-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 2964-2966
doi:10.5923/j.ajmms.20251509.25
Received: Jul. 24, 2025; Accepted: Aug. 16, 2025; Published: Sep. 20, 2025

Algorithms for the Use of Glucocorticosteroid Therapy in Rhabdomyolysis
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLNurmukhamedov Khurshid Dilshadovich1, Bazarova Sayyora Abdubasitovna2
1Military Medical Academy, Uzbekistan, Tashkent
2Central Military Hospital, Uzbekistan, Tashkent
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Tubulointerstitial nephritis of rhabdomyolysis etiology that develops after physical exertion causes inflammation and swelling in the renal glomeruli and interstitium, leading to acute kidney injury. Acute kidney injury (AKI) is one of the main factors leading to negative outcomes for patients, and the rational use of glucocorticosteroid (GCS) drugs in such patients leads to early recovery from the disease and prevention of complications that may arise as a result of the disease.
Keywords: Rhabdomyolysis, Acute kidney injury, Tubulointerstitial nephritis, Glucocorticosteroid drugs
Cite this paper: Nurmukhamedov Khurshid Dilshadovich, Bazarova Sayyora Abdubasitovna, Algorithms for the Use of Glucocorticosteroid Therapy in Rhabdomyolysis, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 2964-2966. doi: 10.5923/j.ajmms.20251509.25.
1. Introduction
- During military service, military personnel have to perform physical loads, and sometimes intense physical loads. Due to the fact that the initial physical condition and level of physical fitness of military personnel of different contingents differ significantly, some of them may experience muscle damage as a result of these loads, which in turn causes the development of acute kidney injury manifested by clinical signs characteristic of rhabdomyolysis.Patients suspected of having rhabdomyolysis are hospitalized and emergency treatment measures are applied in the intensive care or resuscitation department. The scheme-based application of drugs to patients includes the following, depending on the severity and stage of the disease:• Prevention of acute kidney injury - diuretics, hormonal drugs, ACE inhibitors, sodium bicarbonate preparations are administered intravenously to prevent myoglobin cylindrical deposits from damaging the tubules in patients.• Correction of hypovolemia - In rhabdomyolysis, saline solutions are used intravenously under diuresis control.• Elimination of metabolic disorders and intoxication - In this case, calcium gluconate, sodium bicarbonate, enterosorbents are given to the patient.• Extracorporeal hemocorrection - This is considered a promising method of patient recovery. Sometimes plasmapheresis is used, while hemodialysis is used in acute kidney failure [1].Currently, the correct use of glucocorticosteroid (GCS) drugs in appropriate doses in preventing acute kidney injury greatly helps in early recovery from the disease and prevention of subsequent complications that may be observed. In acute tubulointerstitial nephritis of rhabdomyolysis etiology, it is appropriate to use GCS with moderate duration of action - prednisolone and methylprednisolone [2,3].
2. Materials and Methods
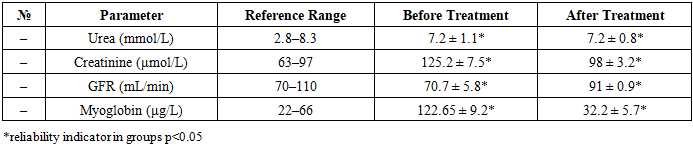
- During the study, 78 male patients with an average age of 29±8.5 were studied. They formed 2 main groups: Group 1 consisted of 64 patients who had signs of kidney damage of rhabdomyolysis etiology after physical exertion. Group 2 consisted of 14 patients who did not have signs of kidney damage of rhabdomyolysis etiology after physical exertion.Physical loads consisted of: running 1000 meters within a time interval (to assess endurance) and running 100m in a short time interval (loaded exercise), 10 pull-ups, and performing a set of strength-oriented exercises within a specified time interval.From laboratory indicators, signs indicating rhabdomyolysis and kidney damage of rhabdomyolysis etiology were taken as: elevated levels of myoglobin, urea, creatinine in biochemical blood analysis, and decreased glomerular filtration. Biochemical examination results were performed using the Cobos 311 apparatus (Germany). Evaluation of renal glomerular filtration was calculated according to the EPI formula adopted in 2011.
3. Discussion of Results
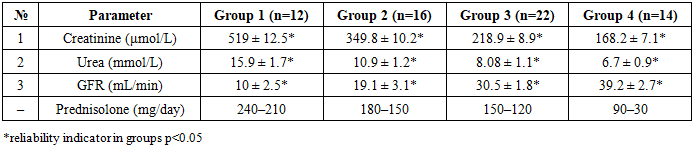
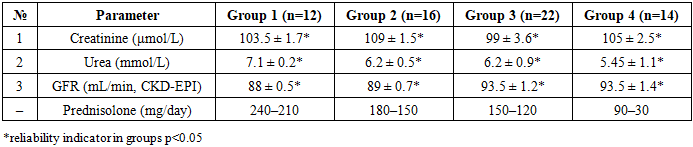
- In patients who experienced kidney damage due to rhabdomyolysis after physical exertion, plasma creatinine was taken as the main indicator and was conditionally divided into 4 groups according to the increase in this indicator (Table 1). Such division provides convenience for the quantitative determination of GCS therapy for patients in our treatment institution in subsequent cases.• Group 1 included patients with plasma creatinine levels of 600-400 μmol/L, and these group patients started with an initial daily dose of prednisolone of 210-240 mg/day.• Group 2 included patients with plasma creatinine levels of 400-300 μmol/L, and these group patients started with an initial daily dose of prednisolone of 180-150 mg/day.• Group 3 included patients with plasma creatinine levels of 300-200 μmol/L, and these group patients started with an initial daily dose of prednisolone of 150-120 mg/day.• Group 4 included patients with plasma creatinine levels of 200-150 μmol/L, and these group patients started with an initial daily dose of prednisolone of 90-30 mg/day (Table 1).
|
|
|
4. Conclusions
- In conclusion, rhabdomyolysis-etiology AKI is observed even among military personnel with physical fitness when performing intensive physical loads. In cases where AKI develops, timely and appropriate dose application of GCS is of great importance. The rational use of the above-mentioned GCS (prednisolone) drugs leads to early recovery from the disease, prevention of complications arising as a result of the disease, and elimination of AKI while using GCS in sufficient doses based on short schemes. This allows for rapid restoration of the patient's kidney function and enables the patient to return to work activities in the shortest possible time.