-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(8): 2829-2832
doi:10.5923/j.ajmms.20251508.87
Received: Aug. 6, 2025; Accepted: Aug. 23, 2025; Published: Aug. 30, 2025

Early Diagnosis of Microelementosis After Surgical Treatment of Obesity: Clinical and Laboratory Analysis in 130 Patients
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLMadaripova Dildora Azimovna
Assistant of the Department of Hematology and Clinical Laboratory Diagnostics of the Bukhara State Medical Institute named after Abu Ali ibn Sino, Bukhara, Uzbekistan
Correspondence to: Madaripova Dildora Azimovna, Assistant of the Department of Hematology and Clinical Laboratory Diagnostics of the Bukhara State Medical Institute named after Abu Ali ibn Sino, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

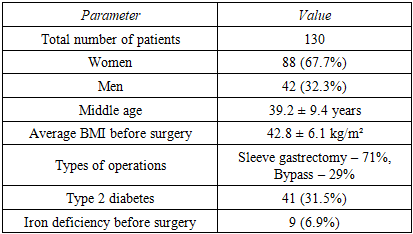
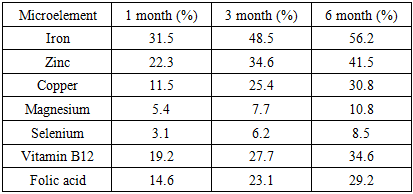
Surgical treatment of obesity (bariatric surgery) effectively reduces body weight, but is often accompanied by disturbances in the metabolism of microelements. The purpose of this study was the early diagnosis of microelementoses in patients who underwent bariatric surgery and the identification of risk factors for their development in the early postoperative period. Materials and methods: 130 patients who underwent various types of surgical treatment for obesity were examined. The concentrations of iron, zinc, copper, magnesium, selenium, vitamin B12 and folates were assessed dynamically - after 1, 3 and 6 months. Results of the study: it was established that microelement deficiency develops in more than 60% of cases by the 3rd month after surgery, and more often in women and patients with initially low levels of hemoglobin and ferritin. The most frequently observed deficiency was iron (56%), zinc (41%) and copper (30%). Conclusion: the study highlights the need for routine monitoring of micronutrient status from the first month after surgery and early initiation of corrective therapy.
Keywords: Bariatric surgery, Microelementosis, Iron deficiency, Zinc, Copper, Postbariatric complications
Cite this paper: Madaripova Dildora Azimovna, Early Diagnosis of Microelementosis After Surgical Treatment of Obesity: Clinical and Laboratory Analysis in 130 Patients, American Journal of Medicine and Medical Sciences, Vol. 15 No. 8, 2025, pp. 2829-2832. doi: 10.5923/j.ajmms.20251508.87.
Article Outline
1. Introduction
- According to WHO, more than 650 million adults worldwide suffer from obesity, and this figure continues to grow [5]. Among the effective methods of treating morbid obesity, bariatric surgery occupies a special place, including such methods as sleeve gastrectomy, biliopancreatic bypass and Roux-en-Y gastric bypass [12]. Despite the positive impact on body weight, bariatric surgery is associated with certain risks, including disturbances in the absorption of micronutrients [1]. Microelementosis is a condition in which the concentration of microelements in the body is disrupted, leading to metabolic, immunological and neurological disorders [4]. After bariatric surgery, this condition may occur as a result of decreased secretion of gastric juice, decreased food volume, and absorption disorders in the altered gastrointestinal tract [2,9]. Microelementoses after surgical treatment of obesity are a complex of metabolic disorders that arise as a result of a deficiency or excess of microelements caused by changes in the anatomical and physiological conditions of absorption of nutrients in the gastrointestinal tract after bariatric surgery [3,6]. These conditions acquire special clinical significance due to the high prevalence and severity of nutritional disorders in patients who have undergone weight loss surgery, especially bypass or combined interventions (sleeve gastrectomy, biliopancreatic diversion, gastric bypass, etc.) [11].Etiopathogenesis. After bariatric surgeries, the absorption of trace elements (iron, zinc, copper, selenium, calcium, magnesium, etc.) is disrupted due to a reduction in the volume of the stomach, bypassing parts of the small intestine, changing the pH of the environment and microbiota. A decrease in the secretion of gastric juice and enzymes, as well as insufficient food intake, leads to a decrease in the bioavailability of trace elements. Increased inflammatory processes and catabolism after surgery can contribute to a more rapid depletion of trace element reserves [7,8].Common deficiencies: Iron - anemia, chronic fatigue, cognitive impairment; Zinc - dermatological manifestations, delayed wound healing, decreased immunity; Calcium and vitamin D - osteopenia, osteoporosis, muscle weakness; Magnesium - neuromuscular and cardiovascular symptoms; Copper - neurological disorders, anemia; Selenium - cardiomyopathy, weakness, thyroid dysfunction; B vitamins, especially B12 - neurological symptoms, anemia [10].Early diagnosis and correction of micronutrient deficiencies is critical to preventing complications and improving long-term outcomes of obesity surgery. Despite this, this problem remains understudied in the early postoperative period.The purpose of the study: to assess the frequency, nature and dynamics of the development of microelementoses in the early postoperative period in patients who have undergone bariatric surgery.
2. Materials and Methods
- Study design: prospective, cohort, with dynamic observation. Patients were randomly selected in the Bukhara Regional Multidisciplinary Medical Center in the Department of Surgery. For the study, patients in the age category from 20 to 55 years who had undergone bariatric surgery for obesity were selected. Participation in the scientific study was strictly by oral consent of the patients. Period: January 2023 – June 2025. The patient characteristics are shown in Table 1 below.
|
3. Research Results
- 1. General frequency of microelementosesBy the 6th month after surgery, a deficiency of at least one microelement was detected in 81 patients (62.3%).2. Frequency of micronutrient deficiencies
|
4. Discussion
- The results of the study confirm the hypothesis of a high incidence of micronutrient deficiency after bariatric interventions. Despite the initial normal content of micronutrients in most patients, a significant decrease in their levels is observed by the 3rd month after surgery.Iron is the most sensitive indicator, especially in women. This is due to a decrease in stomach acid (hypochlorhydria), a violation of the conversion of iron into an absorbable form and the exclusion of meat foods.Zinc is involved in tissue regeneration, immunity and protein synthesis. Its deficiency has been associated with hair loss and delayed wound healing.Copper and vitamin B12 are critical for the nervous system. Their deficiency can lead to irreversible neurological damage.Selenium and magnesium – although less commonly found in deficiency, their role in antioxidant protection and muscle function makes their monitoring essential.
5. Recommendation
- Based on the data obtained, an algorithm for early monitoring and correction of microelementoses was developed.Before surgery:- Screening for iron, B12, ferritin- Prescribing Basic Multivitamins1 month after surgery:- Control of iron, B12, albumin- In case of deficiency - parenteral correction3 months after surgery:- Advanced micronutrient control (Fe, Zn, Cu, Mg, Se, B12)- Differentiated prescription of dietary supplements, infusions6 months and beyond:- Dietary control
6. Conclusions
- Bariatric surgery, despite its pronounced effectiveness, is accompanied by the risk of developing microelementoses already in the first months after the intervention. The study showed that systematic laboratory monitoring of the microelement status and early correction of identified deficiencies can prevent the development of complications and improve rehabilitation.And from all of these the following conclusions follow:1. 62.3% of patients develop microelementoses by the 6th month after surgery.2. The most common deficiencies are iron (56%), zinc (41%) and copper (30%).3. Women have an increased risk of deficiencies.4. Refusal of vitamin supplements and protein foods are key risk factors.5. The implementation of early laboratory monitoring protocols is recommended.