, three pathologies were studied. It was found that nodular goiter was present in 44.61±4.22% (n=62) of cases, hypothyroidism in 33.09±3.99% (n=46) of cases, and diffuse toxic goiter (DTG) in 22.30±3.53% (n=31) of cases among the patients who underwent UE.The final diagnoses of thyroid diseases (nodular goiter, diffuse toxic goiter, hypothyroidism) were based on the 11th edition of the International Classification of Diseases (ICD-11, 2022). This classification is based on clinical, instrumental, and laboratory indicators. Although this classification was recommended for use starting February 18, 2022, the transition period is set from 2022 to 2027. Therefore, the main diagnoses for the patients were made based on the old classification (ICD-10, 2007).The study was conducted in accordance with the World Medical Association's Declaration of Helsinki regarding the inclusion of human subjects in medical research (Helsinki, 1964, last amendment Fortaleza, Brazil, 2013).In addition to clinical and laboratory diagnostic methods for thyroid diseases, instrumental methods also play a significant role. In particular, ultrasound examination (UE) is crucial for the diagnosis of these diseases and has great diagnostic value. Today, elastography is an innovative technology in the ultrasound diagnosis of thyroid diseases, allowing for a non-invasive assessment of the density and elasticity of tissues and volumetric formations in the organ. The use of elastography in studying patients with nodular thyroid pathology increases the accuracy and specificity of the ultrasound examination.Ultrasound examinations (UE) for the patients included in the study were performed using a SonoScape S22 ultrasound scanner manufactured in China. This device is equipped with a special Thyroid ElastoScan function, which allows for a qualitative analysis of the thyroid gland parenchyma and nodular formations, as well as a quantitative evaluation of the elasticity contrast index. Elastography allowed for the identification of the following information in patients: the state of lymph nodes located near the thyroid gland; its morphological structure; its volume; the dimensions of both its lobes; and the structure of the isthmus.The data collected during the study were statistically processed using both parametric and non-parametric analysis methods from traditional variational statistics with the help of the "Excel" software.
3. Results and Discussion
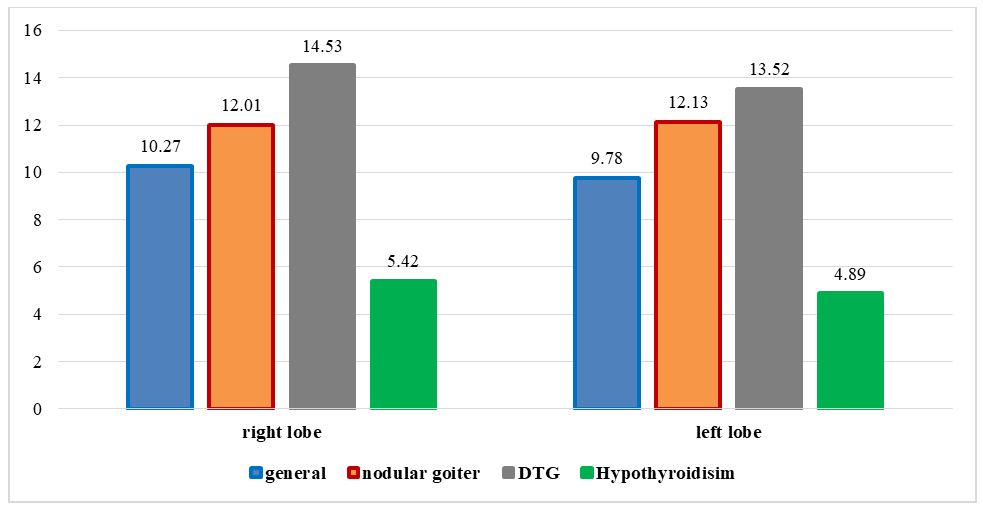
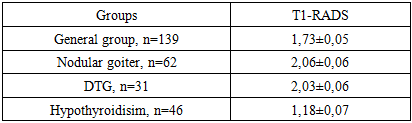
- The study presented the UE anatomy and characteristics of the thyroid gland (TG). It was found that the TG was in its typical location—in the lower part of the neck, anterior to the thyroid cartilage and trachea. In all patients, the gland was found to consist of two parts, the right and left lobes, which are connected by the isthmus. It's easy to identify the TG with UE because the organ is separated from the outside world only by the skin and neck muscles, which are the sternohyoid, sternothyroid, and sternocleidomastoid muscles.In healthy individuals, the TG has a homogeneous echogenicity, and the parenchyma is hyperechoic, making it appear brighter than the surrounding muscles on the ultrasound. All borders of the TG were clearly distinguishable, and no focal pathological changes were detected in the parenchyma. No pathological or aberrant location of the organ was found when viewed in both transverse and longitudinal projections.In addition to studying the UE parameters in the overall patient group, the parameters were also analyzed comparatively among different nosological units of thyroid diseases: nodular goiter, DTG, and hypothyroidism. The results for the TG parameters among the nosological units are presented in Table 1.
|
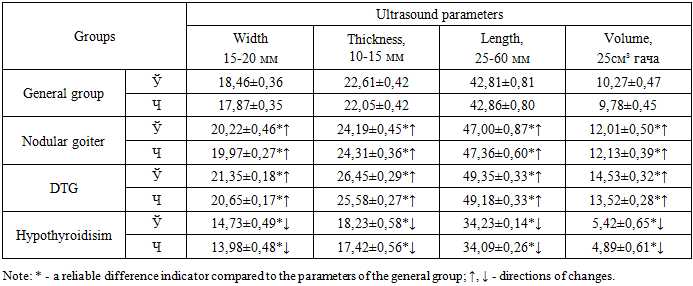
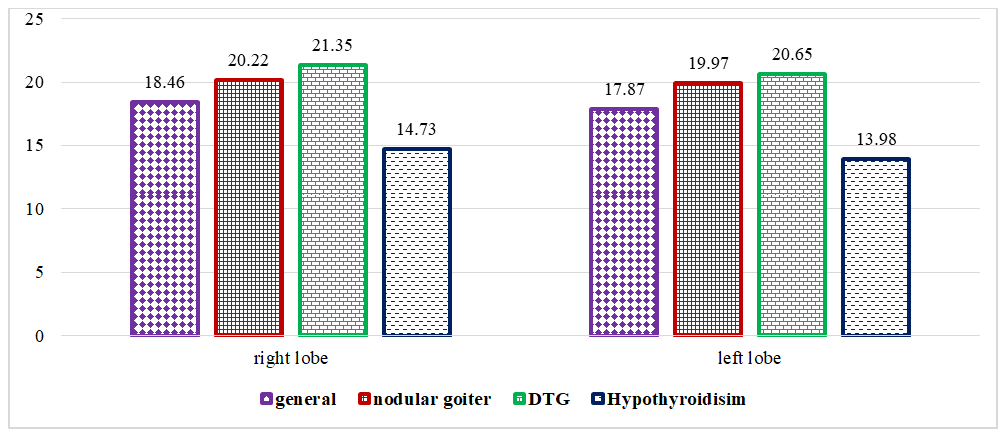 | Figure 1. Comparative Indicators of Thyroid Gland Width (in mm) as an Ultrasound Parameter in Patients with Diagnosed Thyroid Diseases |
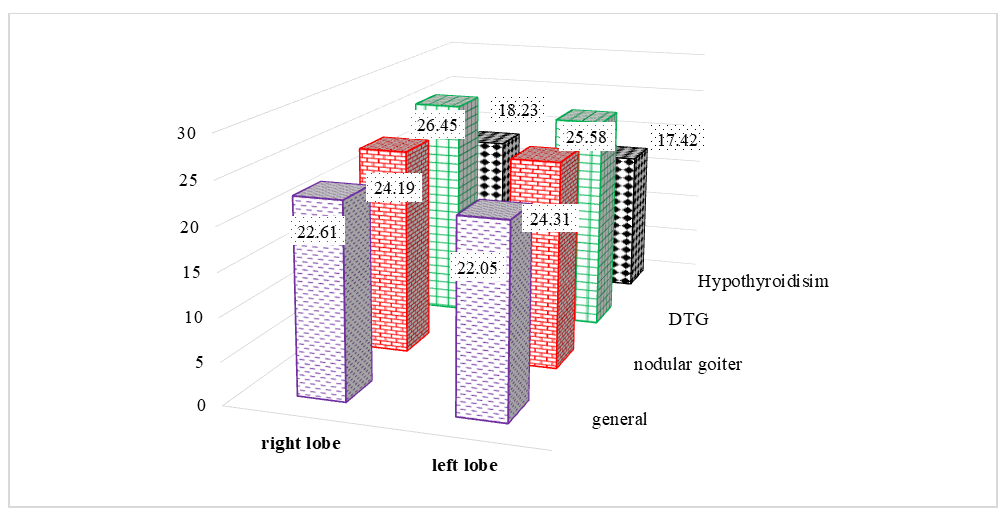 | Figure 2. Comparative Indicators of Thyroid Gland Thickness (in mm) as an Ultrasound Parameter in Patients with Diagnosed Thyroid Diseases |
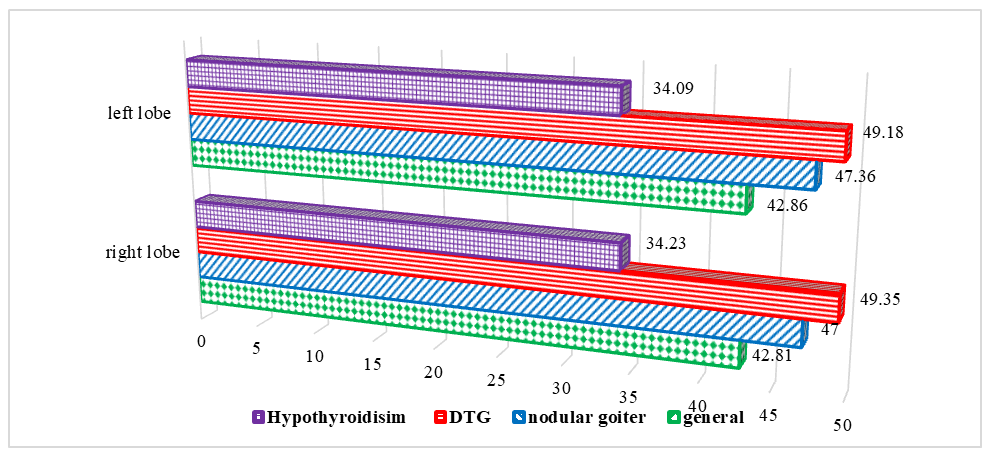 | Figure 3. Comparative Indicators of Thyroid Gland Length (in mm) as an Ultrasound Parameter in Patients with Diagnosed Thyroid Diseases |
 | Figure 4. Comparative Indicators of Thyroid Gland Volume (in cm³) Determined by Ultrasound in Patients with Thyroid Diseases |
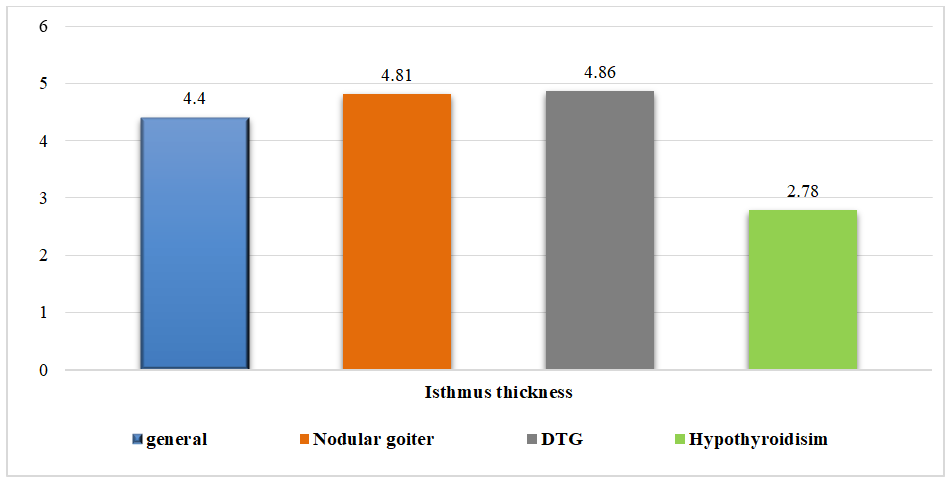 | Figure 5. Measurements of the Thyroid Gland Isthmus (in mm) Determined by Ultrasound in Patients with Thyroid Diseases |
|
4. Conclusions
- 1. The trend and intensity of changes in the width, thickness, length, and volume of the thyroid gland remained consistent across the nosological units (nodular goiter, DTG, hypothyroidism). The ratio of differences in the thickness of the organ's isthmus was particularly significant. This highlights that these ultrasound parameters are important indicators for interpreting the organ's ultrasound anatomy. When diagnosing thyroid pathologies with ultrasound, special attention should be paid to determining and evaluating the thickness of the gland, without neglecting the diagnostic value of its width, length, and volume.2. Two computer programs were developed to assess the degree of structural changes occurring in the organ and the level of utilization of elastographic indicators. These programs use the elastographic parameters of the thyroid gland to create a basis for the early diagnosis and prognosis of the outcome of its diseases.