-
Paper Information
- Next Paper
- Previous Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(8): 2444-2448
doi:10.5923/j.ajmms.20251508.04
Received: Jun. 22, 2025; Accepted: Jul. 20, 2025; Published: Aug. 2, 2025

Effect of Integrated Versus Traditional Dental Management in Pregnant Women Diagnosed with Preeclampsia
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLShukrullayeva G. J.
Basic Doctoral Student, Bukhara State Medical Institute, Bukhara, Uzbekistan
Correspondence to: Shukrullayeva G. J., Basic Doctoral Student, Bukhara State Medical Institute, Bukhara, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Preeclampsia (PE) is associated with systemic inflammatory responses that can exacerbate periodontal disease. This study aimed to evaluate the effectiveness of comprehensive versus conventional periodontal treatment in pregnant women with PE and to assess its impact on oral health indices. A total of 60 pregnant women with PE (main group) were divided into two subgroups: Subgroup I (n=37) received comprehensive periodontal treatment including hydromassage, while Subgroup II (n=23) received only conventional therapy. An additional comparison group of physiologically pregnant women with periodontal inflammation (n=40) received conventional treatment. DMF index and periodontal indices (PMA, PBI, OHI-S, and CPI) were assessed on days 3 and 7 of treatment. The DMF index was significantly higher in the main group (15.53 ± 0.23) compared to the comparison group (12.07 ± 0.20). Subgroup I showed the most significant improvement across all periodontal indices: by day 7, PMA decreased to 22.56 ± 1.85, PBI to 1.56 ± 0.14, OHI-S to 1.31 ± 0.09, and CPI to 1.96 ± 0.11. In Subgroup II, although initial improvement was observed, indices showed regression over time, indicating limited long-term efficacy of conventional treatment. The comparison group had moderate improvements, while the untreated control group showed no significant changes. Comprehensive periodontal therapy, including hydromassage, demonstrated superior effectiveness in improving and sustaining periodontal health in pregnant women with PE. These findings highlight the need for an individualized, multidisciplinary approach in managing oral health during high-risk pregnancies.
Keywords: Preeclampsia, Pregnancy, Periodontal indexes, Caries index (DMFT), Oral hygiene index (OHI-S), Gingival index (PMA), Sulcus bleeding index (SBI), Community Periodontal Index of Treatment Needs (CPITN)
Cite this paper: Shukrullayeva G. J., Effect of Integrated Versus Traditional Dental Management in Pregnant Women Diagnosed with Preeclampsia, American Journal of Medicine and Medical Sciences, Vol. 15 No. 8, 2025, pp. 2444-2448. doi: 10.5923/j.ajmms.20251508.04.
1. Introduction
- Preeclampsia is a pregnancy-specific, multisystem disorder that poses serious health risks to both the mother and fetus. It typically occurs after the 20th week of gestation and is characterized by elevated blood pressure (≥140/90 mmHg) and proteinuria (≥300 mg/24 h), often accompanied by systemic vasospasm, activation of coagulation pathways, and impaired perfusion of vital organs, including the kidneys, liver, brain, and placenta. These pathological processes may lead to severe maternal and fetal complications, including mortality [1,6,9].Despite numerous studies, the exact etiology of preeclampsia remains unknown, and it is considered a complex, multifactorial condition. In developed countries, the prevalence of preeclampsia ranges between 2% and 5% of pregnancies [2,4], whereas in developing nations it exceeds 10%, contributing significantly to maternal mortality [3,10].Recent research suggests a notable association between periodontal disease and preeclampsia. Studies have found that 20–50% of pregnant women experience periodontal pathology, with a higher incidence among socioeconomically disadvantaged populations [5,11]. Chronic inflammation of the periodontal tissues is increasingly being recognized as a potential risk factor for the onset or worsening of preeclampsia [7,10]. Conversely, preeclampsia may exacerbate periodontal conditions by compromising the immune response and gingival tissue integrity due to increased systemic inflammation and the presence of pathogenic bacterial biofilms dominated by Gram-negative anaerobes [8].Given the bidirectional relationship between preeclampsia and periodontal disease, it is crucial to explore effective treatment strategies aimed at improving oral health outcomes in pregnant women with preeclampsia. Furthermore, enhancing preventive and therapeutic approaches to periodontal care in this population may contribute to improved maternal and fetal prognosis. Therefore, the current study aims to evaluate dental indicators before and after conventional and comprehensive treatment in pregnant women diagnosed with preeclampsia.This study aims to enhance the therapeutic and preventive approaches to managing periodontal diseases in pregnant women affected by preeclampsia.Research Objectives:- To study the prevalence of periodontal diseases in pregnant women diagnosed with preeclampsia.- To assess the role of vascular permeability in the development of periodontal tissue diseases in preeclamptic pregnant women using functional diagnostic methods.- To investigate changes in key blood parameters (mineral and hormonal spectra) contributing to the progression of periodontal diseases in patients with pregnancy-associated preeclampsia.- To evaluate the effectiveness of comprehensive treatment methods for periodontal diseases developed in collaboration with specialists, and to develop clinical recommendations for their application in pregnant women with preeclampsia.
2. Materials and Methods
- This scientific study was conducted during the years 2024–2025 at the Bukhara State Medical Institute and the Bukhara Regional Branch of the Republican Specialized Scientific and Practical Medical Center for Mother and Child Health. A total of 120 pregnant women aged between 18 and 44 years were enrolled and underwent clinical, functional, and laboratory examinations. In addition, 20 non-pregnant women were examined as a control group.The participants were divided into three groups:Main group (n = 60): Pregnant women in the third trimester diagnosed with preeclampsia.Comparison group (n = 40): Pregnant women with physiologically normal pregnancies.Control group (n = 20): Non-pregnant women of reproductive age.Patient data were analyzed based on medical histories, discharge summaries, and outpatient records. Clinical examinations were conducted on the study participants, including subjective assessments, objective findings, and additional diagnostic methods.All reproductive-aged participants were also categorized into three subgroups according to age, based on the STRAW+10 (Stages of Reproductive Aging Workshop) criteria:• 18–24 years;• 25–34 years;• 35–44 years.Clinical ExaminationThe clinical examination began with an external inspection of the face. Particular attention was paid to facial asymmetry, the general appearance of the patient, and the presence of lesions or swelling on the vermilion border of the lips. Additionally, the color and condition of the hair and nails, swelling or discoloration of the skin and mucous membranes were assessed.The examination of the tongue focused on the condition of the lingual papillae and the presence of any coating. When inspecting the oral vestibule and cheeks, special attention was given to the moisture and color of the oral mucosa, as well as the presence of dental impressions on the mucosal surface. During the intraoral examination, the presence of dental caries and its complications, as well as existing dental fillings, were recorded.Dental assessments were carried out using the following indices:Caries index (DMFT) – according to the method of Klein and Palmer (1939) for permanent teeth;Oral Hygiene Index – Simplified (OHI-S) – by J.C. Green and J.R. Vermillion (1964);Gingival index (PMA) – using the Parma modification (1960) to assess gingivitis;Sulcus Bleeding Index (SBI) – according to H.R. Muhlemann (1971) to evaluate gingival bleeding;Community Periodontal Index of Treatment Needs (CPITN) – to determine the periodontal status and the need for periodontal treatment.
3. Results
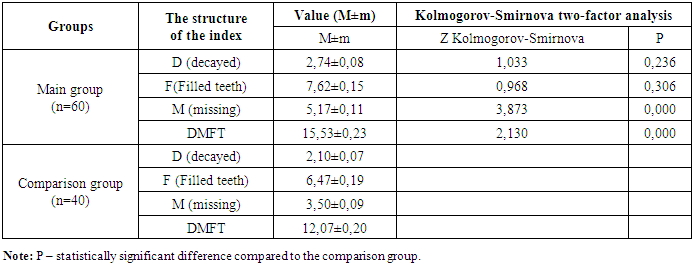
- To evaluate the condition of hard dental tissues, the Decayed, Missing, and Filled Teeth (DMFT) index was used. The DMFT index reflected a high prevalence of dental caries and its complications in both the comparison group and the main group. This indicates a significant burden of carious lesions in these populations.The DMFT index values obtained from the study groups are presented in Table 1.
|
|
|
|
4. Discussion
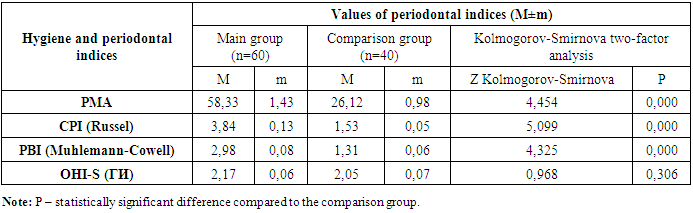
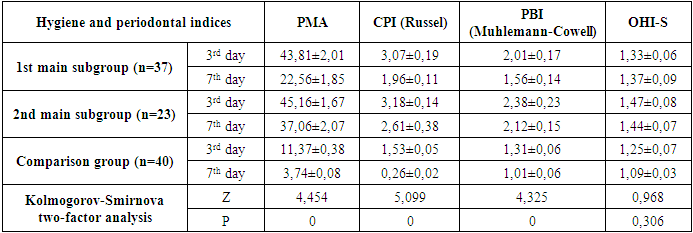
- According to the data presented in Table 1, the average DMF (Decayed, Missing, Filled) index among pregnant women with preeclampsia (main group) was 15.53 ± 0.23, whereas in the comparison group with physiological pregnancy, the index was 12.07 ± 0.20.When analyzing the average values of the decayed (D), filled (F), and missing (M) components in both research groups, significant differences were observed. In particular, the average number of decayed teeth in the main group was 2.74±0.08, compared to 2.10±0.07 in the comparison group.It is important to note that these values were obtained without including carious lesions at the spot (initial) stage. If such early-stage lesions were also taken into account, the indicator in the main group would be expected to be even higher.Regarding filled teeth, the average was 7.62 ± 0.15 in the main group and 6.47 ± 0.19 in the comparison group. As for the number of extracted (missing) teeth, a significant difference was identified between the groups: an average of 5.17 ± 0.11 teeth were extracted in the main group, compared to 3.50 ± 0.09 in the comparison group.Significant dynamics of periodontal condition improvement were observed in both the main and comparison groups as a result of treatment. Notably, although periodontal indices improved in Subgroup II of the main group—pregnant women with preeclampsia (PE) who received conventional treatment—these improvements did not reach the values observed in the physiologically pregnant women of the comparison group.In Subgroup II of the main group, the PMA index decreased from 58.33 ± 1.43 on the 3rd day of treatment to 45.16 ± 1.67, and to 37.06 ± 2.07 by the 7th day. The PBI index dropped from 2.98 ± 0.08 on day 3 to 2.38 ± 0.23, and to 2.12 ± 0.15 by day 7. The OHI-S hygiene index improved from 2.17 ± 0.06 on day 3 to 1.47 ± 0.08, and to 1.44 ± 0.07 on day 7. Changes in the CPI index were observed from 3.84 ± 0.13 on day 3 to 3.18 ± 0.14, and 2.61 ± 0.38 on day 7.In the comparison group of physiologically pregnant women with periodontal inflammation, the respective indices improved to 11.37 ± 0.38, 1.31 ± 0.06, 1.25 ± 0.07, and 1.53 ± 0.05 on day 3, and to 3.74 ± 0.08, 1.01 ± 0.06, 1.09 ± 0.03, and 0.26 ± 0.02 on day 7.These findings suggest that conventional treatment is less effective in patients with PE, indicating the need for a more individualized approach in their treatment.Importantly, Subgroup I of the main group, which received comprehensive treatment, showed significantly better results. The PMA index dropped to 43.81 ± 2.01 by day 3 and to 22.56 ± 1.85 by day 7. The PBI index decreased to 2.01 ± 0.17 by day 3 and 1.56 ± 0.14 by day 7. The OHI-S index improved to 1.33 ± 0.06 on day 3 and 1.31 ± 0.09 on day 7. The CPI index changed to 3.07 ± 0.19 on day 3 and to 1.96 ± 0.11 on day 7.These results highlight the advantages of a comprehensive approach in treating periodontal disease in patients with PE, showing significant improvement in periodontal status and higher oral hygiene levels compared to Subgroup II.The untreated control group showed stability in index values, indicating a lack of dynamic change in their periodontal condition.In Subgroup II of the main group, the PMA, PBI, OHI-S, and CPI indices increased again, likely due to the limited long-term effectiveness of conventional treatment, particularly in patients with PE. Despite initial improvements, the comparison group also showed a return to previous values. The untreated control group remained unchanged.Treatment effectiveness was evaluated on days 3 and 7 through surveys and clinical-laboratory examinations. Seven days after treatment completion, changes in periodontal condition varied among groups. In Subgroup I of the main group, where comprehensive treatment was used, the indices remained consistently at improved levels, demonstrating that comprehensive therapy helps consolidate long-term positive outcomes.Statistical significance was confirmed at p < 0.005.
5. Conclusions
- The conducted study reveals that pregnant women with preeclampsia (PE) demonstrate a significantly higher DMF (Decayed, Missing, Filled) index compared to physiologically pregnant women, indicating a more severe level of dental caries and tooth loss. Notably, the average number of decayed, filled, and missing teeth was substantially higher in the main group, emphasizing the negative impact of PE on oral health.The results of periodontal treatment also varied markedly between the groups. While both conventional and comprehensive treatment approaches led to improvements in periodontal indices, the most pronounced and stable improvements were observed in the subgroup that received comprehensive treatment. These patients showed significant reductions in PMA, PBI, OHI-S, and CPI indices by day 7, suggesting enhanced gingival health, reduced bleeding, improved oral hygiene, and better overall periodontal condition.In contrast, patients receiving only conventional therapy showed temporary improvement, with a trend toward regression in the post-treatment period. The untreated control group exhibited no meaningful change in periodontal status.Thus, the data strongly support the superiority of comprehensive periodontal treatment in pregnant women with PE, both in terms of effectiveness and the sustainability of results. The limited efficacy of conventional therapy underscores the importance of individualized, multifactorial approaches in managing periodontal disease among high-risk pregnant populations.These findings justify the inclusion of comprehensive periodontal care as part of the multidisciplinary management strategy for pregnant women with preeclampsia, which may also contribute to improved systemic and perinatal outcomes.