-
Paper Information
- Next Paper
- Paper Submission
-
Journal Information
- About This Journal
- Editorial Board
- Current Issue
- Archive
- Author Guidelines
- Contact Us
American Journal of Medicine and Medical Sciences
p-ISSN: 2165-901X e-ISSN: 2165-9036
2025; 15(7): 2164-2169
doi:10.5923/j.ajmms.20251507.16
Received: Jun. 17, 2025; Accepted: Jul. 8, 2025; Published: Jul. 11, 2025

Evaluation of Patients' Life Quality in Urologic and Andrologic Complications in Recipients after Kidney Transplantation
 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTMLS. S. Kariev, F. R. Nasirov
Republican Specialized Scientific and Practical Medical Center of Urology, Tashkent, Uzbekistan
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

The aim of the study was to evaluate the life quality of recipients with urologic complications after related kidney transplantation. Background. About two-thirds of people with chronic kidney disease receive hemodialysis, a quarter of patients have a kidney transplantation, and one-tenth receive peritoneal dialysis. Kidney transplantation is considered a superior method to chronic dialysis because it prolongs survival and alleviates uremic symptoms. Material and Methods. A five-month analytical study was conducted. A total of 78 kidney transplant recipients’ data for the past three years were collected. Data were collected using the WHOQOL-BREF questionnaire, which contained 25 questions focused on four domains (physical, psychological, social and environmental). Results. A questionnaire of 78 patients (mean age made up 36.1±9.2 years) was conducted. There were 58 (74.4%) males and 20 (25.6%) females. There was a positive trend between time elapsed after the kidney transplantation and the quality of life score. Demographic variables such as income, age, location, etc. had no significant impact on the quality of life indicators. Discussion. Personalized treatment approaches including medication management, minimally invasive interventions and psychotherapeutic support can improve patients' satisfaction and long-term transplant outcomes. The obtained data confirm a close relationship between somatic complications and psychoemotional status of patients after a kidney transplantation, which should be taken into account in the development of clinical recommendations for the rehabilitation of this type of patients. Conclusion. The absence of any factors significantly affecting the scores of the social and environmental components of the WHOQOL-BREF questionnaire was shown. At the same time, the only factor affecting the physical and psychological state of the recipients was the time passed after a kidney transplantation, where there was a tendency to improve the quality of patients' life as the time after a kidney transplantation increased.
Keywords: Public health, Who-qol bref, Kidney transplantation, Quality of life
Cite this paper: S. S. Kariev, F. R. Nasirov, Evaluation of Patients' Life Quality in Urologic and Andrologic Complications in Recipients after Kidney Transplantation, American Journal of Medicine and Medical Sciences, Vol. 15 No. 7, 2025, pp. 2164-2169. doi: 10.5923/j.ajmms.20251507.16.
Article Outline
1. Introduction
- Terminal stage chronic kidney disease (CKD) is defined as a significant decline of renal function that is fatal without dialysis or transplantation [1]. The incidence of CKD is more than 1500 per million population in high prevalence countries such as the USA and Japan. Risk factors for CKD include hypertension, diabetes mellitus, obesity, and a history of acute renal failure [2]. About two-thirds of people with CKD receive hemodialysis, a quarter of patients have a kidney transplantation (KT), and one-tenth receive peritoneal dialysis. At the same time, KT is considered a superior method to chronic dialysis because it prolongs survival and alleviates uremic symptoms [3]. Kidney transplant recipients are at risk of developing various postoperative complications on the background of receiving immunosuppressive drugs and concomitant pathologies associated with long-term CKD [4-5]. Urologic complications (UC) constitute the second cause of morbidity after KT and rejection episodes, and may be associated with transplant loss and mortality [6-9].In patients with CKD, quality of life is influenced by the disease itself and the treatment option the patient chooses. A variety of factors affecting quality of life in patients on hemodialysis have been identified: age, gender, duration of dialysis, family care and support, vital status, patient adherence, and education level [9-11]. It is noted that elderly recipients have significantly lower graft survival rates, as well as a significantly higher risk of graft loss and mortality [12-13]. Life after KT has negative aspects such as strict immunosuppressant regimen and associated side effects, frequent physician visits, infections, uncertainty and worry about rejection episodes, potential graft loss, lifetime medical costs and unemployment.It is also important to consider personal, environmental, and clinical factors that negatively impact health-related quality of life. Quality of life evaluation is a useful tool in determining the efficiency of certain therapeutic interventions in patients with chronic diseases when complete cure is not possible [12-13]. Various tools such as WHOQOL-BREF, KTQ, SF-36, etc. can be used to measure the patient's quality of life. The aim of the study was to evaluate the life quality of recipients with urologic complications after related kidney transplantation.
2. Material and Methods
- We examined and treated 78 adult recipients (≥18 years of age) with UC after related KT who received outpatient and inpatient treatment at the Republican Specialized Scientific and Practical Medical Center of Urology from 2022 to 2025. A significant majority of patients (90.7%) were operated for terminal stage CKD in the outcome of chronic glomerulonephritis. In the remaining cases, polycystic kidney disease, chronic pyelonephritis and urinary tract anomalies were the indications for KT, i.e. the cause leading to terminal CKD. Data were collected using the WHOQOL-BREF questionnaire, which contained 25 questions focused on four domains (physical, psychological, social and environmental). The questionnaire was completed by telephone with the patient's prior consent. A total of 78 patients with an average age of 36.1±9.2 years were questioned. There were 58 (74.4%) males and 20 (25.6%) females. Thirty-four recipients (43.6%) lived in urban areas and the remaining 44 (56.4%) recipients were from rural areas. Fifty-four (69.2%) recipients were married and the remaining 24 (30.8%) were single. Twenty-nine (37.1%) recipients had educational status above the secondary level. Forty-two (53.8%) patients had various systemic disorders, such as diabetes, coronary heart disease, hypertension, hepatitis C, etc.
3. Results
- Mean quality of life scores based on the parameters of the WHOQOL-BREF questionnaire are presented in Figure 1.
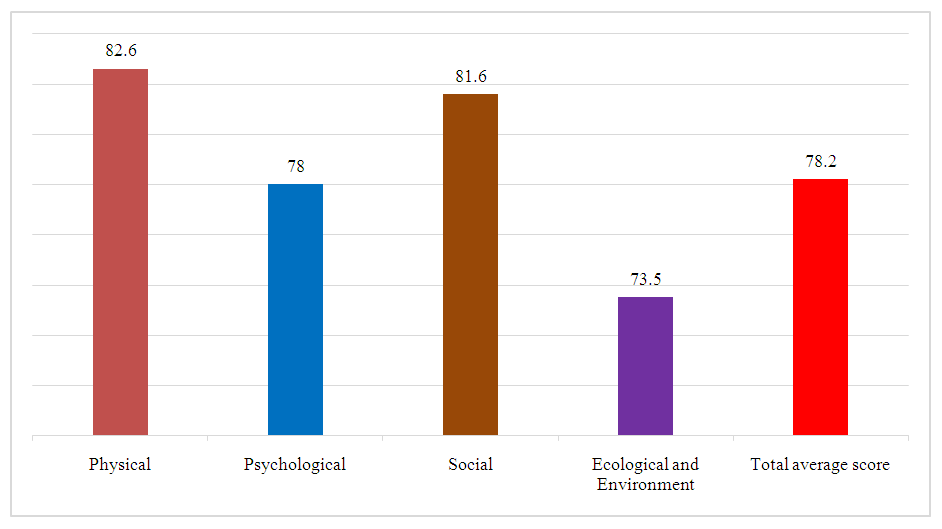 | Figure 1. Evaluation of the life quality of recipients with urologic and andrologic complications after related KT using the WHOQOL-BREF questionnaire |
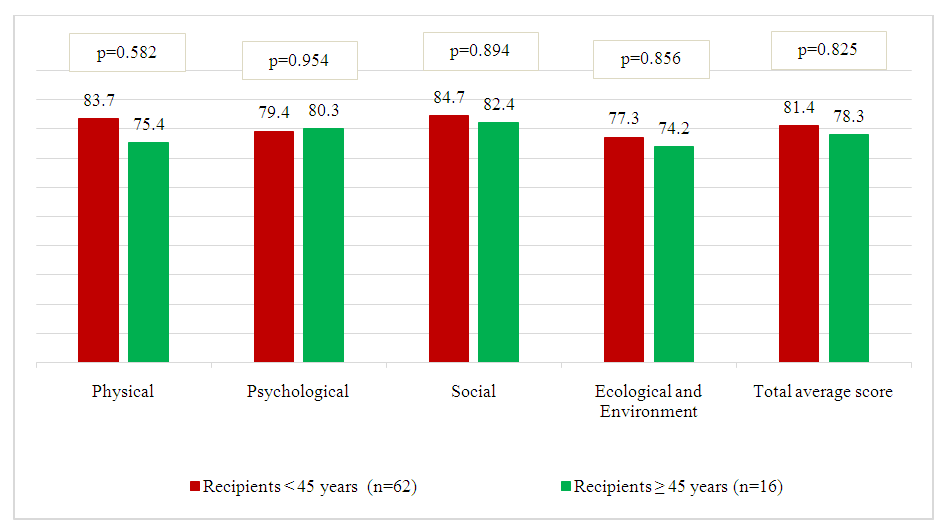 | Figure 2. Evaluation of the life quality of recipients with urologic and andrologic complications after related KT according to the WHOQOL-BREF questionnaire depending on the age group |
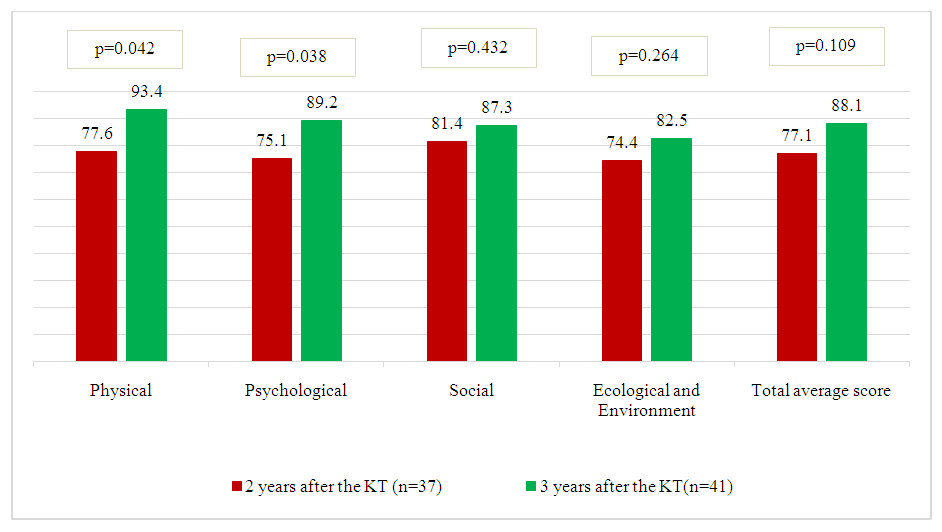 | Figure 3. Evaluation of the life quality of recipients with urologic and andrologic complications after related KT according to the WHOQOL-BREF questionnaire depending on the time after KT |
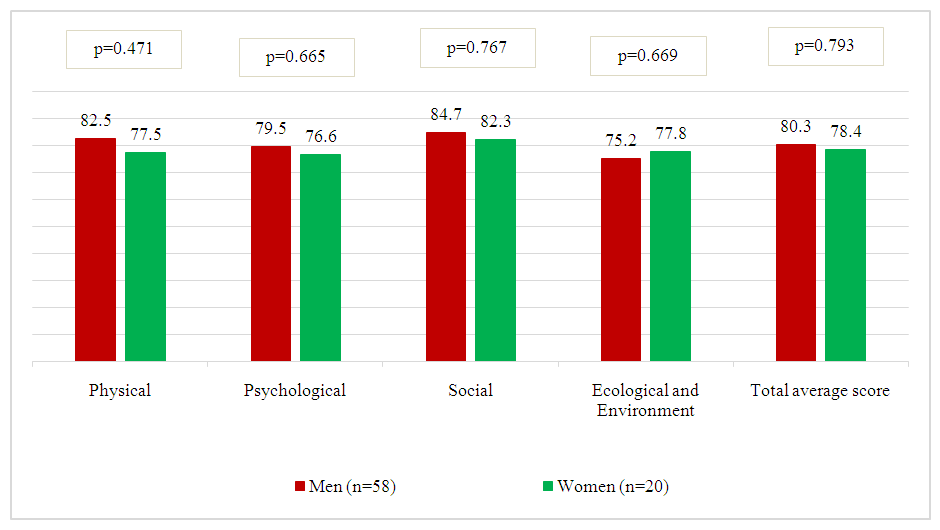 | Figure 4. Evaluation of the life quality of recipients with urologic and andrologic complications after related KT according to the WHOQOL-BREF questionnaire depending on gender |
 | Figure 5. Evaluation of the life quality of recipients with urologic and andrologic complications after related KT according to the WHOQOL-BREF questionnaire depending on marital status |
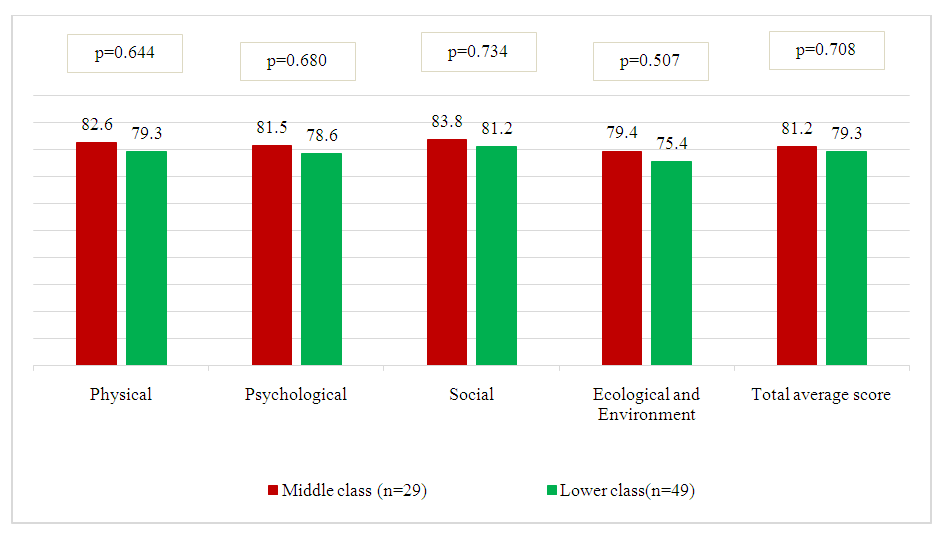 | Figure 6. Evaluation of the life quality of recipients with urologic and andrologic complications after related KT according to the WHOQOL-BREF questionnaire depending on socioeconomic status |
4. Discussion
- The data obtained during the study indicate a significant impact of urological and andrological complications on the quality of life of recipients after kidney transplantation. These complications include urethral strictures, vesicoureteral anastomotic strictures, orchitis, epididymitis, erectile dysfunction and hypogonadism, which is confirmed by a number of clinical and questionnaire observations conducted on the basis of SF-36, IIEF-5 questionnaires and other validated scales for assessing the quality of life.The results of the study are consistent with the data presented in the works of SpiritoL. et al. (2020), which revealed a significant deterioration in sexual function (decrease in IIEF 15) in the first 6–12 months after kidney transplantation, which also indicated a significant decrease in the psycho-emotional status and social activity of patients who experienced complications after transplantation. Our study revealed statistically significant differences between patients with and without urological-andrological complications according to physical and mental health scales. The decline in scores was particularly pronounced in the domains of “general health,” “social functioning,” and “vital activity”.Analysis of sexual function in male recipients revealed a high prevalence of erectile dysfunction of varying severity, including in patients under 50 years of age. It has been shown that kidney transplantation does not always lead to complete normalization of the hormonal profile and vascular function of the penis. Hypogonadism often persists, requiring early diagnosis and testosterone replacement therapy.The presence of infravesical obstruction and recurrent urinary tract infections also negatively affects physical comfort, disturbs sleep, increases anxiety levels and contributes to the development of depressive states. It confirms the importance of a multidisciplinary approach involving urologist, nephrologist, andrologist and psychotherapist in the management of such patients.The obtained data indicate the need for regular assessment of quality of life in kidney recipients as part of outpatient monitoring, especially in the presence of urological and andrological symptoms. Personalized treatment approaches including medication management, minimally invasive interventions and psychotherapeutic support can improve patients' satisfaction and long-term transplant outcomes.The obtained data confirm a close relationship between somatic complications and psychoemotional status of patients after a kidney transplantation, which should be taken into account in the development of clinical recommendations for the rehabilitation of this type of patients.
5. Conclusions
- The absence of any factors significantly affecting the scores of the social and environmental components of the WHOQOL-BREF questionnaire was shown. At the same time, the only factor affecting the physical and psychological state of the recipients was the time passed after a kidney transplantation, where there was a tendency to improve the quality of patients' life as the time after a kidney transplantation increased.Our study confirmed the need for regular evaluation of quality of life, physical and psychological aspects, and work capacity status in kidney transplant recipients.
Conflict of Interests’ Statement
- The authors declare no conflict of interest. This study does not include the involvement of any budgetary, grant or other funds. The article is published for the first time and is part of a scientific work.
ACKNOWLEDGEMENTS
- The authors express their gratitude to the management of the multidisciplinary clinic of Republican Specialized Scientific and Practical Medical Center of Urology for the material provided for our study.
Ethical Approval and Consent to Participate
- The Research Ethics Board of our institution does not require review or approval of case reports. Our research was carried out in accordance with the World Medical Association Code of Ethics (Declaration of Helsinki).
Source of Funding
- Each of the authors has reviewed and approved this manuscript. None of the authors has a conflict of interest, financial or otherwise. This manuscript is original, no part of it has been previously published and is not being considered for publication elsewhere. The corresponding author agrees to accept full responsibility for authorship at the submission and review stages of the manuscript.