-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 2902-2908
doi:10.5923/j.ajmms.20251509.12
Received: Aug. 6, 2025; Accepted: Sep. 2, 2025; Published: Sep. 8, 2025

Longitudinal Analysis of Bowel Function and Quality of Life in Children Treated for Low Anorectal Malformations
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLYuldashev Muzaffar Abduvoxidovich1, Toshboev Sherzod Olimovich2
1Department of Pediatric Surgery, Andijan State Medical Institute, Andijan, Uzbekistan
2Department of Anesthesiology and Emergency Medicine, Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Toshboev Sherzod Olimovich, Department of Anesthesiology and Emergency Medicine, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This study evaluated long-term functional outcomes in 39 children who underwent surgical treatment for low anorectal malformations. Comparative analysis revealed that single-stage sphincter-sparing procedures-especially anterior sagittal anorectoplasty (ASARP) - were associated with significantly better quality of life scores compared to conventional two-stage operations, particularly in the domains of physical and emotional functioning. In contrast, children who underwent two-stage procedures exhibited substantially lower PedsQL scores across all domains. A clear inverse correlation was observed between the Baylor Continence Score (BCS) and the total PedsQL score, indicating that increased defecation-related dysfunction negatively impacts quality of life. These findings underscore the importance of early identification and management of bowel symptoms and the need for regular, multidimensional functional monitoring using validated assessment tools.
Keywords: Low anorectal malformations, Anterior sagittal anorectoplasty, Continence, Quality of life, PedsQL, BCS score, Infants
Cite this paper: Yuldashev Muzaffar Abduvoxidovich, Toshboev Sherzod Olimovich, Longitudinal Analysis of Bowel Function and Quality of Life in Children Treated for Low Anorectal Malformations, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 2902-2908. doi: 10.5923/j.ajmms.20251509.12.
Article Outline
1. Introduction
- Anorectal malformations (ARMs) represent a significant proportion of surgical pathologies encountered in neonates, infants, and young children. These anomalies are among the leading causes of severe congenital disability in pediatric patients, with an estimated incidence of approximately 1 in every 5,000 live births [3,10]. ARMs encompass a wide clinical spectrum, ranging from simple low-type anomalies to complex high lesions, and their effective management and treatment require a multidisciplinary approach involving not only pediatric surgeons but also neonatologists, pediatricians, gastroenterologists, and rehabilitation specialists. The surgical strategy in patients with ARMs is typically determined by the type and location of the anomaly, the presence of associated malformations, and the overall clinical condition of the child. Treatment may involve either a single-stage radical procedure or a multistage surgical approach. Currently, a variety of surgical techniques are employed for the correction of ARMs, including anoperineal, abdomino-sacral-perineal, and abdominoperineal approaches, as well as anterior sagittal anorectoplasty (ASARP) and posterior sagittal anorectoplasty (PSARP). These procedures may be performed with or without a protective colostomy [6,8]. Recent advancements in surgical technology, anesthesiology, intensive care, medical imaging, and neonatal care have substantially improved the postoperative and long-term management of anorectal malformations (ARMs). These developments have enabled not only the restoration of anatomical integrity but also the implementation of optimized strategies for bowel function management during long-term follow-up [1,2,4]. A review of the literature reveals that the functional outcomes of surgical interventions in ARMs have often been inadequately assessed - typically relying on a limited number of criteria and lacking a uniform, comprehensive methodology. The absence of standardized protocols for long-term evaluation contributes to the variability of reported outcomes and introduces a degree of subjectivity into their interpretation. Functional assessments commonly include clinical examination, anorectal manometry, radiological imaging, and various continence scoring systems such as the Kelly score, the Baylor Continence Scale (BCS), and the Krickenbeck classification [5,11]. In addition, instruments for assessing psychosocial well-being and health-related quality of life (HRQoL), such as the PedsQL questionnaire, are also employed. Despite the availability of these multidimensional tools, their application in clinical practice remains inconsistent [7,9].
1.1. Purpose of the Study
- To conduct a longitudinal analysis of the impact of surgical treatment outcomes on bowel function and quality of life in children diagnosed with low-type fistulous anorectal malformations.
2. Materials and Methods
- This study was based on the clinical records of infants and young children with low-type anorectal malformations (ARMs) who underwent surgical treatment at the Department of Pediatric Surgery of the Andijan Regional Multidisciplinary Medical Center between 2015 and 2024. The investigation was designed as a cross-sectional cohort study. During the study period, a total of 135 children were admitted with diagnoses of “low anorectal malformation,” “atresia ani,” or “atresia ani et recti.” Among them, non-fistulous low-type ARMs were identified in 92 cases (68.1%), while fistulous forms were diagnosed in 43 patients (31.9%). Due to changes in diagnostic and surgical management strategies over the years, the cohort was divided into two groups for comparative analysis. The retrospective group included 73 patients (54.1%) treated between 2015 and 2019, whereas the prospective group comprised 62 patients (45.9%) treated between 2020 and 2024. In line with the study objectives, only patients with fistulous low-type ARMs were included in the main analysis. From the retrospective group, 16 of the 21 patients (21.9%) with fistulous ARM types were included in the control group. Exclusions from this group included 2 cases with rectovesical fistula, 2 with rectovaginal fistula, and 2 neonates with multiple severe congenital anomalies. In the prospective group, 1 patient with a rectovesical fistula and 2 patients with life-incompatible multiple congenital anomalies were also excluded. The remaining 23 patients (37.1%) formed the study group for prospective analysis.Accordingly, after applying the exclusion criteria, a total of 39 infants and young children with fistulous low-type anorectal malformations (ARMs) who underwent surgical treatment were included in the study.
2.1. Study Design
- In the study group, anoperineal and rectoperineal fistulous ARM types were diagnosed in 8 male (34.7%) and 4 female infantss (17.4%), while in the control group, these types were observed in 6 male (37.5%) and 2 female (12.5%), respectively. The rectovestibular fistula was the most common anomaly overall: it was detected in 11 girls (42.8%) in the study group (Group A) and in 5 girls (31.2%) in the control group (Group B). Additionally, the rectoscrotal variant of ARM was diagnosed in 3 boys (18.7%) in the control group (Figure 1).
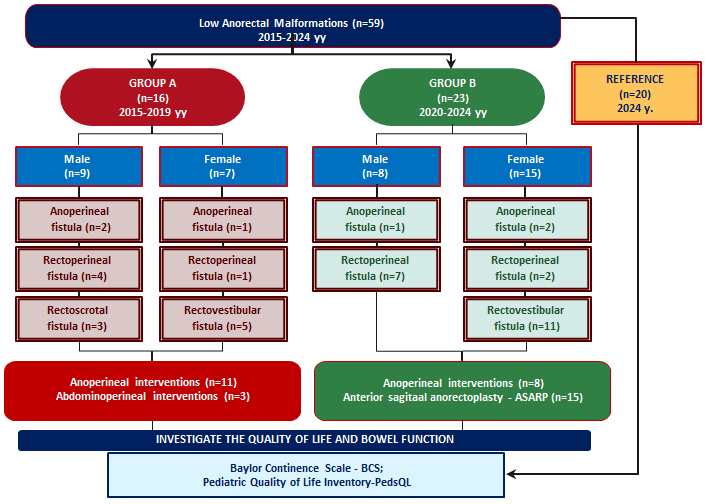 | Figure 1. Study design |
2.2. Surgical Management
- In both the retrospective and prospective groups, depending on the specific type of low-type fistulous anorectal malformation, patients underwent either single-stage anal reimplantation procedures or staged reconstructive anorectoplasty following a protective colostomy. The types of surgical procedures performed in the study groups are presented in Table 1.
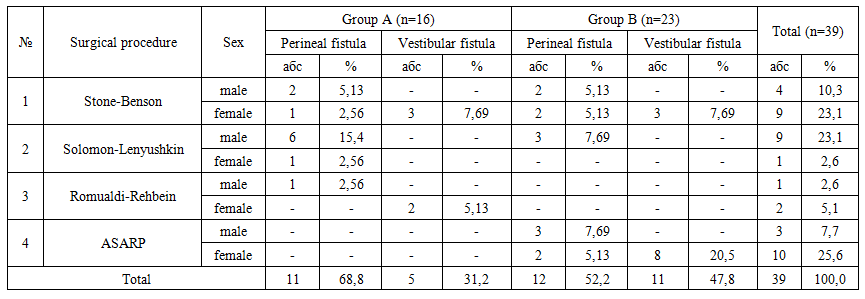 | Table 1. Types of Surgical Procedures Performed in the Study Groups According to Patient Sex and Fistula Type |
2.3. Measurements
- Based on the primary aim of the study, bowel function and its impact on quality of life were assessed in both study groups among children with low anorectal malformations of the anoperineal and vestibular fistula types who had undergone anal reimplantation. To evaluate these outcomes, two validated instruments were employed: the Baylor Continence Scale (BCS), which measures continence and social adaptation, and the Pediatric Quality of Life Inventory (PedsQL 4.0), which assesses health-related quality of life in children [8,9].The BCS consists of 23 questionnaire items with a total score ranging from 2 to 84 points. Lower scores indicate better continence and social adaptation. The PedsQL includes 23 items as well, covering multiple domains, including physical functioning (8 items), emotional functioning, and social functioning, enabling comprehensive assessment of a child’s quality of life. Data for both continence and quality of life scores were obtained from the parents or legal guardians of children under the age of 3, based on their responses to the respective questionnaires.
2.4. Statistical Analysis
- All statistical analyses were performed using IBM SPSS Statistics Base software (version 27.0, 2020, USA) under a proprietary license. A p-value of less than 0.05 was considered the threshold for statistical significance. Categorical variables were compared using the chi-square (χ²) test. Continuous variables were presented as means and standard deviations and were analyzed using either the independent samples t-test or one-way analysis of variance (ANOVA), as appropriate. The significance of differences between study groups was determined using the Clopper–Pearson exact method based on the β-distribution to calculate 95% confidence intervals (CI) for binomial proportions. The correlation between bowel function and quality of life was assessed using Pearson’s correlation coefficient. In addition, a linear regression analysis was performed to evaluate the relationship between BCS scores and overall PedsQL outcomes.
3. Results
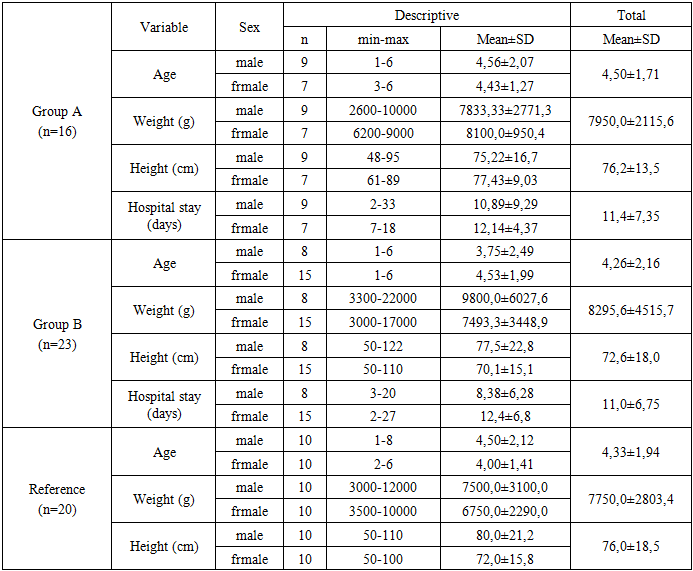
- No significant differences were observed in age or anthropometric parameters (weight and height) between the children included in the study (p>0.05). In the control group, during the observation period, 2 infants (12.5%) were under 3 months of age and 14 children (87.5%) were between 3 and 12 months. In the study group, these values were 6 children (26.1%) under 3 months and 17 children (73.9%) between 3 and 12 months, respectively (Table 2).
|
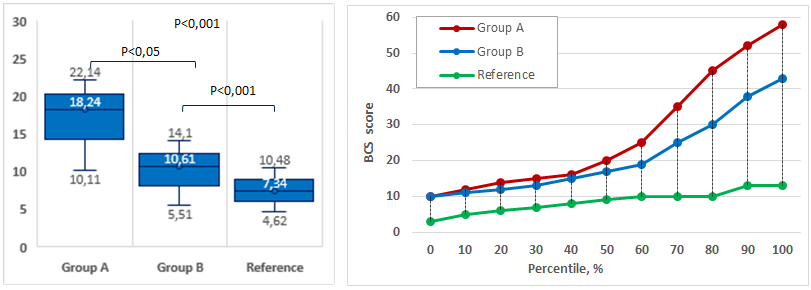 | Figure 2. Mean BCS scores and percentage distribution among children in the study groups |
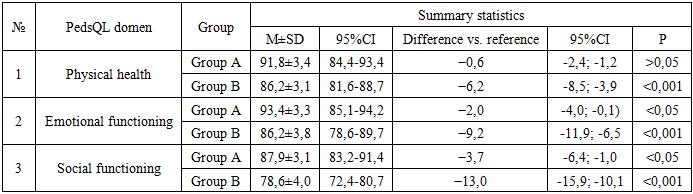
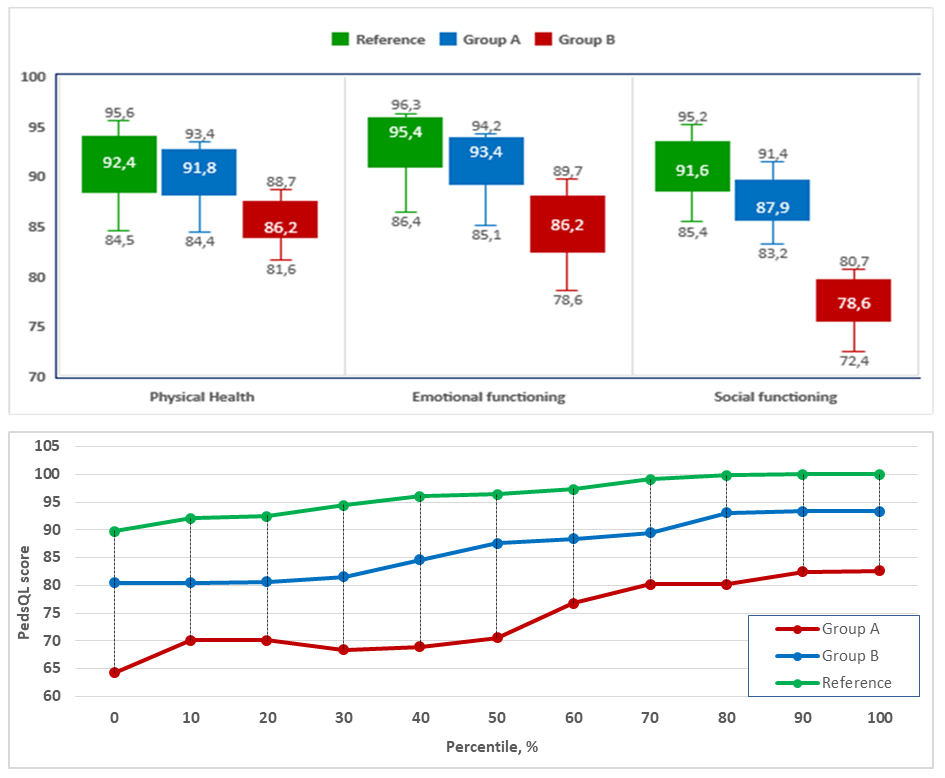 | Figure 3. Comparative PedsQL Domain Scores by Type of Surgery in the Study Groups |
|
4. Conclusions
- The findings of this study demonstrate that in children born with low anorectal malformations, single-stage surgical procedures- particularly those incorporating sphincter-preserving strategies such as anterior sagittal anorectoplasty (ASARP)-enable the maintenance of health-related quality of life at levels nearly comparable to the reference group, especially within the domains of physical health and emotional functioning. Although a slight reduction was noted in the social functioning domain, this decrease was considerably less pronounced compared to that observed following multi-stage procedures involving colostomy. In contrast, the control group exhibited significantly lower quality of life scores across all domains relative to the reference population, indicating that functional and psychosocial recovery is more limited after two-stage surgical approaches.Furthermore, the observed inverse relationship between BCS and PedsQL scores, particularly in the domains of emotional and social functioning, reflects marked impairments in psychosocial integration and emotional stability associated with increasing bowel dysfunction. These findings emphasize the necessity of timely identification and management of defecation-related problems, as well as the importance of continuous monitoring of factors influencing quality of life, including patient age, type of surgical intervention, follow-up duration, and the presence of comorbidities.