-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(8): 2731-2733
doi:10.5923/j.ajmms.20251508.65
Received: Aug. 5, 2025; Accepted: Aug. 27, 2025; Published: Aug. 30, 2025

The Role of Healthcare Professionals in the Prevention of Dental Diseases: A Case Study of Pubertal Girls
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLKuryazov Shoxrux Akbarovich, Kuryazov Akbar Kuramboyevich, Khabibova Nazira Nasulloevna
Bukhara State Medical Institute named after Abu Ali ibn Sina, Bukhara, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

This article presents a study on the role of healthcare professionals, particularly dentists, in the primary prevention of dental diseases among pubertal girls aged 13–17. Based on surveys and interviews with 119 dentists and 570 adolescent girls, the article examines the prevalence of key dental conditions in this age group, including periodontitis, pulpitis, and lesions of hard dental tissues. It also analyzes the professionals’ perspectives on preventive practices and the effectiveness of various intervention formats. Findings highlight a low level of actual preventive coverage among adolescent girls, despite timely dental service utilization. The study reveals differences between dentists’ and girls’ preferences for communication methods, underlining the need for targeted, age-appropriate prevention programs.
Keywords: Dental diseases, Primary prevention, Pubertal girls, Healthcare professionals, Risk factors, Social media, Dental education
Cite this paper: Kuryazov Shoxrux Akbarovich, Kuryazov Akbar Kuramboyevich, Khabibova Nazira Nasulloevna, The Role of Healthcare Professionals in the Prevention of Dental Diseases: A Case Study of Pubertal Girls, American Journal of Medicine and Medical Sciences, Vol. 15 No. 8, 2025, pp. 2731-2733. doi: 10.5923/j.ajmms.20251508.65.
1. Introduction
- The promotion of oral health in adolescence is a key aspect of general health care. Pubertal girls, aged 13–17, undergo significant hormonal, psychological, and social changes that can influence their susceptibility to dental diseases. While treatment remains an essential component of dental care, the focus on primary prevention is increasingly recognized as a cost-effective and sustainable strategy. Primary prevention aims to reduce the incidence of disease before clinical symptoms appear, through health education, early intervention, and risk factor control [1,3,4].Despite widespread acknowledgment of the importance of dental prevention, there is limited research on how effectively healthcare professionals apply preventive strategies among adolescents, particularly pubertal girls. This study seeks to fill this gap by exploring both the prevalence of dental diseases in this group and the actual involvement of dental practitioners in preventive efforts [4,5].
2. Materials and Methods
- The study employed a cross-sectional design using quantitative and qualitative methods. A total of 119 dentists from both public (n=67) and private (n=52) dental clinics were surveyed. Participants included 70 men (58.82%) and 49 women (41.18%). The majority (64.70%) were aged between 21 and 35, while 28.57% were aged 36–60, and 6.72% were over 60. Work experience ranged from less than 5 years (49.57%) to more than 20 years (20.16%).In addition, 570 pubertal girls aged 13–17 were interviewed regarding their oral health awareness and views on preventive education. The study examined not only disease prevalence but also the extent of exposure to preventive dental activities and the communication formats preferred by both professionals and patients.Statistical analysis included descriptive statistics and comparative evaluations using the chi-square test. Differences with a p-value of less than 0.05 were considered statistically significant.
3. Results and Discussion
- The findings revealed that the most common diagnoses among pubertal girls seeking dental care were periodontitis (80.67%), pulpitis (78.99%), and hard tissue lesions (77.31%). Despite the high disease burden, 90.70% of dentists noted that these girls typically sought care on time, in contrast to the general population, where timely visits occurred in only 53.78% of cases.However, the extent of participation in primary prevention activities was markedly low. Only 4.47% of adolescent girls in public clinics and 2.84% in private clinics had received any form of preventive intervention. Among public dentists, 38.80% reported conducting preventive work, compared to just 15.38% in the private sector.Dentists reported using various communication formats: individual consultations (public: 20.89%, private: 23.07%), social media and publications (29.85% and 25.00%, respectively), seminars and round-table discussions (less than 5% in both sectors), and handouts (14.92% and 11.53%). Notably, over 26% of dentists in both groups expressed uncertainty about which preventive methods to use.Figure 1 presents a comparative analysis of the timeliness of dental service utilization between the general population and pubertal girls aged 13–17. The blue columns represent the percentage of individuals who sought dental care on time, while the orange columns reflect delayed consultations.
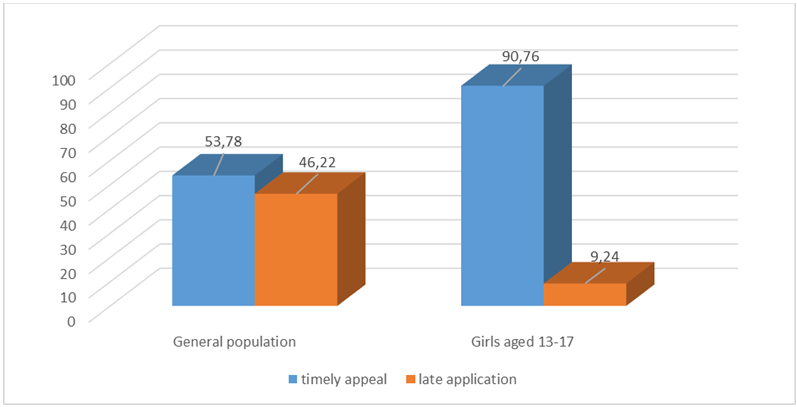 | Figure 1. Comparative indicators of timely referral of patients to specialists for dental services, % |
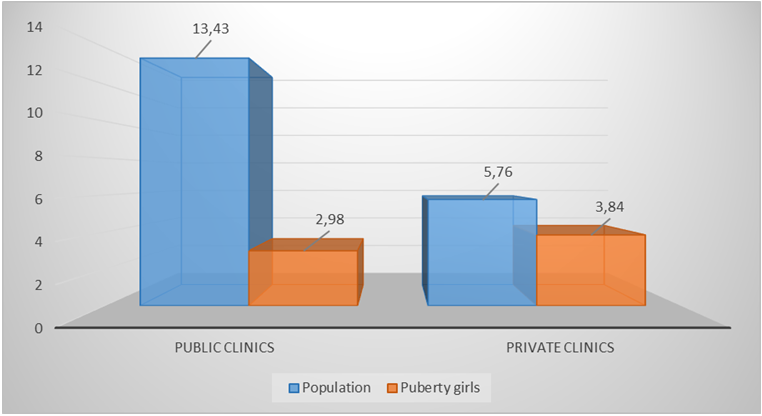 | Figure 2. Indicators of official appeals to specialists for primary prevention of dental diseases, % |
4. Conclusions
- The study underscores the need for more structured and targeted dental prevention strategies among pubertal girls. Although many of them show good awareness and make timely visits, only a small fraction benefit from organized preventive care. Disparities between the views of healthcare professionals and adolescents highlight the necessity of involving the target population in designing effective prevention tools.To increase the efficiency of primary prevention, interventions should focus on the most acknowledged communication methods — particularly social media and one-on-one consultations. Greater integration of dental education into schools and community programs, supported by healthcare systems and policies, can help mitigate the rising burden of dental disease in this vulnerable group.