-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(8): 2816-2818
doi:10.5923/j.ajmms.20251508.83
Received: Aug. 9, 2025; Accepted: Aug. 27, 2025; Published: Aug. 30, 2025

Gender and Regional Features of Arterial Hypertension and Ischemic Heart Disease
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLAkhmedov A. T.1, Sharipov Zh. R.2
1PhD., Associate Professor, Pediatric Surgery and Neurosurgery, Bukhara State Medical Institute, Bukhara, Uzbekistan
2Head of Department, ICU, Bukhara Branch of Republican Specialized Cardiology Scientific-Practical Medicine Center, Bukhara, Uzbekistan
Correspondence to: Akhmedov A. T., PhD., Associate Professor, Pediatric Surgery and Neurosurgery, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The article presents the results of a comprehensive clinical and laboratory study of 120 patients treated at the Bukhara Regional Cardiology Dispensary. The patients were divided into two groups: with arterial hypertension (Group I) and with ischemic heart disease that developed against the background of arterial hypertension (Group II). The work analyzed sex, place of residence and distribution of body mass index among patients. Significant differences between the groups were revealed, indicating a progressive worsening of cardiovascular disorders with a combination of arterial hypertension and ischemic heart disease. The results obtained can serve as a basis for further studies of the pathogenesis and prognosis of cardiovascular diseases.
Keywords: Arterial hypertension, Ischemic heart disease, Gender characteristics, Body mass index, Place of residence
Cite this paper: Akhmedov A. T., Sharipov Zh. R., Gender and Regional Features of Arterial Hypertension and Ischemic Heart Disease, American Journal of Medicine and Medical Sciences, Vol. 15 No. 8, 2025, pp. 2816-2818. doi: 10.5923/j.ajmms.20251508.83.
1. Introduction
- Cardiovascular diseases (CVD) remain the leading causes of global mortality, annually claiming the lives of more than 18 million people [1,2]. Arterial hypertension (AH) and coronary heart disease (CHD) are the main factors determining the development of critical vascular complications. According to global statistics [3], AH affects over 1.2 billion people, and CHD has been diagnosed in more than 126 million. The combination of these pathologies is especially common in people over 60 years of age, reaching 45–50%, which is associated with the progressive impact of such factors as excess body weight, lipid metabolism disorders, and chronic inflammation [3,4,9].Current approaches to the treatment and prevention of CVD do not fully solve the problem of effective hypertension management: in 35–40% of patients, blood pressure remains above target values, which significantly increases the risk of developing coronary heart disease and other cardiovascular events. Uncontrolled hypertension is associated with an increase in mortality from CVD, reaching 15–20% per decade [5,8]. The transition from isolated hypertension to a combination with coronary heart disease is due to complex processes, including vascular remodeling, microcirculatory disorders, and systemic metabolic shifts, but the detailed mechanisms of this process remain poorly understood [6,7].In this regard, there is a need for studies that will reveal the influence of gender, regional and anthropometric characteristics on the development and course of hypertension and coronary heart disease. Such data can become the basis for improving the methods of early prediction and prevention, which emphasizes the importance of this study.Purpose of the study. to study gender and regional characteristics of arterial hypertension and coronary heart disease.
2. Materials and Methods
- To conduct the study, a comprehensive clinical and laboratory examination of 120 patients who were undergoing inpatient and outpatient treatment at the Bukhara Regional Cardiology Dispensary was conducted. All study participants were carefully selected taking into account the inclusion and exclusion criteria to ensure maximum reliability of the data obtained and exclude the influence of concomitant pathologies. Patients were divided into two main clinical groups depending on the established diagnosis:Group I included 60 patients suffering from hypertension. These patients were diagnosed with primary hypertension, without obvious signs of coronary heart disease, which allowed us to focus on the characteristics of the hypertensive process.Group II consisted of 60 patients with an established diagnosis of coronary heart disease that developed against the background of hypertension. These patients represented a more complex clinical category, since the combination of two diseases significantly worsens the course and prognosis of cardiovascular disorders.The control group consisted of 20 conditionally healthy individuals with no history of chronic cardiovascular diseases, which was confirmed by clinical examination and additional instrumental diagnostic methods.
3. Results and Discussion
- Recent studies have shown that there is a certain difference between men and women in the frequency and severity of coronary heart disease in patients with hypertension. These differences are due to a combination of genetic, hormonal, immunological and vascular factors that can affect the course of the disease and the likelihood of its complications. Despite the active study of this topic, the mechanisms underlying gender differences in the pathogenesis of coronary heart disease remain complex and require additional research for their full understanding.According to clinical observations, men more often suffer from early development of coronary heart disease, which is associated with a greater tendency to dyslipidemia, insulin resistance and aggressive forms of atherosclerosis. At the same time, in women, coronary heart disease often manifests itself at a later age, but is often accompanied by atypical symptoms, which can complicate the timely diagnosis of the disease. Hormonal factors play an important role: estrogens have a protective effect on the vascular system, reducing inflammatory processes and preventing endothelial dysfunction, while in the postmenopausal period, the level of estrogens decreases, which leads to an increased risk of cardiovascular diseases in women.
|

|

|
4. Conclusions
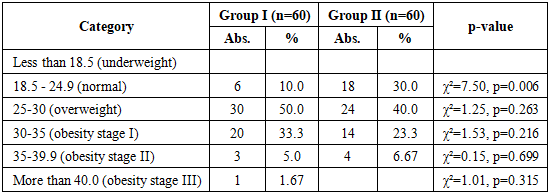
- 1. In patients with isolated hypertension, a significant predominance of women was noted - 61.7%, while among patients with a combination of hypertension and coronary heart disease, the proportion of men was 51.7%. Women were more common in group I (37 out of 60), while men predominated in group II (31 out of 60), but these differences did not reach statistical significance (p=0.144).2. Rural residents predominated among patients with isolated hypertension - 80.0%, while in patients with hypertension and coronary heart disease their proportion was 71.7%. The urban population was more common in group II - 28.3% compared to 20.0% in group I, although the differences did not reach significance (p = 0.292).3. Excess body weight was more often recorded in patients with isolated hypertension - 50.0%, while among patients with a combination of hypertension and coronary heart disease this figure was 40.0%. The proportion of individuals with normal BMI in group II was higher - 30.0% versus 10.0% in group I, which reflects statistically significant differences in the distribution of BMI (p=0.049).