-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 2893-2896
doi:10.5923/j.ajmms.20251509.10
Received: Aug. 2, 2025; Accepted: Sep. 1, 2025; Published: Sep. 8, 2025

The Impact of Deep Parasternal Block after Coronary Artery Bypass Grafting Surgery on Clinical Outcomes in the Early Postoperative Period
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLV. Kh. Sharipova1, N. A. Akramova2, Sh. A. Yuldosheva1
1Republican Research Center of Emergency Medicine, Tashkent, Uzbekistan
2Bukhara Branch of the Republican Research Center of Emergency Medicine, Bukhara, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the study was to evaluate the impact of deep parasternal block after coronary artery bypass grafting surgery on clinical outcomes in the early postoperative period. Background. Recent scientific researchers have focused on the development and implementation of a multimodal concept of pain relief, which aims to reduce opioid consumption and actively introduce regional pain relief methods into postoperative pain management practice. Studying the impact of parasternal block after coronary artery bypass grafting surgery in the early postoperative period on clinical outcomes is currently a relevant issue requiring scientific research in this area. Material and methods. The study included 121 patients after coronary artery bypass grafting surgery. Patients were divided into two groups depending on the method of postoperative pain relief: Group 1 (n=60) - deep parasternal block on both sides under ultrasound guided navigation. Group 2 (n=61) received postoperative pain relief with narcotic analgesics (morphine, promedol) in combination with nonsteroidal anti-inflammatory drugs and paracetamol at a dose of 1000 mg. Results. The use of deep parasternal block under ultrasound guidance as the basic method of pain relief after coronary artery bypass grafting surgery has a beneficial impact on the clinical results of the study. This method contributed to a 95% reduction in the consumption of narcotic analgesics in Group 1 patients compared to Group 2 patients; a 37.3% reduction in the time required for extubation; a 43.4% reduction in the incidence of postoperative nausea and vomiting; a 2.1-fold decrease in episodes of abdominal distension; and a 45.5% reduction in the time taken for intestinal peristalsis recovery. Conclusion. Deep parasternal block after coronary artery bypass grafting surgery has a beneficial impact on clinical outcomes in the early postoperative period.
Keywords: Parasternal block, Coronary artery bypass grafting, Postoperative analgesia, Narcotic analgesic
Cite this paper: V. Kh. Sharipova, N. A. Akramova, Sh. A. Yuldosheva, The Impact of Deep Parasternal Block after Coronary Artery Bypass Grafting Surgery on Clinical Outcomes in the Early Postoperative Period, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 2893-2896. doi: 10.5923/j.ajmms.20251509.10.
Article Outline
1. Introduction
- The implementation of the concept of accelerated recovery aims to achieve both rapid and high-quality recovery after cardiac surgery [1]. Since these goals may contradict high-dose opioid administration, perioperative pain relief protocols should include alternative pain relief methods or opioid adjuvants [2]. Recent scientific studies have been devoted to the development and implementation of a multimodal concept of pain relief, which aims to reduce opioid consumption and actively introduce regional pain relief methods into postoperative pain relief practice [3-4].Today, there is an urgent need to develop a strategy to reduce perioperative opioid use in cardiac surgery while ensuring efficient postoperative analgesia for patients after cardiac surgery. This is facilitated by the introduction of regional pain relief methods under ultrasound guided navigation [5-6]. One of the new approaches to treating postoperative pain syndrome in cardiac surgery is deep parasternal block under ultrasound guided navigation. A review of recent literature has revealed that studies aimed at investigating the efficiency and safety of parasternal block after coronary artery bypass grafting were based on the study of hemodynamic parameters, stress hormones, clinical laboratory data and certain factors of clinical outcome of the disease [7-8]. Studying the impact of parasternal block after coronary artery bypass grafting surgery in the early postoperative period on clinical outcomes is currently a relevant issue requiring scientific research in this area. The aim of the study was to evaluate the impact of deep parasternal block after coronary artery bypass grafting surgery on clinical outcomes in the early postoperative period.
2. Material and Methods
- The study included 121 patients who underwent off-pump coronary artery bypass grafting at the Republican Research Center of Emergency Medicine and its Bukhara branch between 2022 and 2024. Patients were divided into two groups depending on the method of postoperative pain relief. The first group (main group) included 60 patients. The mean age of patients was 62.48 ± 9.00 years. There were 45 (75%) men and 15 (25%) women. Postoperative pain relief was provided as follows: immediately after the surgery, patients received a deep parasternal block on both sides under ultrasound navigation control. Narcotic analgesics were used as a “rescue strategy” when needed. The second group (control group) consisted of 61 patients. The mean age was 61.95 ± 7.41 years. There were 44 (72.1%) men and 17 (27.9%) women. Postoperative pain relief was provided using narcotic analgesics (morphine, promedol) in combination with NSAIDs and paracetamol at a dose of 1000 mg. All patients were diagnosed with ischemic heart disease of varying severity. Among concomitant pathologies, chronic obstructive pulmonary disease was detected in 20.7% of cases, diabetes mellitus of various stages - in 29.7% of cases, and obesity of varying severity - in 19.8% of cases. The following indicators were recorded in the postoperative period: • time of first analgesic requirement;• extubation time;• time of gastrointestinal motility recovery;• presence of postoperative nausea and vomiting;• amount of narcotic analgesic used in the postoperative period;• duration of stay in the intensive care unit;• duration of hospital stay. Statistical analysis was performed using StatTech v. 4.8.3 (developed by StatTech LLC, Russia). Pearson's chi-square test and Welch's t-test were used to evaluate the statistical significance of the results.
3. Results
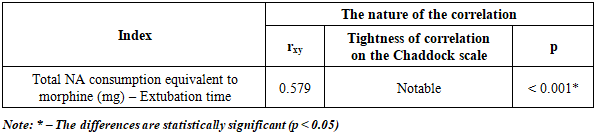
- Against the background of a decrease in the use of parasternal blocks as part of a multimodal analgesia regimen, there was a 95% reduction in the consumption of narcotic analgesics (NA) in the main group of patients compared to the control group. A reduction in the consumption of narcotic analgesics led to improved treatment outcomes in the postoperative period, which were also manifested by a reduction in the extubation time of patients in the main group by 37.3%. A correlation analysis of the relationship between the total consumption of narcotic analgesics and the time of extubation revealed a significant direct correlation (Table 1).
|
|
|
|
4. Conclusions
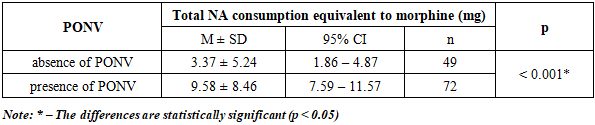
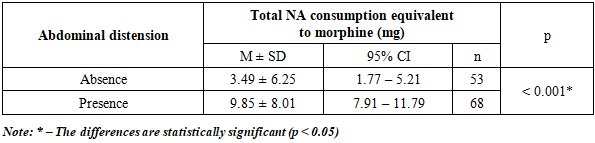
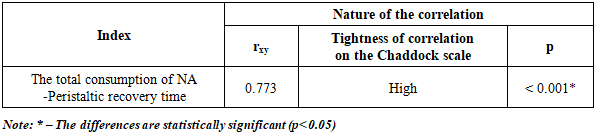
- The use of deep parasternal block under ultrasound navigation control as a basic method of pain relief after coronary artery bypass grafting surgery has a beneficial effect on clinical results of the study. This method contributed to a 95% reduction in the consumption of narcotic analgesics in patients in the main group compared to patients in the control group; reduction in extubation time for patients in the main group by 37.3%; reduction in the incidence of postoperative nausea and vomiting by 43.4%; reduction of abdominal distension episodes by 2.1 times; reduction of intestinal peristalsis recovery time by 45.5%.
Conflict of Interests’ Statement
- The authors declare no conflict of interest. This study does not include the involvement of any budgetary, grant or other funds. The article is published for the first time and is part of a scientific work.
ACKNOWLEDGEMENTS
- The authors express their gratitude to the management of the multidisciplinary clinic of Republican Research Center of Emergency Medicine (RRCEM) and its Bukhara branch for the material provided for our study.
Source of Funding
- Each of the authors has reviewed and approved this manuscript. None of the authors has a conflict of interest, financial or otherwise. This manuscript is original, no part of it has been previously published and is not being considered for publication elsewhere. The corresponding author agrees to accept full responsibility for authorship at the submission and review stages of the manuscript.
Ethical Aspects
- The study was approved by the local ethics committee of the Republican Research Center of Emergency Medicine (RRCEM). All patients signed voluntary informed consent to participate. Personal data were encrypted and used only for scientific purposes.