-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 2897-2901
doi:10.5923/j.ajmms.20251509.11
Received: Aug. 5, 2025; Accepted: Sep. 1, 2025; Published: Sep. 8, 2025

Features of Clinical Manifestations, Course of Pregnancy and Birth Outcomes in Women with Undifferentiated Connective Tissue Dysplasia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLM. E. Sharipova, D. D. Saidjalalova
Tashkent State Medical University, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the research was to study clinical manifestations, features of pregnancy and birth outcomes in women with undifferentiated connective tissue dysplasia. Background. Undifferentiated connective tissue dysplasia is currently considered one of the most common and underestimated multisystem conditions, especially in women of reproductive age. According to various authors, signs of undifferentiated connective tissue dysplasia occur in 20–40% of women of childbearing age, but in clinical practice it is diagnosed in less than 10%. Material and methods. The study included 202 pregnant women; 102 of them were with diagnosed undifferentiated connective tissue dysplasia (main group) and 100 were somatically healthy women (control group). An analysis of anamnestic, clinical, laboratory and instrumental data, features of pregnancy course, childbirth and the condition of newborns was carried out. Results. Women with undifferentiated connective tissue dysplasia had a significantly higher incidence of complications such as threatened miscarriage (56.8%), cervical insufficiency (42.1%), premature birth (21.5%), weakness of labor activity (34.3%), and postpartum hemorrhage (18.6%). In 29.4% of newborns from the main group, signs of dysplasia were observed. In the control group, the frequency of these complications was statistically significantly lower (p<0.05). Discussion. The clinical phenotype of women with undifferentiated connective tissue dysplasia was characterized by typical signs of systemic connective tissue dysfunction: asthenic somatotype (78.4%), joint hypermobility (65.7%), varicose veins (41.1%), mitral valve prolapse (23.5%), and skin changes (37.2%). These data are consistent with the results of studies presented in the literature, which indicate a high prevalence of asthenic and dysplastic phenotypes among women with undifferentiated connective tissue dysplasia and their association with obstetric pathology. Conclusion. Undifferentiated connective tissue dysplasia is a risk factor for complicated pregnancy and childbirth, requiring individual management and interdisciplinary monitoring.
Keywords: Undifferentiated connective tissue dysplasia, Risk factor, Complicated pregnancy
Cite this paper: M. E. Sharipova, D. D. Saidjalalova, Features of Clinical Manifestations, Course of Pregnancy and Birth Outcomes in Women with Undifferentiated Connective Tissue Dysplasia, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 2897-2901. doi: 10.5923/j.ajmms.20251509.11.
Article Outline
1. Introduction
- Undifferentiated connective tissue dysplasia (UCTD) is currently considered one of the most common and underestimated multisystem conditions, especially in women of reproductive age. According to various authors, signs of UCTD occur in 20–40% of women of childbearing age, but in clinical practice it is diagnosed in less than 10% [1-2].Connective tissue amounts to 60% of the human body mass and participates in the construction of all organs and systems: cardiovascular, respiratory, musculoskeletal, genitourinary, including reproductive. Its structural insufficiency can be the basis for the pathogenesis of a number of obstetric and perinatal complications.The increased interest to this pathology is caused by the following factors: • the high prevalence of UCTD in the population; • non-specificity and polymorphism of the clinical presentation;• insufficient awareness among obstetricians and gynecologists;• increased frequency of complicated pregnancies, deliveries and adverse perinatal outcomes;• risk of developing dysplasia in offspring. Research of UCTD has intensified in recent years, but it is mainly descriptive or localized in nature, most often addressing individual aspects (e.g., the impact of joint hypermobility or valve prolapse on pregnancy).In international practice, UCTD is distinguished as an independent clinical category using the Beighton score for assessing joint hypermobility and the comprehensive criteria according to Villefranche (1998), which was revised in 2017 [3].Studies show an association between UCTD and mitral valve prolapse, varicose veins, premature birth, and isthmic-cervical insufficiency (ICI) [4].Kozlova N.M. et al. (2021) showed that in women with UCTD, the frequency of threatened miscarriage is more than 50%, and in women with ICI, the incidence is up to 40%. Belyaeva Yu.Yu. (2020) studied placental insufficiency in women with dysplasia and proved an increased risk of fetal hypoxia. Khusnullin S.K. noted the need for early detection of UCTD in pregnant women with asthenic phenotype and complaints of rapid fatigue, back pain, varicose veins [5-7,2].However, most studies do not employ a comprehensive interdisciplinary approach. There are also few studies that use objective morphogenetic, cardiometabolic, and echographic assessment methods in pregnant women with UCTD. The aim of the research was to study clinical manifestations, features of pregnancy and birth outcomes in women with undifferentiated connective tissue dysplasia.
2. Material and Methods
- The study was prospective and was conducted at the 9th maternity complex in Tashkent. We examined 202 pregnant women who were treated at our clinic between 2022 and 2024. All patients were divided into two groups. The main group (n = 102) consisted of women with a confirmed diagnosis of UCTD (according to the criteria of cartilaginous, cutaneous, vascular, musculoskeletal symptoms, Beighton index ≥ 4). The control group (n = 100) consisted of healthy women without signs of dysplasia, matched for age and gestational age. Clinical history, physical status, ultrasound data, Dopplerometry, cardiography, delivery, and the condition of newborns were evaluated. Statistical processing was carried out using the χ² criterion, according to which p<0.05 was considered significant.
3. Results
- Asthenic body type among patients with UCTD was observed in 80 (78.4%) patients in the main group and in 32 (32.0%) cases in the control group. The asthenic or dysplastic somatotype is characterized by the following signs: • tall stature with insufficient body weight (body mass index <18.5–20 kg/m²); • narrow shoulders and chest, long limbs; • severe thoracic kyphosis or scoliosis; • narrow face with elongated features, thin lips. These features reflect a systemic deficiency of collagen structures, which disrupts the normal formation of the musculoskeletal frame. The asthenic type is one of the most common external manifestations of dysplasia, is detected in most patients with UCTD and can be combined with postural hypotension, increased fatigue, pain in the muscles and back (Table 1).
|

|
|
4. Discussion
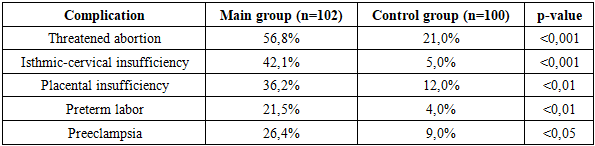
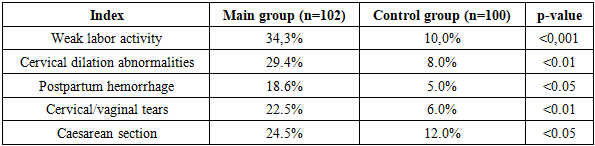
- The results obtained confirm that undifferentiated connective tissue dysplasia (UCTD) is a significant predictor of complicated pregnancy, childbirth, and adverse perinatal outcomes.The clinical phenotype of women with UCTD was marked by typical signs of systemic connective tissue dysfunction: asthenic somatotype (78.4%), joint hypermobility (65.7%), varicose veins (41.1%), mitral valve prolapse (23.5%), skin changes (37.2%). These data are consistent with the results of studies presented in the literature, which indicate a high prevalence of asthenic and dysplastic phenotypes among women with UCTD and their association with obstetric pathology [5,8]. The high frequency of pregnancy complications in the main group (threat of miscarriage — 56.8%, ICI — 42.1%, placental insufficiency — 36.2%, IUGR — 18.6%) reflects a violation of the structural and functional integrity of the connective tissue elements of the uterus, vessels and placenta. Joint hypermobility and weakness of the collagen structures of the cervix can promote isthmic-cervical insufficiency, while vascular insufficiency and fetoplacental insufficiency can develop into placental insufficiency and fetal growth restriction. These pathogenetic mechanisms were previously described by De Paepe A. (2018) and Malfait F. (2017) [3-4]. Features of labor in women with UCTD included: weak labor activity (34.3%), abnormal cervical dilation (29.4%), postpartum hemorrhage (18.6%), frequent traumatic tears (22.5%), increased frequency of cesarean section (24.5%).This pattern of complications demonstrates that functional failure of the myometrium and connective tissue structures of the birth canal is a key factor in birth complications.Perinatal outcomes were also worse in the main group: the body weight of newborns was significantly lower (2760 ± 240 g vs. 3110 ± 280 g), and a low Apgar score <7 at the 1st minute was observed in 15.6% of cases (vs. 4.0% in the control group). It confirms that systemic connective tissue dysplasia of the mother adversely affects fetoplacental function and the adaptive abilities of the newborn.Thus, a comprehensive analysis of clinical, obstetric, and perinatal data shows that UCTD is a multisystem risk factor requiring early detection, dynamic monitoring and personalized prevention of obstetric complications.
5. Conclusions
- Undifferentiated connective tissue dysplasia in women of reproductive age is associated with a high risk of complicated pregnancy and childbirth, including threatened miscarriage, isthmic-cervical insufficiency, placental insufficiency, IUGR and preterm birth.The clinical profile of UCTD (asthenic type, joint hypermobility, varicose veins, mitral valve prolapse, skin changes) is a significant diagnostic marker for the early detection of patients at a risk.The course of labor in women with UCTD is associated with an increased frequency of labor abnormalities, traumatic tears, and postpartum hemorrhage, often requiring surgical delivery.Perinatal outcomes were more unfavorable in the main group: there was a decrease in the body weight of newborns and more frequent asphyxia at birth, which was associated with chronic fetoplacental insufficiency.The identified features justify the need for early screening for UCTD, personalized management of pregnancy and childbirth, including prevention of ICI, placental insufficiency and obstetric hemorrhage.
Conflict of Interests’ Statement
- The authors declare no conflict of interest. This study does not include the involvement of any budgetary, grant or other funds. The article is published for the first time and is part of a scientific work.
ACKNOWLEDGEMENTS
- The authors express their gratitude to the management of the multidisciplinary clinic of the 9th Maternity Complex in Tashkent for the material provided for our study.
Ethical Approval and Consent to Participate
- The Research Ethics Board of our institution does not require review or approval of case reports. Our research was carried out in accordance with the World Medical Association Code of Ethics (Declaration of Helsinki).
Source of Funding
- Each of the authors has reviewed and approved this manuscript. None of the authors has a conflict of interest, financial or otherwise. This manuscript is original, no part of it has been previously published and is not being considered for publication elsewhere. The corresponding author agrees to accept full responsibility for authorship at the submission and review stages of the manuscript.
Ethical Aspects
- All patients signed voluntary informed consent to participate. Personal data were encrypted and used only for scientific purposes.