-
Paper Information
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(8): 2598-2602
doi:10.5923/j.ajmms.20251508.38
Received: Jul. 6, 2025; Accepted: Aug. 3, 2025; Published: Aug. 6, 2025

Clinical Assessment and Treatment of Changes in the Occlusal Surface of the Dentition in Children
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLRuzieva Gavkhar Tokhirovna
Bukhara State Medical Institute, Uzbekistan
Correspondence to: Ruzieva Gavkhar Tokhirovna, Bukhara State Medical Institute, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Introduction: Diagnosis, treatment, and prevention of dental and jaw anomalies is one of the urgent tasks in modern orthodontics. As a result of dental and jaw anomalies, functions such as food intake and chewing are disrupted, children may mispronounce words, and cosmetic appearance is affected. Studying the prevalence of dental and jaw anomalies and deformities, as well as the effectiveness of their treatment, is an important issue. Among dental diseases, dental and jaw anomalies rank third in terms of occurrence and prevalence, following dental caries and periodontal diseases. Methods: Violations of occlusion of the dentition in children: violation of the central symmetry of the teeth - in 12 children (10%), infraocclusion - in 24 children (20%), supraocclusion - in 18 children (15%), secondary adentia - in 20 children (16.67%). The prevalence of dental caries in children aged 10–18 years averaged 68.7%. The highest rate of physiological growth in facial height in boys and girls was observed between the ages of 14 and 18 years. Conclusion- according to the results of the study, it was found that the deformations of the dental rows increase in direct proportion to the age group of children. Occlusal disorders of the dental rows in children - violation of the symmetry of the central teeth - were observed in 12 children (10%), infraocclusion in 24 children (20%), supraocclusion in 18 children (15%), and secondary edentulism in 20 children (16.67%). The average prevalence of dental caries in children aged 10-18 was 68.7%. In this case, the prevalence of dental caries in 10-year-old children was 63.5% on average. at the age of 13 - 62.7%; At the age of 15 - 47.8%, at the age of 18 - 41.4% (r<0.001), the greatest increase in the prevalence of caries was observed in children aged 10 to 13 years.
Keywords: Anomalies and deformations, Occlusal surface, Oral cavity
Cite this paper: Ruzieva Gavkhar Tokhirovna, Clinical Assessment and Treatment of Changes in the Occlusal Surface of the Dentition in Children, American Journal of Medicine and Medical Sciences, Vol. 15 No. 8, 2025, pp. 2598-2602. doi: 10.5923/j.ajmms.20251508.38.
1. Introduction
- During the period of mixed dentition, the dental-jaw system is in the phase of growth and formation, so anomalies and deformities addressed in a timely manner will lead to the normalization of growth later on. All the above confirms the need for a new approach in diagnosing, treating, and preventing anomalies and deformities in the dental-jaw system, which arise due to changes in the occlusal plane of children’s dental arches. In our scientific research, we conducted dental examinations among 155 children aged 10 to 18. Among them, 120 children had deformities in the occlusal plane of their dental arches, and 35 children were healthy (see Figure 1). They had come to the "Dental Center" of the Bukhara State Medical Institute for treatment. Patient histories were collected and analyzed, their views on the onset and development of the condition were heard, and a detailed objective examination was carried out.
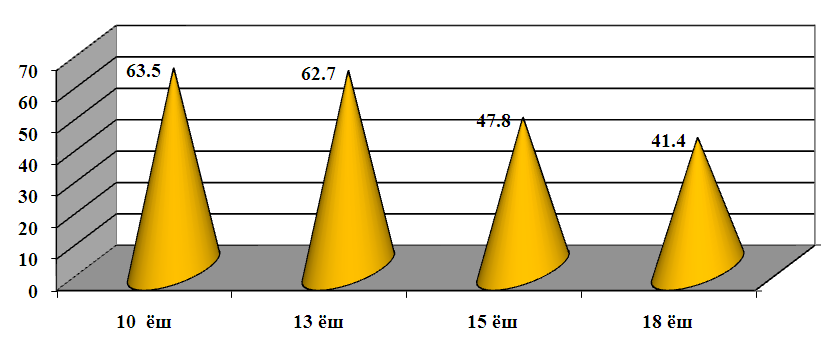 | Figure 1. Prevalence of permanent tooth caries in children aged 10 to 18 years (%) |
2. Methodology
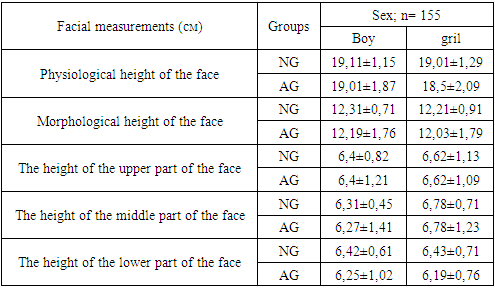
- 155 children aged 10-18 were examined. 1. Children with deformities in the occlusal plane of their dental arches (120 children)2. Children with normal occlusion (35 children)57 of the examined children were girls and 63 were boys. All the examined children were grouped into age categories based on the stages of occlusion development according to D.A. Calvelis:• Group 1 – Late mixed dentition period (10-13 years), consisting of 52 children (28 boys and 24 girls);• Group 2 – Permanent dentition period (14-18 years), consisting of 68 children (36 boys and 32 girls).In the main group, we identified local and general etiological and pathogenetic factors leading to supraocclusion, infraocclusion, and tooth loss in the dental arches. Special attention was given to analyzing the age at which the children lost teeth and the resulting morphological and functional changes.The dental examination and inspection were conducted using a generally accepted standard set of dental instruments, including a survey, patient complaints, objective examination, inspection of the oral mucosa, teeth and dental arches, periodontal tissues, chewing muscles, and the temporomandibular joint. Previous orthodontic treatment, surgery in the facial-jaw area, and the patient’s complaints were also identified. [1,3,5]During the clinical examination, a medical history was collected, and attention was paid to the presence or absence of local and general systemic diseases, as well as salivation. During the tooth inspection, the color, size, position, presence of decayed or broken teeth, sensitivity changes, mobility, and the condition of the alveolar bone in the location of missing teeth were noted. The movements of the lower jaw in vertical, transverse, and sagittal directions were evaluated. The functional aspect of the diagnosis included dynamic tests (breathing, speech, swallowing). Clinical functional tests according to Ilyina-Markosyan were carried out. The orthodontic diagnosis was made according to D.A. Calvelis’ classifications. In facial and head anthropometric examination, several points and landmarks exist [2,7]. In our scientific research, we used several of them. Facial type – According to the classification of Garson and Kollman, there are three types of face: broad, medium, and long [4,6].To determine the facial type, we identified two parameters: 1) the height of the face from the front and 2) the width of the face between the cheekbones, which we measured using a caliper. In our scientific work, to achieve our objective, it is possible to qualitatively determine the facial profile type without using a patient photo. The face was classified as straight, concave, or convex. To determine the facial profile type, we used a flat rectangular colorless plate (15 x 5 cm). Analysis of the models was carried out according to the methodology of O.J. Nazarov (2010). Radiographic examination methods – Among functional examinations of teeth, jaw, and temporomandibular joint, radiographic examination plays a key role. Our examinations using the orthopantomogram (OPG) showed that the condition of the upper and lower dental arches, occlusion relationships, and the sequence of tooth eruption were analyzed in the main group of patients. Cephalometric radiography – In this radiographic method, the examination is initially performed from a considerable distance (approximately 1.5 meters). In such an examination, the X-rays are directed parallel to each other, which minimizes projection distortions and shows the object in its minimal state. As a result, it is possible to obtain a full-sized image of the head and neck, which is an advantage of this research method. Currently, there is a technique to convert a three-dimensional image into a two-dimensional one. [8]Cephalometric radiography can be performed in two projections: lateral (sagittal) and direct anterior (frontal). The lateral cephalogram allows for a clear assessment of the jaw’s relationships. We analyzed the cephalometric radiographs using the Schwarz, Downs, and Tweed methods. Schwarz's method uses points located on the cranial base (anterior part) as landmarks. For studying the cephalometric radiograph according to Schwarz, the following points are considered fundamental: Se (Sella), N (Nasion), Or (Orbitale), Sna (Spina nasalis anterior), Snp (Spina nasalis posterior), Po (Porion), Ss (Apoint), Sn (Subnasale), Spm (Bpoint), Pg (Pogonion), Go (Gonion), Gen (Gnation). The A-point is the subspinal point, the deepest point on the upper jaw's apical base, while the B-point is the supramental point, the deepest point on the lower jaw's apical base. The statistical analysis of the results was conducted using the Statistica software package for Windows 7.0 and the EXCEL-2007 program. The distribution parameters of the analyzed features are presented in the form of the mean (M ± m) and the standard deviation. To compare the means of more than one group, multiple comparison methods were used (Newman-Keuls); for comparing multiple groups, the Student t-test was applied. The Spearman correlation coefficient was calculated. A difference between groups was considered statistically significant at p < 0.05.
3. Results
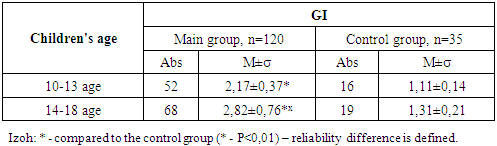
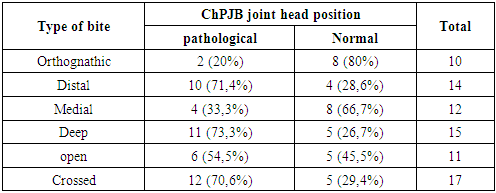
- The types of occlusal disorders in children’s dental arches and their prevalence rates are shown in. The symmetry of the central incisors was disrupted in 11 children (9.6%), and infraocclusion was observed in 24 children (21%). In the main group of children, the primary causes of tooth loss were identified as dental caries and its complications, according to the medical histories collected from the children and their parents. Based on the research conducted and the medical histories gathered from the children and their parents, we can state that 85-90% of children do not know about the eruption of the first permanent molar at the age of 6.5–7 years. As a result, during the early mixed dentition period, milk teeth (deciduous teeth) are affected by caries. Consequently, due to the complications of caries, permanent teeth are also extracted. In the main group of children, caries is widely spread on the chewing surfaces of the molars, particularly in the natural fissures. Caries lesions were detected in the cervical part of the frontal teeth. The examinations showed that the prevalence of dental caries in 10-year-old children was 63.5% on average. In 13-year-olds, it was 62.7%; in 15-year-olds, it was 47.8%, and in 18-year-olds, it was 41.4% (p < 0.001). The data presented in indicates that the highest increase in the spread of caries was observed in children between 10 to 13 years old. In this group, the intensity of the caries process in permanent teeth was 2.41 ± 0.12 on average. The caries intensity of permanent teeth in 18-year-olds was 2.55 ± 0.02. A comparative analysis of the spread of caries in permanent teeth was conducted for children aged 13 to 18 in the main group. In our study, the average spread of the caries process in the main group of.In the main group of children, the hygiene index for the 14–18-year-old group was the highest, reaching 2.82. The data presented in Table 1 shows that the initial oral hygiene condition was poor in children from the main group who were planned for comprehensive treatment. In the main group, dental calculus was detected in 71.4% of the children.
|
|
|
4. Conclusions
- according to the results of the study, it was found that the deformations of the dental rows increase in direct proportion to the age group of children. Occlusal disorders of the dental rows in children - violation of the symmetry of the central teeth - were observed in 12 children (10%), infraocclusion in 24 children (20%), supraocclusion in 18 children (15%), and secondary edentulism in 20 children (16.67%).The average prevalence of dental caries in children aged 10-18 was 68.7%. In this case, the prevalence of dental caries in 10-year-old children was 63.5% on average. at the age of 13 - 62.7%; At the age of 15 - 47.8%, at the age of 18 - 41.4% (r<0.001), the greatest increase in the prevalence of caries was observed in children aged 10 to 13 years.It was found that it is possible to assess normal or pathological facial growth processes in children using anthropometric measurements. The highest rate of growth in physiological facial height in children with deformities caused by the loss of molar teeth was observed in the main group of children aged 14-18 years. The highest rate of growth in physiological facial height in boys and girls was found in the age group of 14-18 years. Late replacement bite - 10-13 years old: use of myofunctional caps to normalize the relationship of the jaws, as well as caps to normalize the myobridges and occlusal level, replacing lost teeth with acetal microprostheses.Permanent bite - 14-18 years: the use of non-removable mechanical impact (braces) orthodontic devices to ensure the relationship of the jaws, the clinching of antagonistic teeth in a normal position and caps to normalize the occlusion level, replacing lost teeth with acetal microprostheses, compared to the basic treatment, a 93.4% positive result was achieved.