-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(9): 2888-2892
doi:10.5923/j.ajmms.20251509.09
Received: Jul. 4, 2025; Accepted: Aug. 2, 2025; Published: Sep. 3, 2025

Comparative Clinical and Pathomorphological Analysis of Tuberculous Spondylitis with and without the Influence of COVID-19
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMamajonov Ikboljon Maribjonovich1, Makhkamov Nosirjon Jurayevich2
1Independent Researcher, Andijan State Medical Institute, Andijan, Uzbekistan
2Associate Professor, Doctor of Medical Sciences, Andijan State Medical Institute, Andijan, Uzbekistan
Correspondence to: Mamajonov Ikboljon Maribjonovich, Independent Researcher, Andijan State Medical Institute, Andijan, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This scientific article presents a comparative clinical and pathomorphological analysis of tuberculous spondylitis in cases associated with COVID-19 infection and those without it. Clinical observations revealed that tuberculous spondylitis complicated by COVID-19 was characterized by more pronounced general intoxication symptoms, more severe pain syndrome, and a more rapid progression of motor function limitations. Pathomorphological analysis demonstrated that cases of tuberculous spondylitis associated with COVID-19 showed more extensive neutrophilic infiltration, foci of caseous necrosis, signs of vasculitis, and the proliferation of fibrous tissue. Furthermore, on the microscopic level, increased vascular damage and immune complex alterations were noted under the influence of COVID-19. These findings play a significant role in better understanding the course of tuberculous spondylitis, improving differential diagnostic criteria, and developing more effective treatment strategies.
Keywords: Tuberculous spondylitis, COVID-19, Clinical features, Pathomorphology, Caseous necrosis, Vasculitis, Immune complexes, Spinal tuberculosis, Differential diagnosis
Cite this paper: Mamajonov Ikboljon Maribjonovich, Makhkamov Nosirjon Jurayevich, Comparative Clinical and Pathomorphological Analysis of Tuberculous Spondylitis with and without the Influence of COVID-19, American Journal of Medicine and Medical Sciences, Vol. 15 No. 9, 2025, pp. 2888-2892. doi: 10.5923/j.ajmms.20251509.09.
Article Outline
1. Introduction
- In recent years, the systemic impact of COVID-19 on the human body particularly its effect on the immune system, pro-inflammatory cytokine activity, and microcirculatory disturbances — has significantly altered the course of many chronic diseases [1,2]. This is especially relevant in the case of tuberculosis (TB), where coinfection with COVID-19 appears to exacerbate disease progression. In patients with tuberculous spondylitis, the presence of COVID-19 is associated with more severe clinical symptoms, such as intensified pain, systemic intoxication, and decreased spinal mobility [3,4].Pathomorphologically, COVID-19-positive TB spondylitis cases demonstrate more aggressive features, including pronounced neutrophilic infiltration, vasculitis, caseous necrosis, and widespread fibrosis within spinal tissues [5,6]. Furthermore, SARS-CoV-2 infection leads to endothelial dysfunction, hypercoagulation, and immune-complex-mediated damage, which significantly worsens the course of tuberculous lesions [7–9].In Uzbekistan, an increasing number of TB cases among both younger and older populations, particularly in the post-COVID period, has emphasized the need for comprehensive investigation of this comorbidity [10,11]. Comparative clinical and pathomorphological analysis of tuberculous spondylitis with and without the influence of COVID-19 is essential for understanding the immune-mediated mechanisms and for optimizing diagnostic and treatment strategies [12,13].
2. Purpose of Research
- The main purpose of this study is to conduct a comparative analysis of the clinical and pathomorphological characteristics of tuberculous spondylitis with and without the influence of COVID-19 infection, to identify the differences between these two conditions, and to improve differential diagnostic and therapeutic approaches that are essential for clinical practice.
3. Materials and Methods
- This research was conducted on histological specimens obtained from 150 patients diagnosed with tuberculous spondylitis at the Andijan Regional Center for Phthisiology and Pulmonology during the period from 2019 to 2023. Tissue samples were fixed in 10% neutral buffered formalin following standard histoprocessing protocols, embedded in paraffin blocks, and sectioned into 4–5 µm thick slices using a microtome.Several classical histological staining techniques were applied to enable a comprehensive assessment of tissue architecture and pathological changes. Hematoxylin and eosin (H&E) staining was used to assess general tissue architecture and cellular morphology. The Van Gieson method was applied to highlight areas of caseous necrosis and granulomatous inflammation, while Masson’s trichrome staining was utilized to visualize collagen fibers and assess the extent of fibrosis.A detailed morphometric and comparative pathomorphological analysis was carried out. All cases were categorized into two groups: those with confirmed concurrent COVID-19 infection and those without. Morphometric parameters such as the extent of fibrotic tissue proliferation, area of necrosis, degree of neutrophilic infiltration, and presence of vasculitic changes were quantitatively assessed using digital image analysis software calibrated for histological evaluation. The collected data were statistically analyzed to identify significant differences between the two groups and to better understand the modifying influence of COVID-19 on the pathological course of tuberculous spondylitis.
4. Results and Discussion
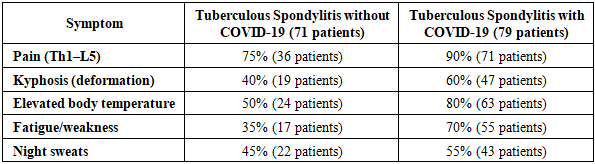
- The results of this study clearly demonstrated the clinical, pathomorphological, and morphometric differences between cases of tuberculous spondylitis associated with COVID-19 and those without. In particular, the analysis of clinical symptomatology revealed that the disease progresses more severely and rapidly under the influence of COVID-19 infection. The primary symptoms related to lesions in the thoracic (Th1–Th12) and lumbar (L1–L5) segments of the spine—namely, pain, kyphosis, elevated body temperature, general fatigue, and night sweats—were thoroughly analyzed.A total of 150 patients were included in the study. Among them, 71 patients had tuberculous spondylitis associated with COVID-19 infection, while the remaining 79 patients had tuberculous spondylitis without COVID-19 involvement. The table below presents the differences in the clinical frequency of these symptoms between the two groups (see Table 1).
|
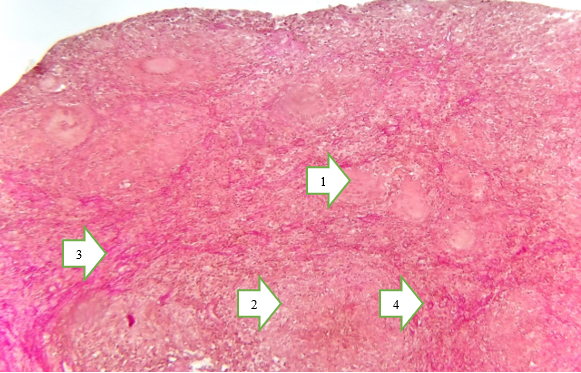 | Figure 1. Under the influence of COVID-19. Pirogov–Langhans giant cells (1). Caseous necrosis (2). Fibrous connective tissue structures surrounding the necrotic area (3). Vascular wall sclerosis (4). Size: 4×10. Stain: Van Gieson |
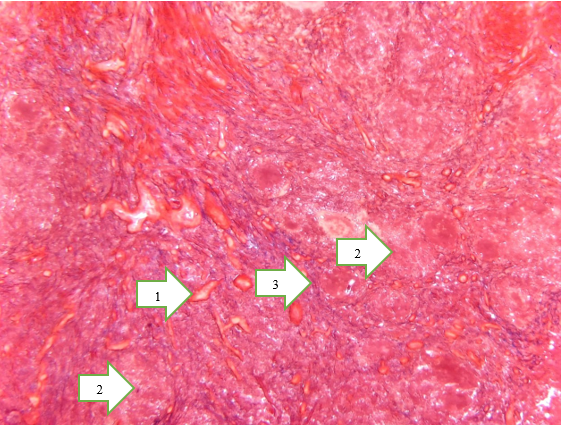 | Figure 2. Without the influence of COVID-19. Sclerosis of the vascular wall and collagen fibers (1). Foci of necrosis (2). Collagen fibers surrounding the necrotic area (3). Magnification: 4×10. Size: 4×10. Stain: Van Gieson |
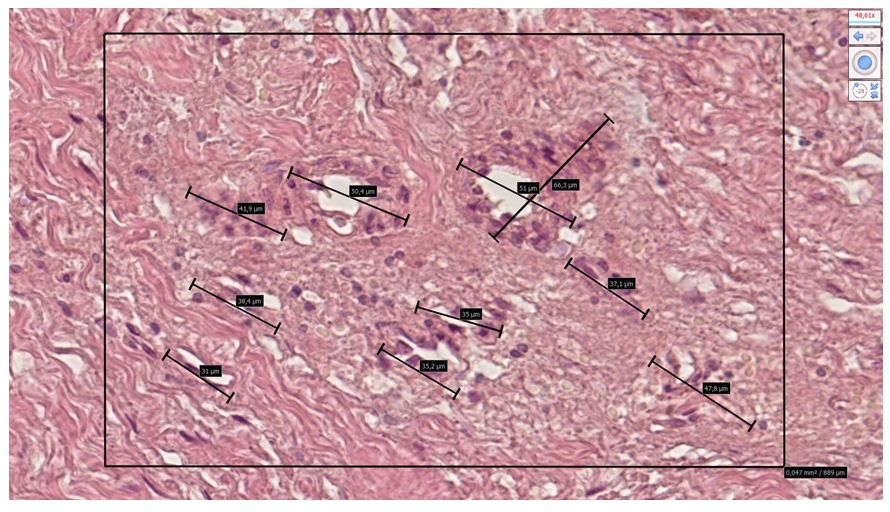
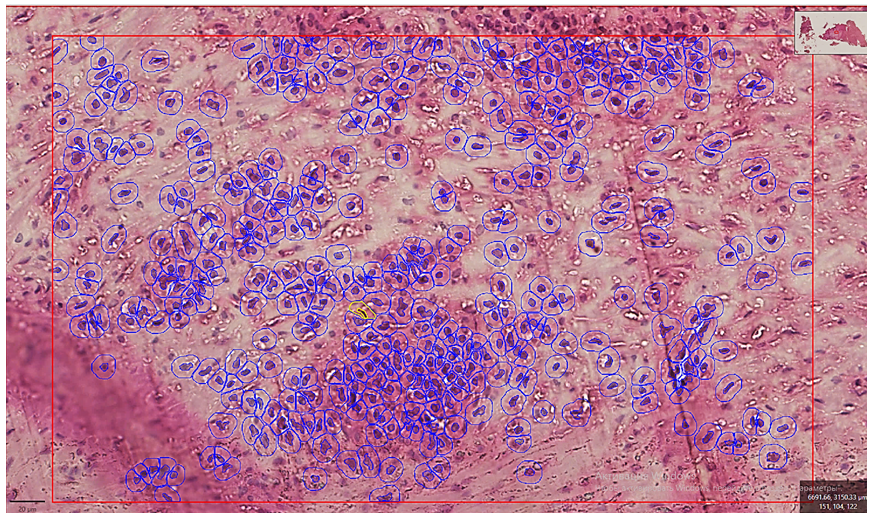 | Figure 3. In tuberculous spondylitis developed under the influence of COVID-19, the number and area occupied by leukocytes within the productive inflammatory focus of bone tissue are presented. The microscopic specimen was scanned using the NanoZoomer (REF C13140-21, S/N000198, HAMAMATSU PHOTONICS, 431-3196 JAPAN). Staining: G.E. Dimensions: 10x20 |
 | Figure 4. In the area of chronic productive inflammation of bone tissue, pericyte cell proliferation was observed around the vascular perimeter, and the vessel diameter was measured. The microscopic specimen was scanned using the NanoZoomer (REF C13140-21, S/N000198, HAMAMATSU PHOTONICS, 431-3196 JAPAN). The boundaries of cellular and fibrous structures in the arterial walls were presented with precise dimensions. Staining: G.E. Dimensions: 10x20 |
5. Conclusions
- The conducted comparative morphological and morphometric analysis has convincingly demonstrated that tuberculous spondylitis associated with COVID-19 infection possesses distinct pathogenetic features and histological hallmarks compared to classical tuberculous lesions. A defining characteristic in these cases is the presence of systemic vasculitis involving small-caliber blood vessels, surrounded by zones of extensive caseous necrosis and intense cellular infiltration composed of epithelioid cells and Pirogov–Langhans type multinucleated giant cells.Moreover, the marked proliferation of pericytic and fibroblastic elements, particularly in the post-viral phase, underscores the heightened reparative response and fibrotic transformation associated with COVID-19-mediated immune dysregulation. Morphometric findings further substantiate these observations, with a pronounced reduction in preserved trabecular bone area (1.68% vs. 4.41% in classical cases), and a statistically significant increase in both the number and diameter of giant cells, suggesting intensified immunopathological activity.Of particular note is the presence of mixed-type inflammatory responses, including aseptic necrosis and lymphoplasmacytic infiltration, indicative of overlapping infectious and post-infectious immune mechanisms.Taken together, these findings suggest that COVID-19 significantly exacerbates the pathomorphological progression of tuberculous spondylitis, resulting in more aggressive tissue destruction, complex healing responses, and potentially poorer clinical outcomes. Accordingly, such cases necessitate meticulous histopathological monitoring and the development of tailored, multidisciplinary treatment strategies.