-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 2999-3003
doi:10.5923/j.ajmms.20251509.33
Received: Aug. 17, 2025; Accepted: Sep. 10, 2025; Published: Sep. 23, 2025

Optimizing Gastric Resection in Bariatric Surgery: Clinical and Pathomorphological Study
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLFarrukh Saidaliyevich Akbarov1, Nosirjon Juraevich Mahkamov2
1PhD, Andijan State Medical Institute, Andijan, Uzbekistan
2Associate Professor, Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Farrukh Saidaliyevich Akbarov, PhD, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Optimizing gastric resection in bariatric surgery requires a comprehensive evaluation of patients’ clinical parameters and pathomorphological features. This study analyzed patients who underwent gastric resection via bariatric techniques, with a focus on age and sex distribution as well as the prevalence of comorbidities. Clinical characteristics, including obesity severity and gastrointestinal symptoms, were assessed. Pathomorphological examination evaluated morphological alterations in the resected gastric tissues, including structural changes in the mucosal and parenchymal layers. The findings demonstrated a strong association between age, sex, and comorbid factors with both the morphological alterations of gastric tissue and clinical parameters. These results confirm the importance of integrating clinical and pathomorphological analysis to individualize surgical strategies and optimize resection techniques in bariatric surgery.
Keywords: Bariatric surgery, Gastric resection, Clinical parameters, Pathomorphological analysis, Age groups, Comorbidities
Cite this paper: Farrukh Saidaliyevich Akbarov, Nosirjon Juraevich Mahkamov, Optimizing Gastric Resection in Bariatric Surgery: Clinical and Pathomorphological Study, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 2999-3003. doi: 10.5923/j.ajmms.20251509.33.
Article Outline
1. Introduction
- Bariatric surgery has become one of the most effective treatment modalities for obesity in recent decades and is widely applied in global clinical practice [1,2]. The influence of age on surgical outcomes has been reported with varying conclusions: while some studies suggest a higher complication rate in younger patients, others confirm that bariatric surgery can be both safe and effective in older individuals [3,4]. Gender factors are also significant, with certain studies showing greater weight loss and fewer complications in women compared to men [5,6], whereas other investigations have found no substantial differences between sexes [7].Comorbidities—particularly type 2 diabetes mellitus, hypertension, and obstructive sleep apnea—play a crucial role in determining postoperative outcomes [8,9]. In many patients, these conditions improve or go into remission after surgery; however, results may vary depending on age and gender [10,11]. Pathomorphological studies of gastric tissue enable the evaluation of morphological changes in relation to age, gender, and comorbidities, thus providing opportunities to individualize surgical techniques and optimize resection strategies [12].
2. Purpose of the Study
- The aim of this study is to analyze the clinical parameters and pathomorphological changes in patients undergoing gastric resection via bariatric surgery, considering the influence of age, sex, and comorbidities, in order to identify opportunities for optimizing and individualizing surgical strategies.
3. Materials and Methods
- The study material consisted of 183 cases of gastric tissue and its mucosal layer, obtained from patients who underwent bariatric gastric resection and were subjected to biopsy at the Republican Center of Pathological Anatomy between 2022 and 2024. Clinical and morphopathological data for these cases were verified and included in the analysis.The following methods were applied to conduct the study:- Collection of clinical information including patient age, sex, and comorbidities;- Pathomorphological examination of the resected gastric specimens obtained via bariatric surgery;- Microscopic evaluation of morphological changes in the gastric mucosa and parenchymal layers;- Analysis of the correlations between clinical and pathomorphological parameters;These methods allowed for the integration of clinical and pathomorphological analyses to identify opportunities for individualizing and optimizing bariatric gastric resection strategies.
4. Results and Discussion
- The analysis of the 183 patients included in the study revealed that 22 patients (12.0%) were male, while 161 patients (88.0%) were female. These findings clearly demonstrate the predominance of female patients seeking bariatric surgery.A more detailed examination showed that females constitute the majority, representing 88% of the total cases. This indicates a significantly higher engagement of women in bariatric procedures. Male patients accounted for only 12%, reflecting a marked gender disparity, with females being nearly seven times more prevalent than males in this cohort.The observed predominance of female patients may be associated with clinical manifestations of obesity, aesthetic concerns, or reproductive factors that influence the decision to undergo bariatric surgery. Conversely, the lower number of male patients may reflect reduced willingness or lower clinical referral rates among men.In conclusion, female patients represent the main proportion of individuals undergoing bariatric surgery. These results emphasize the importance of considering gender as a significant factor in clinical studies and surgical planning. The data presented in the table provide a clear visualization of the demographic distribution (Figure 1).
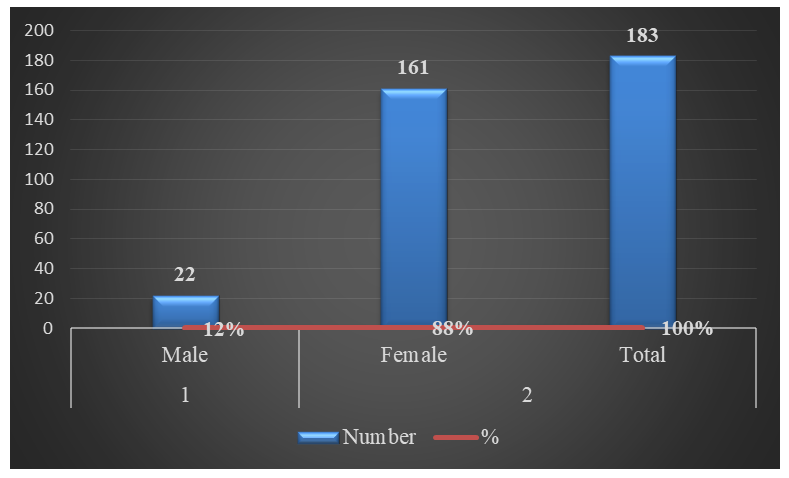 | Figure 1. Distribution of patients by sex, expressed as percentages |
 | Figure 2 |
 | Figure 3 |
|
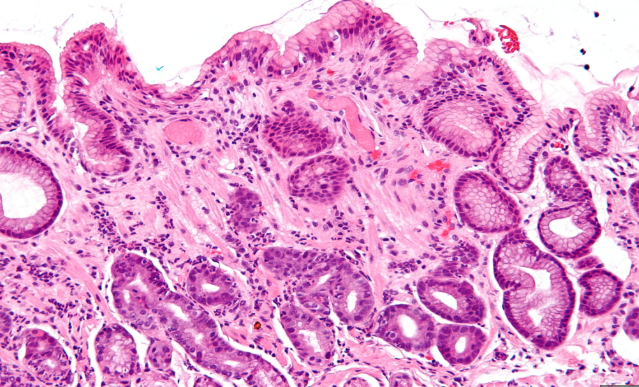 | Picture 1. Microscopic changes of the gastric mucosa (hyperplasia and inflammation). Gastric mucosal hyperplasia in the antral region (1). Signs of inflammation and regenerative epithelial changes (2). H&E staining. Magnification 10×400 |
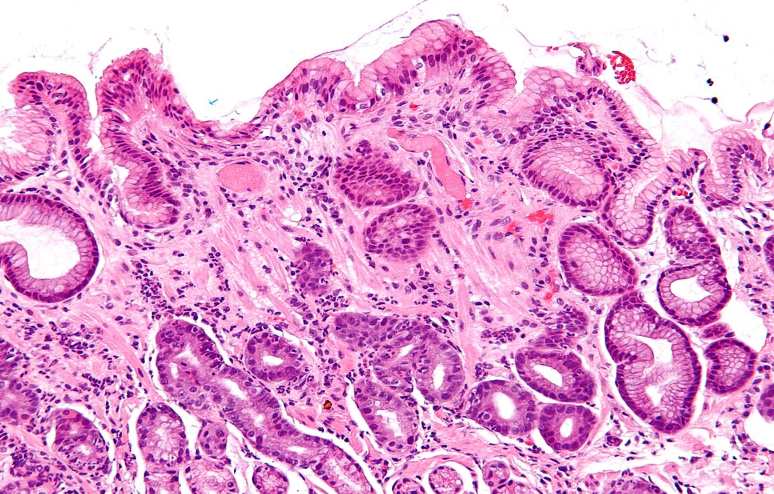 | Picture 2. Morphological changes in the gastric tissue Thickening of the gastric wall (1). Congestion of capillaries and venous branches with foci of microcirculatory disturbances (2). H&E staining. Magnification 10×400 |
5. Conclusions
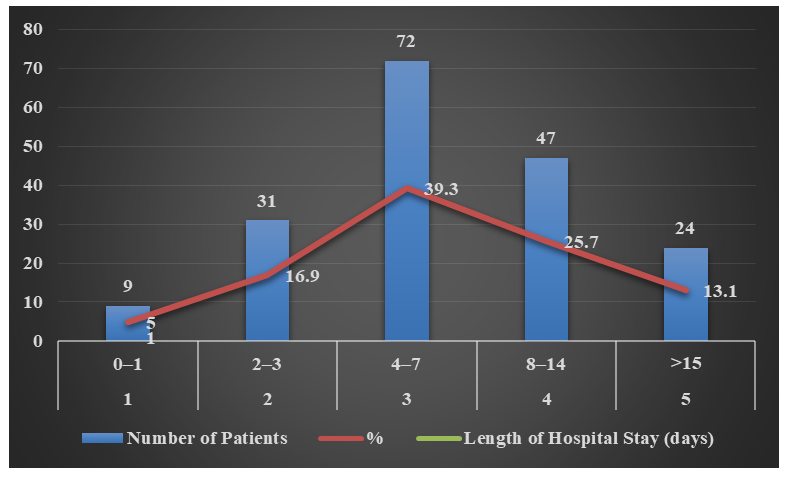
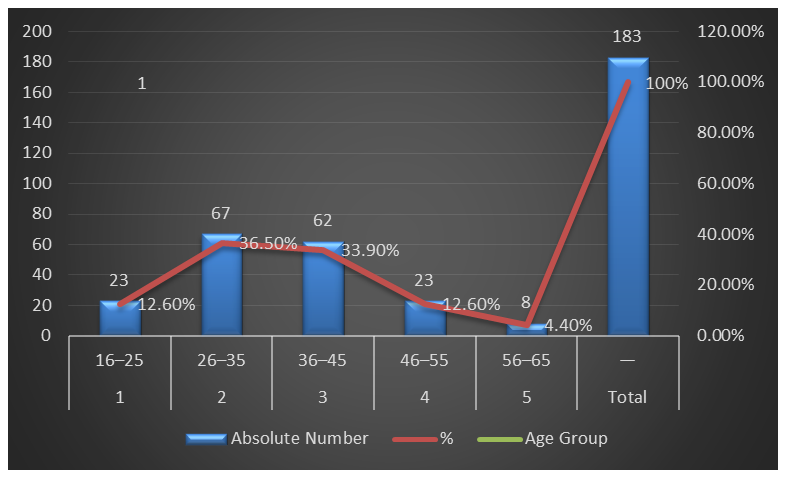
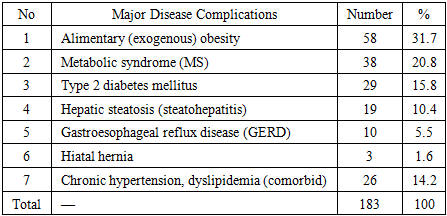
- The results of the study indicate that the clinical and pathomorphological data of 183 patients undergoing bariatric gastric resection were comprehensively analyzed in terms of age, sex, primary diseases, and postoperative hospital stay. Regarding age groups, the majority of patients were in the 26–35 and 36–45 age ranges, reflecting the higher prevalence of obesity and metabolic syndrome among middle-aged adults. Sex analysis revealed a predominance of female patients, who accounted for 88% of the cohort, highlighting the greater participation of women in bariatric surgery, while males represented only 12%, indicating notable gender disparities and differences in clinical decision-making.Analysis of primary comorbidities showed that alimentary obesity and metabolic syndrome were the most common conditions, representing 31.7% and 20.8% of cases, respectively. Additionally, type 2 diabetes mellitus and hepatic steatosis were frequently associated with obesity-related cases. These findings underscore the importance of comprehensive evaluation of clinical and pathomorphological changes in bariatric surgery and suggest effective approaches for managing obesity and metabolic complications.Regarding postoperative hospital stay, a simple mathematical model estimated the expected duration at 6.6 days. This finding is crucial for clinical planning and optimizing resource allocation. The observed distribution of hospitalization periods, when considered alongside age groups and comorbidities, can guide the development of individualized surgical strategies.Furthermore, pathomorphological analysis revealed microscopic changes in the gastric mucosa, including hyperplasia, wall thickening, vascular alterations, and focal intestinal metaplasia in patients with long-standing GERD. These results confirm the clinical significance of gastric tissue alterations and provide insights into the prolonged impact of obesity and metabolic stress.Overall, the study demonstrates that incorporating clinical and pathomorphological parameters associated with age, sex, and comorbidities can provide a scientific basis for individualizing and optimizing bariatric surgical strategies, ultimately improving patient outcomes and treatment planning.