-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(8): 2763-2768
doi:10.5923/j.ajmms.20251508.73
Received: Aug. 8, 2025; Accepted: Aug. 27, 2025; Published: Aug. 30, 2025

Arthroscopic Tenodesis for Traumatic Rupture of the Long Head of the Biceps Brachii: Clinical Outcomes and Surgical Technique
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLIrismetov Murodjon Ergashovich1, Hamroyev Shaxzod Farhodovich2, Shamshimetov Dilshod Fayzaxmatovich3
1Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics of Uzbekistan, Director, Uzbekistan
2Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics of Uzbekistan, Traumatology and Orthopedics Doctor, Uzbekistan
3Republican Specialized Scientific and Practical Medical Center of Traumatology and Orthopedics of Uzbekistan, Head of Sport Trauma Department, Traumatology and Orthopedics Doctor, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Traumatic rupture of the proximal tendon of the long head of the biceps brachii muscle (LHBT) is a clinically significant condition in shoulder pathology, often associated with pre-existing degenerative changes and rotator cuff injuries. While isolated LHBT ruptures are less common, they predominantly affect middle-aged, physically active men and result from sudden eccentric loading of the biceps muscle. Accurate diagnosis and appropriate treatment selection remain challenging, especially in the acute setting. To improve the effectiveness of surgical treatment for LHBT ruptures using a minimally invasive arthroscopic tenodesis technique, aimed at enhancing tendon fixation strength, reducing complications, and accelerating functional recovery. A prospective study was conducted on 25 patients with acute LHBT ruptures treated at the RIIATM clinic between 2022 and 2025. All patients underwent arthroscopic tenodesis using a novel technique involving transosseous fixation with lavsan sutures. The surgical approach was standardized and included specific positioning, arthroscopic identification of the tendon, and transosseous tendon fixation in the proximal bicipital groove. Clinical outcomes were assessed using range of motion (ROM), the University of California Los Angeles (UCLA) shoulder score, the Constant-Murley score, and the Visual Analog Scale (VAS) for pain at baseline, and at 1, 6, and 18 months postoperatively. Postoperative data showed significant improvement in active and passive ROM, particularly in external/internal rotation and abduction. The UCLA score improved from 19.92±0.53 preoperatively to 31.80±0.66 at 18 months. The Constant score increased from 33.52±0.71 to 78.52±0.71, and the VAS score decreased from 5.20±0.24 to 1.24±0.10, indicating substantial pain relief and functional recovery. No major complications were reported. A representative clinical case demonstrated the successful application of the technique, confirmed by imaging and functional recovery. Arthroscopic tenodesis using transosseous suturing is a safe, minimally invasive, and effective method for treating traumatic LHBT ruptures. It offers excellent functional outcomes, pain reduction, and aesthetic advantages, with a lower risk of complications compared to traditional techniques. The results support the use of this technique as a preferred surgical option, especially in active patients with high functional demands.
Keywords: Long head of biceps tendon, Traumatic rupture, Arthroscopic tenodesis, Shoulder injury, Minimally invasive surgery, Transosseous fixation, Functional outcome, Rehabilitation
Cite this paper: Irismetov Murodjon Ergashovich, Hamroyev Shaxzod Farhodovich, Shamshimetov Dilshod Fayzaxmatovich, Arthroscopic Tenodesis for Traumatic Rupture of the Long Head of the Biceps Brachii: Clinical Outcomes and Surgical Technique, American Journal of Medicine and Medical Sciences, Vol. 15 No. 8, 2025, pp. 2763-2768. doi: 10.5923/j.ajmms.20251508.73.
1. Introduction
- Traumatic rupture of the proximal tendon of the long head of the biceps brachii muscle (long head of biceps tendon, LHBT) represents a significant clinical problem in shoulder joint traumatology and orthopedics. Although degenerative changes in the LHBT are often associated with rotator cuff pathology (especially supraspinatus muscle injuries) [1,2], isolated traumatic ruptures of this tendon also occur, albeit less frequently. They typically occur in physically active middle-aged individuals (more often men) as a result of a sudden eccentric contraction of the biceps against significant resistance — when lifting weights, falling on an extended arm, or direct impact on a tensed muscle [3,4].Although the exact prevalence of isolated traumatic LHBT ruptures remains a subject of research, data indicate their substantial proportion among biceps pathologies. Ruptures of the proximal biceps tendon generally account for up to 96% of all biceps ruptures [5]. Isolated LHBT ruptures, according to large retrospective studies, occur with a frequency of approximately 1.2–2.5 cases per 100,000 people per year [6,7]. However, many authors emphasize that these figures may be underestimated due to possible lack of diagnosis or misinterpretation of symptoms [8].The peak incidence occurs at the age of 40–60 years, with ruptures occurring significantly more frequently (7–10 times) in men than in women [6,8]. This is associated with a greater occupational and sports-related load on the shoulder girdle in men of this age group. The main predisposing factor for traumatic rupture, in addition to acute stress, is considered to be pre-existing tendon degeneration ("tendinopathy"), which develops under conditions of chronic microtrauma or impingement [9,10].The clinical picture of acute rupture often includes the characteristic "Popeye sign" — visible distal displacement of the biceps belly, accompanied by acute pain in the anterior shoulder area, crepitation, and subsequent weakness in supination and forearm flexion, especially against resistance [3]. However, diagnosis can be challenging, and the symptoms may be nonspecific, requiring thorough clinical examination and imaging (ultrasound, MRI) [11,12].Modern views on treatment have undergone significant evolution. While open tenodesis was previously widely practiced, today arthroscopic tenodesis using various fixation techniques (interference screws, suture anchors, suspensory fixations) has become the "gold standard" for active patients with high functional demands on the shoulder [13–16]. Conservative treatment is considered an option for elderly patients with low demands or with contraindications to surgery [17]. Recent studies have focused on optimizing surgical techniques, assessing long-term functional outcomes, comparing the effectiveness of various fixation methods [18], as well as studying biomechanics and pathophysiology to better understand risk factors and preventive strategies [19,20].Purpose of the research. Improving the effectiveness of treatment ёof injuries to the long head tendon of the biceps brachii muscle using minimally invasive technologies.
2. Research Materials and Methods
- Arthroscopic tenodesis of the long head tendon of the biceps brachii muscle is a minimally invasive surgical procedure that allows preserving the function of the biceps brachii muscle, reducing the risk of complications, and accelerating the recovery process. This chapter examines in detail the technique of performing the operation, the materials used, fixators, and the criteria for evaluating the effectiveness of treatment.The main goal we sought to achieve was to increase the strength of fixation of the long head of the biceps tendon to the humerus, reduce the degree of injury, and achieve a more favorable aesthetic and plastic result of the operation.Twenty-five patients from this group were treated at the RIIATM clinic in 2022-2025, and the surgical treatment was carried out according to the new methodology we developed.Patients are prepared for surgical intervention after all the aforementioned clinical and instrumental examinations and specialist consultations. In this group of patients, surgical intervention was performed in new cases of tendon rupture.The method was implemented as follows (Fig. 1):The patient undergoes a brachial plexus block and the neck and upper arm area is treated 3 times with a 2% iodine solution. The patient is placed in a semi-recumbent position. The upper arm is abducted up to 70° from the shoulder joint and straightened at the elbow joint. The shoulder is externally rotated, and the forearm is brought to a supination position. The patient's head is turned towards the healthy shoulder.A 2 cm skin incision is made along the anterior surface of the shoulder longitudinally - 1 cm medial to the lateral bicipital groove in the upper third. The deltoid and biceps muscles are retracted laterally. The proximal part of the tendon sheath of the long head of the biceps brachii muscle is exposed. Using an electrosurgical scalpel-coagulator, the synovial part of the bicipital groove is removed. A depression is created in the proximal part of the bicipital groove using a special bone burr.Then, using a trocar, the arthroscope shaft is inserted into the distal part of the tendon through the first skin incision. The arthroscope camera is inserted through its shaft into the bicipital groove in the distal direction, and the distal part of the ruptured tendon is identified. A second longitudinal skin incision 1.0 cm long is made externally over the projection of the long head of the biceps tendon.The tendon stump is externalized and reinforced with lavsan suture, leaving the ends of the threads loose. The free ends of the sutures are inserted into the fibrous sheath through the first skin incision from the distal incision to the proximal incision and brought out. The tendon of the long head of the biceps muscle, brought to the anatomical point, is fixed to the proximal part of the bicipital groove with four transosseous sutures. The strength of the tendon repair is checked by passive extension of the arm at the elbow joint. The surgical wound is closed in layers. The arm is immobilized with a shoulder fixator for 4 weeks.
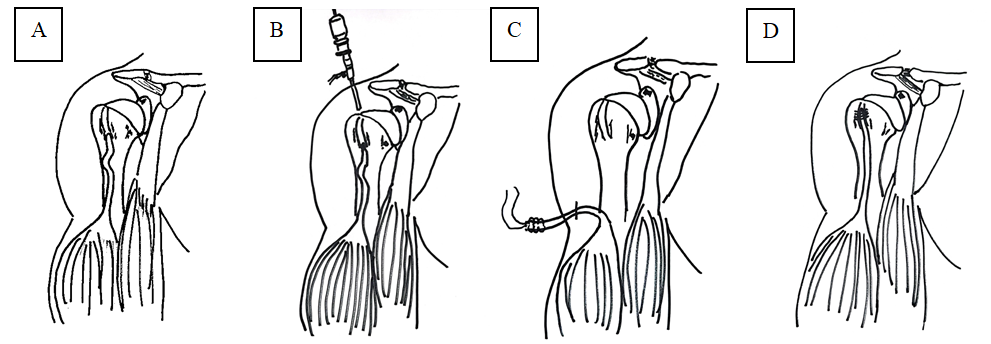 | Figure 1. A. Appearance of the ruptured long head tendon of the biceps brachii muscle before surgery; B. Locating the long head tendon of the biceps brachii muscle using a joint arthroscope; C. Mobilization and fixation of the long head tendon of the biceps brachii muscle; D. Placement of transosseous sutures |
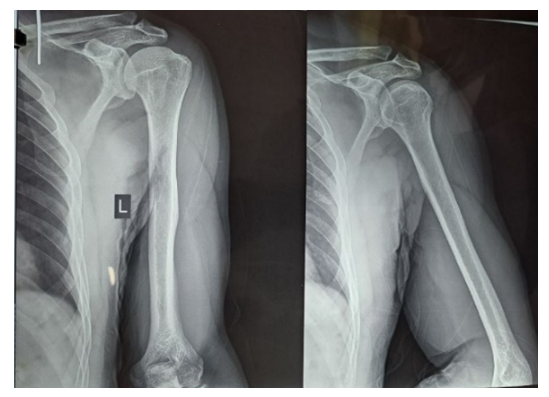 | Figure 2. Patient S.Yu. X-ray analysis |
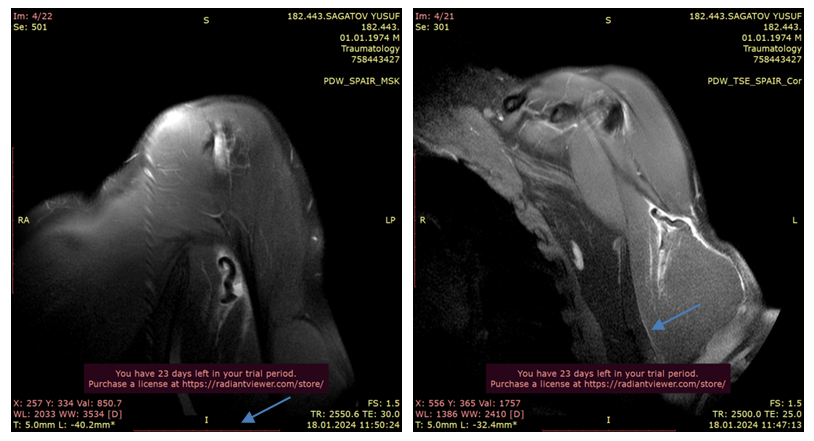 | Figure 3. Patient S.Yu. MRI analysis |
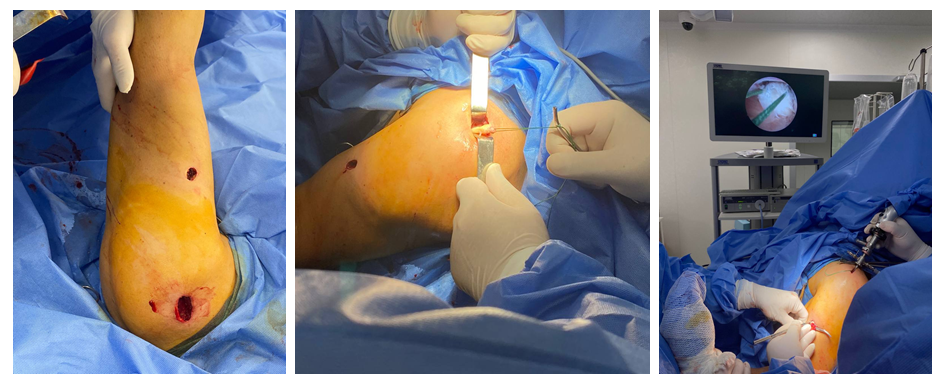 | Figure 4. Patient S.Yu. The process of arthroscope insertion and tendon identification. Transosseous tendon fixation. The image shows the guides, tendon, and lavsan threads used for suturing |
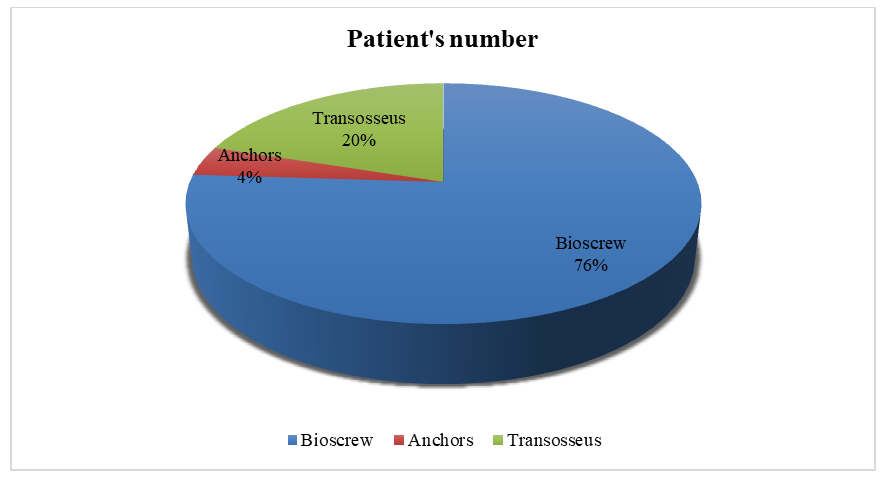 | Diagram 1. Distribution of patients according to the fixation method in arthroscopic tenodesis |
3. Research Results
- Before and 1 month after surgery: The range of motion in all directions remains practically unchanged, which corresponds to the early postoperative period and is maintained due to the immobilization of the patient's arm.After 6 months: Improvement in movement is observed in all directions. For example, active external rotation increases from 56.40° to 65.40°, active internal rotation from 63.20° to 72.00°, and active abduction from 75.20° to 83.00°. A similar trend is observed for passive movements: passive external rotation increases to 75.40°, while passive internal rotation increases to 81.40° or 93.60° depending on the measurement method.After 18 months: the range of motion reached maximum results. For example, active external rotation reaches up to 72.80°, active internal rotation up to 80.80°, and active abduction up to 92.00°. Passive external rotation increases to 84.00°, passive internal rotation to 86.20°, and passive abduction to 102.60°.Active movements (external and internal rotation, abduction) demonstrate steady improvement, indicating enhanced strength and coordination in independently performed movements.Passive movements also improved, indicating a reduction in postoperative limitations and successful tissue recovery. An increase in the range of passive internal rotation was especially pronounced (from 85.60° to 102.60°).The absence of changes in the first month after surgery indicates the standard period of immobilization and early recovery. Improvements after 6 months confirm the effectiveness of the rehabilitation course and the positive effect of surgical intervention on restoring functional mobility. A further increase in the range of motion by 18 months indicates the stability and long-term nature of the achieved results, which is of crucial importance for the clinical prognosis and quality of life of patients.The University of California Shoulder Evaluation Scale before surgery and 1 month after: the average value was 19.92±0.53, indicating significant impairment of shoulder joint function and a high degree of pain syndrome. The absence of changes in the initial postoperative stage (1 month) is associated with the immobilization period and initial tissue healing. After 6 months: the average value increased to 22.20±0.48, indicating signs of joint function recovery, a decrease in pain syndrome, and improved activity. After 18 months: the indicators dynamically increased to 31.80±0.66, demonstrating stable recovery of indicators and initial effectiveness of the surgical intervention.On the Constant Shoulder Scale before surgery and 1 month after: the score was 33.52±0.71, indicating a poor functional state of the shoulder joint. After 6 months: a consistent increase to 48.52±0.71 was observed, with improvements noted in all aspects of shoulder function (pain, strength, mobility), effects of active rehabilitation, and restoration of postoperative results. After 18 months: a gradual increase to 78.52±0.71 was observed, allowing for nearly complete restoration of joint function and demonstrating the effectiveness of arthroscopic tenodesis and a high-quality rehabilitation program.The VAS scale before surgery and 1 month after: the pain level according to VAS was 5.20±0.24, indicating pronounced severity of pain syndrome in patients. After 6 months: a decrease in pain to 2.40±0.16 reflects reduced pain sensations associated with tissue regeneration and decreased inflammation. After 18 months: when the pain syndrome was almost completely eliminated and patients achieved a high level of comfort, a consistent decrease to 1.24±0.10 points was observed.
4. Conclusions
- Comparative analysis of the dynamics of functional indicators and range of motion in patients who underwent arthroscopic tenodesis showed a significant and stable improvement in the condition of the shoulder joint in both short and long-term perspectives. The assessment results according to the UCLA and Constant Shoulder Score scales noted a significant increase in joint function: from low preoperative indicators to high indicators at 18 months after surgery, which indicates a qualitative restoration of activity, strength, and mobility. At the same time, the decrease in VAS test values indicates that the pain syndrome has been significantly alleviated.Analysis of the range of motion (active and passive indicators of external and internal rotation, abduction) also confirms positive dynamics: in the early postoperative period, with minimal changes, a significant expansion of the range of motion is observed by 6 and 18 months. These data collectively demonstrate the high effectiveness of arthroscopic tenodesis and confirm that a comprehensive postoperative rehabilitation course contributes to the stable and long-term restoration of shoulder joint functions.Thus, the obtained results serve as a reliable justification for the choice of this method, ensure an improvement in clinical and functional indicators, which positively affects the quality of life of patients.Compared to other methods, arthroscope-assisted tenodesis has the following advantages:• Minimal invasiveness: reduced tissue damage, lower risk of blood loss and postoperative scarring.• Cosmetic result: Small incisions provide the best aesthetic appearance.• Precision: ability to visualize structures and accurately secure the tendon.• Reduced risk of complications: Lower probability of nerve damage (e.g., n. musculocutaneus).• Quick recovery: Patients return to their daily activities faster.Despite its advantages, the method requires high surgical skill during the procedure. Additionally, in older injuries, the use of the arthroscope device is challenging due to the fact that after tendon retraction, the surrounding area is covered with scar tissue.