-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 2987-2995
doi:10.5923/j.ajmms.20251509.31
Received: Aug. 13, 2025; Accepted: Sep. 11, 2025; Published: Sep. 23, 2025

Association Between CD34 and P53 Marker Expression and Recurrence of Non-Muscle-Invasive Bladder Cancer
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAllamova Shakhlo Maksudovna1, Boyko Elena Vladimirovna2
1PhD Student, Republican Specialized Scientific-Practical Medical Center of Oncology and Radiology, Ministry of Health of Uzbekistan, Tashkent, Uzbekistan
2DSc, Professor, Head of Oncourology Department, Republican Specialized Scientific-Practical Medical Center of Oncology and Radiology, Ministry of Health of Uzbekistan, Tashkent, Uzbekistan
Correspondence to: Allamova Shakhlo Maksudovna, PhD Student, Republican Specialized Scientific-Practical Medical Center of Oncology and Radiology, Ministry of Health of Uzbekistan, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Relevance: Urothelial carcinoma (UC) of the bladder is one of the leading causes of cancer-related morbidity and mortality worldwide. Accurate prediction of recurrence and progression risk necessitates the identification of reliable biomarkers. Among these, microvascular density (MVD) and p53 have emerged as key indicators, given their critical roles in tumor angiogenesis and cell cycle regulation. Objective: To evaluate the prognostic significance of microvascular density (MVD) and p53 expression in predicting recurrence in patients with non-muscle-invasive bladder cancer (NMIBC). Materials and Methods: The study included 155 patients diagnosed with non-muscle-invasive bladder cancer (NMIBC), all of whom underwent immunohistochemical staining for CD34 and p53 markers. Microvascular density (MVD) was assessed in tumor hot spots using the Weidner method. p53 expression was quantified as the percentage of positively stained tumor cell nuclei. Statistical analysis was performed using the t-test and chi-square (χ²) test with SPSS software, version 28.0. A p-value of less than 0.05 was considered statistically significant. Results: High microvascular density (MVD), defined as ≥10 vessels per high-power field, was identified in 40% of patients. p53 expression was observed in 62% of cases, with high expression levels (>50% of tumor cells) significantly associated with elevated MVD (p < 0.001). Statistical analysis revealed that both high MVD and elevated p53 expression were significantly associated with an increased risk of tumor recurrence and progression (relative risk: 2.3; 95% confidence interval: 1.6–3.2). Conclusions: Microvascular density (MVD) and p53 expression are significant prognostic factors for recurrence in non-muscle-invasive bladder cancer (NMIBC). Incorporating these markers into clinical assessment may enhance risk stratification and support a more personalised approach to treatment.
Keywords: Non-muscle-invasive bladder cancer, Angiogenesis, Microvascular density, p53, CD34, Prognostic markers
Cite this paper: Allamova Shakhlo Maksudovna, Boyko Elena Vladimirovna, Association Between CD34 and P53 Marker Expression and Recurrence of Non-Muscle-Invasive Bladder Cancer, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 2987-2995. doi: 10.5923/j.ajmms.20251509.31.
1. Introduction
- According to GLOBOCAN data, bladder cancer ranks as the ninth most common malignancy worldwide. In 2022, approximately 614,298 new cases and 220,596 deaths were reported globally due to this disease [1,9]. Approximately 75% of urothelial carcinoma (UC) cases are diagnosed at a low grade and classified as non-muscle-invasive bladder cancer (NMIBC). [2,30]. Low-grade tumors rarely progress to invasive disease (1% to 45%), but they frequently recur (31–78%) within five years of follow-up, generally associated with a favourable prognosis. In contrast, high-grade papillary tumors have a greater potential to progress to muscle-invasive bladder cancer (MIBC) [2,10]. The European Association of Urology (EAU) guidelines employ a similar risk stratification system; however, unlike the American Urological Association (AUA) guidelines, the EAU model includes age over 70 as an independent risk factor and introduces a "very high-risk" category. This category encompasses patients with high-grade disease and/or carcinoma in situ (CIS), along with additional risk factors such as age over 70, multifocal papillary tumours, and tumour size greater than 3 cm [4]. In low-risk non-muscle-invasive bladder cancer (NMIBC), despite the very low rates of progression, the risk of recurrence remains substantial—approximately 40–50% within five years [1,16]. In high-risk disease, although up to 80% of patients initially respond to intravesical BCG therapy, the overall rate of recurrence or progression of high-grade bladder cancer remains around 50% [5,8]. In T1-stage disease, particularly when the tumor is detected during repeat resection, the progression rate can reach as high as 80% [16]. Some studies suggest that papillary and non-papillary urothelial carcinomas may follow distinct molecular pathways, which could account for their physiological differences. [24]. Angiogenesis—the process of forming new blood vessels—plays a key role in tumor progression by promoting growth and metastasis. Microvascular density (MVD), assessed using the CD34 marker, serves as an indicator of angiogenic activity and tumor prognosis [29]. High MVD is associated with more aggressive tumor behaviour and an increased risk of recurrence.Angiogenesis—the formation of new capillaries from pre-existing blood vessels—is essential for tumor growth and metastasis. It is a complex process influenced by numerous factors and involves signaling pathways that regulate various aspects of cellular biology. In recent years, increasing attention has been given to the role of angiogenesis in malignant bladder tumors. Most patients with bladder cancer initially present with low-grade, mucosa-confined tumors that are prone to recurrence after transurethral resection. Up to one-third of these non-muscle-invasive bladder cancers (NMIBC) may progress to more invasive or higher-grade tumors. Angiogenesis represents one of the critical steps in this progression, and our understanding of its role in bladder cancer continues to evolve.Microvascular density (MVD) is used to assess angiogenesis by quantifying the number of blood vessels per unit area or per high-power field. As a marker of tumor angiogenesis, MVD has been proposed for identifying patients at high risk of recurrence [2]. Angiogenesis quantification can be performed using immunohistochemical staining with antibodies specific to vascular endothelial cells. CD34, a transmembrane glycoprotein, is an antigen of hematopoietic progenitor cells that is also expressed in vascular endothelial cells. It serves as a sensitive marker of endothelial differentiation, staining endothelial cells in tumors more intensely than in normal tissue [28].Another important marker, p53, is a key regulator of the cell cycle and apoptosis. Mutations in the p53 gene are observed in 50–60% of urothelial carcinoma cases, making it a significant prognostic factor. Increased p53 expression is associated with genetic instability and disease progression [20].Despite a substantial body of evidence, the role of p53 as an independent prognostic marker for recurrence remains a subject of debate, largely due to variability in research methodologies and differing interpretations of results. The present study aims to clarify the prognostic value of p53 expression in the context of NMIBC recurrence, as well as to assess its correlation with microvascular density, depth of invasion, and tumor grade.
2. Materials and Methods
- Study DesignThe study was conducted as both a retrospective and prospective analysis in the Department of Urology at the Republican Specialized Scientific and Practical Medical Center of Oncology and Radiology of Uzbekistan, covering the period from 2020 to 2024. The study protocol was approved by the institution's ethics committee.Inclusion and Exclusion CriteriaThe study included 155 patients with histologically confirmed non-muscle-invasive bladder cancer (NMIBC) following transurethral resection of the bladder tumor (TURBT). Cases were excluded if there was significant inflammation, insufficient biopsy material, or a lack of follow-up data.Immunohistochemical AnalysisAntibodies against CD34 and p53 were used for immunohistochemical staining. Microvessels were counted in three "hot spots" at 400× magnification across ten high-power fields. p53 expression was evaluated semi-quantitatively using the following scale: 0 (no staining), 1+ (<20%), 2+ (20–50%), and 3+ (>50%). Tumors with >20% positively stained cells were considered p53-positive.Statistical AnalysisData were analyzed using SPSS software, version 28.0. Group comparisons were performed using the t-test, chi-square (χ²) test, and ANOVA. Relative risk (RR) was calculated with a 95% confidence interval (CI).Interpretation of Resultsp53 is a nuclear marker, and tumor “hot spots,” often corresponding to the invasive margin, were selected for analysis. A total of 500 tumor cells were counted, and the number of p53-positive cells was recorded individually. Expression was then evaluated semi-quantitatively as follows: 0 – no expression; 1+ – <20% of tumor cells positive; 2+ – 20–50% positive cells; 3+ – >50% positive cells. Only tumors with >20% positively stained cells were considered p53-positive. Expression levels below 20% were classified as negative.CD34 expression was assessed in tumor "hot spots." Branching structures were counted as a single vessel. A single microvessel was defined as any brown, immunostained endothelial cell structure clearly separated from adjacent microvessels, tumor cells, and other connective tissue components. The number of vessels was counted across ten consecutive high-power fields at 400× magnification, corresponding to an area of 0.152 mm².Since CD34 expression, represented as intratumoral microvascular density (MVD), is a quantitative variable, and p53 expression and tumor grade are categorical variables, analysis of variance (ANOVA) was performed to determine whether MVD differed significantly between groups stratified by p53 status and tumor grade. Homogeneity of variances was tested prior to ANOVA. Post hoc comparisons were conducted using the Least Significant Difference (LSD) method. To assess correlations between categorical variables, the chi-square (χ²) test was applied using SPSS version 28.0.
3. Results
- Clinical CharacteristicsThe mean age of the patients was 65.1 ± 15.0 years. Males accounted for 83.9% of the study population. The majority of cases (64.5%) occurred in patients over 50 years of age (Figure 1). Most tumors (69%) were well- or moderately differentiated (G1 and G2), while 31% were poorly differentiated (G3). Lamina propria invasion was observed in 58% of patients, and muscular layer invasion was identified in 33%.
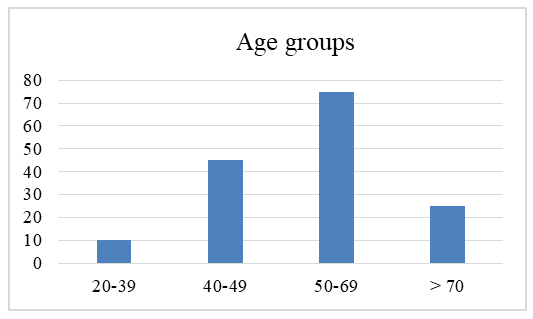 | Figure 1. Age distribution of the patient groups |
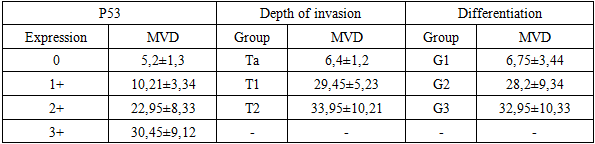
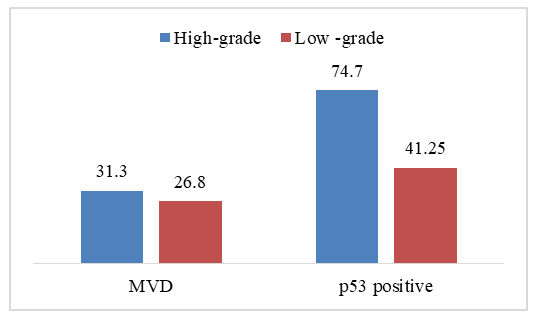 | Figure 2. Relationship between mean microvascular density (MVD), p53 gene expression, and tumor differentiation |
|
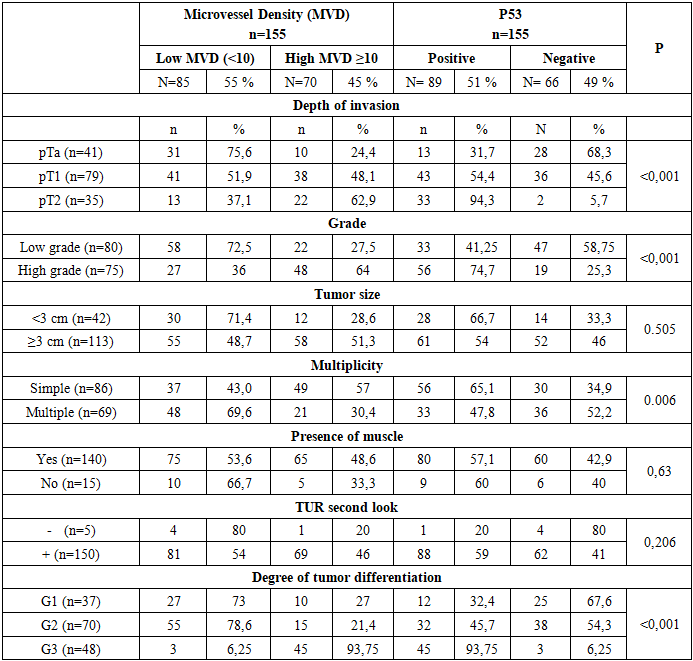
 | Figure 3. Association of p53 Protein Expression with Tumor Invasion Depth and Degree of Differentiation |
|
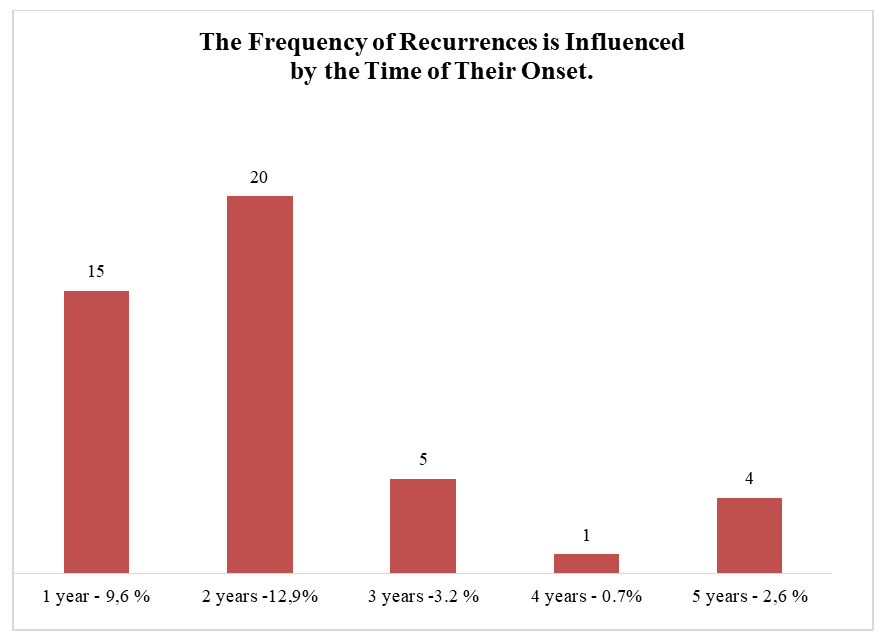 | Figure 4. Recurrence rate of non-muscle-invasive bladder cancer following TUR |
|
4. Discussion
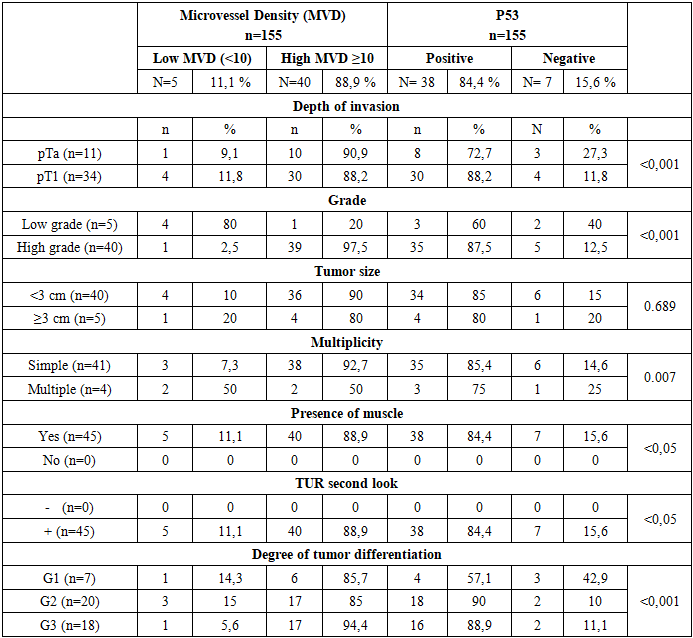
- Bladder cancer is the most common malignancy of the urinary tract and ranks tenth among all cancers worldwide. According to GLOBOCAN data, approximately 614,298 new cases are diagnosed annually, with the highest incidence observed in developed countries characterized by urbanized populations and aging demographics.At initial diagnosis, 75–80% of bladder tumors are classified as non-muscle-invasive bladder cancer (NMIBC), which are associated with a high recurrence rate and a significant risk of progression within the first few years of follow-up [1,8]. p53 expression was detected in 51% of cases, of which 20.8% exhibited low expression and 79.2% showed high expression. In our study, no significant correlation was found between p53 expression and either tumor stage or histological grade.Intratumoral microvessel density (MVD) was found to be significantly correlated with both tumor stage and grade. Similar associations were previously reported by Kern. Independent studies by Weidner and Vermeulen also identified increased MVD as an independent risk factor for metastasis. In our study, a 66.7% correlation was observed between the absence of p53 expression and high MVD. Additionally, there was a statistically significant association between high p53 expression and CD34 expression (P = 0.001; Table 2, Figure 1). Elevated p53 levels were associated with increased MVD, which, in turn, was linked to poor prognosis. The correlation between p53 expression and MVD was statistically significant (P = 0.0006), with a correlation coefficient of 0.31.The assessment of parameters related to tumor angiogenesis has provided valuable prognostic information across various tumor types. Alterations in the p53 gene have been shown to shift the local balance between pro- and anti-angiogenic factors toward a pro-angiogenic state. A significant correlation was also observed between p53 expression and microvessel density (MVD).Despite the trends identified in this study, larger-scale investigations focusing on stage II and III disease are necessary to validate our findings. In our analysis, p53 and CD34 were not independent prognostic factors for non-muscle-invasive bladder cancer. However, when evaluated together, they serve as reliable predictors of disease behavior and may assist in identifying patients at risk for progression, metastasis, or recurrence. Furthermore, these markers could contribute to assessing treatment response, thereby potentially improving both recurrence-free and overall survival.Angiogenesis is one of the hallmarks of carcinogenesis, playing a critical role in tumor progression and metastasis. Global incidence data on urothelial carcinoma demonstrate a predominance in males, a finding corroborated by studies conducted by Gupta and Biswas [7]. Our current study yielded similar results, with males accounting for 86% of cases and a male-to-female ratio of 6.1:1. The majority of urothelial carcinoma cases occur in patients over the age of 50, while it is exceedingly rare in children and young adults. Gupta et al. reported a mean age at diagnosis of 60 ± 4.4 years, and Biswas et al. found the highest incidence in individuals over 60 years of age. These findings are consistent with our results, which showed that 74% of cases occurred in patients older than 50 [7].The most common histological subtype of urothelial carcinoma in the present study was invasive papillary urothelial carcinoma (25 out of 50 cases), followed by invasive urothelial carcinoma (13 out of 50 cases). Only two cases were classified as non-invasive papillary urothelial carcinoma, which is consistent with the findings of Quinten and Jhaveri. Low-grade tumors were relatively rare, accounting for only 10% of cases, whereas high-grade tumors comprised 90%. In a 2018 study by Haque et al., 72% of cases were reported as high-grade and 28% as low-grade.While tumor grade and stage remain important prognostic indicators, additional insights can be gained through the evaluation of biological markers such as microvessel density (MVD). In the present study, MVD was assessed using two markers: p53 and CD34. The mean CD34-MVD value in high-grade tumors was slightly higher than in low-grade tumors. These findings highlight the significance of angiogenesis as a key process contributing to tumor regrowth. A statistically significant association (p<0.05) supports MVD as a promising prognostic marker for recurrence.Goddard et al. studied 180 cases and found a significant correlation between microvessel density (MVD), tumor stage, and progression. However, the mean MVD was not statistically significantly associated with high-grade tumors [13].The conflicting results among different studies may be attributed to variations in staining techniques, antibody selection, antigen detection methods, tissue characteristics, or microvessel counting approaches.In 84.4% of patients with recurrence, positive p53 expression was detected, indicating a strong association between p53 mutation and an increased risk of tumor regrowth. In contrast, recurrence was less common (15.6%) among patients with negative p53 expression. These findings support the role of p53 as a significant indicator of poor prognosis.The level of microvessel density (MVD) was highest among patients with recurrent pT1 tumors (88.2%), significantly exceeding the corresponding rate in patients with superficial pTa tumors (90.9% with high MVD). Positive p53 expression was also more frequently observed in patients with recurrent pT1 tumors (88.2%) compared to those with superficial tumors (72.7%). These findings highlight the importance of invasion depth, in conjunction with the biological characteristics of the tumor, in predicting recurrence.Patients with high-grade tumors exhibited high microvessel density (MVD) in 97.5% of cases and positive p53 gene expression in 87.5%, both of which were significantly associated with tumor recurrence. In contrast, among patients with low-grade tumors, recurrences were less frequently associated with high MVD (20%) and p53 expression (60%). These findings confirm that tumor aggressiveness directly influences the likelihood of recurrence (p<0.001).Tumor size (less than 3 cm or greater than 3 cm) did not show a significant association with recurrence (p = 0.689). However, patients with smaller tumors (<3 cm) more frequently exhibited high microvessel density (90%) and positive p53 expression (85%). This underscores that, in predicting recurrence, not only tumor size but also its molecular characteristics play a crucial role.In patients with multiple tumors, recurrences were often associated with low microvessel density (50%) and negative p53 expression (25%). In contrast, patients with solitary tumors predominantly exhibited high MVD (92.7%) and positive p53 expression in 85.4% of cases. This suggests that multiple tumors may possess distinct mechanisms of recurrence that differ from those of solitary tumors (p = 0.007).All patients with recurrences who underwent repeat transurethral resection (TUR second look) demonstrated high microvessel density (88.9%) and positive p53 expression (84.4%). This emphasizes the importance of dynamic monitoring and periodic assessment of molecular markers for accurate prediction of tumor recurrence.Patients with poorly differentiated tumors (G3) exhibited high microvessel density (MVD) in 94.4% of cases and positive p53 expression in 88.9% of cases in the context of recurrence. In contrast, patients with well-differentiated tumors (G1) demonstrated lower rates—85.7% for MVD and 57.1% for p53 expression. These findings indicate that the degree of tumor differentiation plays a significant role in predicting the risk of tumor regrowth (p<0.001).
5. Conclusions
- The results of the study confirm that high microvessel density (MVD) and positive p53 expression are associated with bladder tumor recurrence. These parameters may be utilized for risk assessment of recurrence and for planning further treatment strategies.Significant differences between groups in terms of MVD levels and p53 expression highlight their effectiveness as prognostic markers for dynamic patient monitoring and the individualization of therapy.