Inoyatova Feruza Khidoyatovna1, Islamova Nodira Ulugbekovna2, Karimov Murodulla Yuldashevich3, Ismailov Nurxan Uralovich4
1Professor, Department of Medical and Biological Chemistry, Tashkent Medical Academy, Tashkent, Uzbekistan
2Assistant, Department of Medical and Biological Chemistry, Tashkent Medical Academy, Tashkent, Uzbekistan
3Professor, Head of the Department of Traumatology, Orthopedics and Military Field Surgery No.1, Tashkent Medical Academy, Tashkent, Uzbekistan
4Assistant, Head of the Department of Traumatology, Orthopedics and Military Field Surgery No.1, Tashkent Medical Academy, Tashkent, Uzbekistan
Correspondence to: Inoyatova Feruza Khidoyatovna, Professor, Department of Medical and Biological Chemistry, Tashkent Medical Academy, Tashkent, Uzbekistan.
| Email: |  |
Copyright © 2025 The Author(s). Published by Scientific & Academic Publishing.
This work is licensed under the Creative Commons Attribution International License (CC BY).
http://creativecommons.org/licenses/by/4.0/

Abstract
The dissertation examines the features of biochemical parameters of synovial fluid in chronic synovitis of the knee joint in order to identify their diagnostic and prognostic significance. A clinical and laboratory study was conducted in patients with acute and chronic forms of synovitis, including the analysis of such parameters as total protein, glucose, lactic acid, lactate dehydrogenase and alkaline phosphatase activity. Based on the data obtained, reliable differences in the biochemical characteristics of synovial fluid in various clinical forms of the disease were revealed. An algorithm for interpreting laboratory data to improve the accuracy of diagnosis and assess the prognosis of the course of chronic synovitis was developed. The results of the study can be used in the practice of traumatologists-orthopedists and rheumatologists for differential diagnosis, monitoring the effectiveness of treatment and preventing relapses of the inflammatory process in the knee joint.
Keywords:
Chronic synovitis, Synovial fluid, Knee joint, Biochemical markers, Diagnostics, Prognosis
Cite this paper: Inoyatova Feruza Khidoyatovna, Islamova Nodira Ulugbekovna, Karimov Murodulla Yuldashevich, Ismailov Nurxan Uralovich, Biochemical Indicators of Synovial Fluid in Patients with Acute and Chronic Knee Joint Synovitis, American Journal of Medicine and Medical Sciences, Vol. 15 No. 7, 2025, pp. 2147-2151. doi: 10.5923/j.ajmms.20251507.13.
1. Introduction
B in recent years, the frequency of synoviitis has been progressively increasing due to the increase in injuries of various origins, joint inflammatory diseases, joint damage in various somatic diseases, surgical interventions, and the introduction of various drugs into the synovial cavity [1,2]. Among these, the knee joint holds a special place, as it is the most traumatic and complex joint. According to the World Health Organization, knee joint injuries rank second among body parts injuries (9%), and third among all joint injuries (up to 50%) [3] According to the results, after arthroscopic intervention, cartilage damage occurs in 60-70% of knee joint injuries. The frequency of isolated cartilage injuries is 30%, and combined damage to the cartilage and other intra-articular structures of the knee joint reaches 70%, in 35-58% of cases, intra-articular cartilage damage is the result of a traumatic, contactless mechanism of injury and often takes on a chronic course. Improvement of treatment outcomes for knee joint injuries in the presence of hemarthrosis depends on accurate and rapid diagnosis of intra-articular injuries and subsequent selection of an adequate treatment method. Synovial fluid (SF), as one of the main organ-specific components of each joint, responds to any intra-articular processes by changing its composition and properties. At the current stage of medical diagnostics development, the study of CS changes using laboratory methods remains the most informative and accessible. Biochemical analysis of the CSF in acute knee joint injuries allows for the detection of disorders in protein, carbohydrate, and lipid metabolism, the presence of inflammatory and destructive processes, changes in the lipid peroxidation system (LPO) and antioxidant system (AOS) at the preclinical stage, predicting the outcome of the disease, and using optimal treatment tactics [4]. Significance of determining the activity of antioxidant defense enzymes in synovial fluid in predicting postoperative complications in patients with. The determination of necrotic substances in the knee joint is a prognostic marker of the severity of damage to the structural components of the knee joint [5]. The high frequency of knee joint lesions requires the development of diagnostic and therapeutic measures to prevent complications. Due to the development of diagnostic arthroscopy, the possibility of obtaining KJ, assessing its biochemical composition, and developing diagnostic criteria for the outcome of knee joint synovitis based on them is one of the pressing problems of clinical medicine and laboratory diagnostics.
2. Purpose of the Research
Purpose of the study: to study the biochemical parameters of synovial fluid in acute and chronic knee joint synovitis.
3. Materials and Methods
The study included 50 patients with knee joint synovitis admitted to the traumatology department of the 2nd TMA clinic. Among those with the acute process were 24 (48%), and chronic synovitis of the knee joint - 26 (52%). Of the total number of patients, 28 (56%) were men and 22 (44%) were women. The patients were between 25 and 69 years old, with an average age of 42.42±2.15 years for the acute process and 49.46±2.60 years for the chronic process. The distribution of patients by age and sex was carried out in accordance with WHO recommendations (2018). Mainly young and middle-aged individuals predominated. In the group of patients with acute synovitis, there were 14 (58.3%) men (41.7% of them young and 16.7% middle-aged) and 10 (41.7%) women (middle-aged). In the group of patients with chronic synovitis, there were 14 (53.8%) men, of whom 15.4% were young, 23.1% were middle-aged, and 15.4% were elderly, and 12 (46.2%) women, of whom 7.7% were young, 23.1% were middle-aged, and 15.4% were elderly. As can be seen from the data presented, acute knee joint synovitis was mainly characteristic of middle-aged men, while chronic synovitis was characteristic of both young, middle-aged, and elderly men, and for middle-aged and elderly women.The duration of chronic synovitis, previous injuries to the affected joint, and hereditary severity of osteoarthritis were determined. The diagnosis of acute and chronic knee joint synovitis was established jointly with traumatologists based on clinical and anamnestic data, MRI studies, and arthroscopy, which allows us to judge the presence of intra-articular pathology. Bauer-Jackson classification was used to assess the condition of the knee joint cartilage. The ISAKOS classification was used to assess meniscus injuries.The research material was CS taken during arthroscopy. The content of total protein, albumins, C-reactive protein (CRP), cholesterol, and glucose was determined using a MINDRAY BA-88A (China) biochemical analyzer using CYPRESS Diagnostics (Belgium) reagents. MDA content was determined by the method [7] catalase activity according to the method of [8]. As a comparison, we used literature data and reference values of test system manufacturers. The digital material was processed using the variational statistics method using the Statistika software package.
4. Results and Discussion
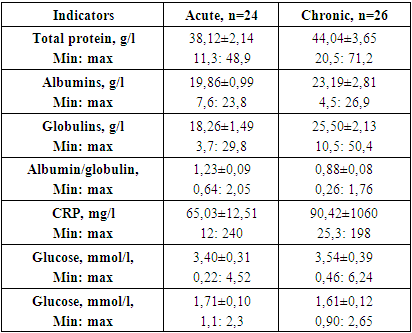
According to literature data, the total protein content in CS does not exceed 10-20 g/l, averaging 14.9±1.22 g/l. It is mainly represented by albumins and globulins, the albumin-globulin ratio is 0.5-2.0 [10]. Our studies showed that in the CS of patients with acute knee joint synovitis, the total protein content averaged 38.12±2.14 g/l, ranging from 11.3 g/l to 48.9 g/l (Table 1). If only in 8.8% of patients this indicator was within 20 g/l, then in the remaining 91.2% of patients it exceeded the normative values. At the same time, in patients with a chronic course of synovitis, the total protein content was 44.04±3.65 g/l, ranging from 20.5 g/l to 71.2 g/l. At the same time, in 7.7% of patients, it was up to 20 g/l, in 50% - from 21 to 50 g/l, and in 42.3% - more than 50 g/l. This phenomenon is explained not only by increased permeability of the synovial membrane during inflammation but also by increased production of γ-globulins by synovial cells. Table 1. Biochemical indicators of synovial fluid in patients with acute and chronic synovitis, M±m
 |
| |
|
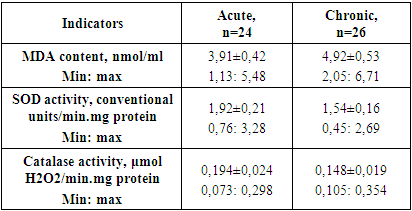
According to literature data, the albumin content in normal CS is 72% of the total protein (10 to 14 g/l). In our studies, the albumin content in the CS of patients with acute knee joint synovitis averaged 19,86±0.9 g/l, ranging from 7.6 g/l to 23.8 g/l (Table 1). If only in 8.3% of patients this indicator was within 14 g/l, then in the remaining 91.7% of patients it exceeded the normative values. At the same time, in patients with a chronic course of synovitis, the albumin content was 23.19±2.81 g/l, ranging from 4.5 g/l to 26.9 g/l. At the same time, in 7.7% of patients, it was up to 14 g/l, in 92.3% - exceeded these values. Analysis of globulin levels showed the following results: in the acute course averaged 18.26±1.49 g/l, ranging from 3.7 g/l to 29.8 g/l (see table. 1). If only in 8.3% of patients this indicator was within 6 g/l, then in 50% it reached 20 g/l, in the remaining 41.7% of patients it was higher than 20 g/l. In patients with a chronic course of synovitis, the globulin content was 25.50±2.13 g/l, ranging from 10.5 g/l to 50.4 g/l, and in all patients, it exceeded the normative values. At the same time, in 26.9% of patients, it was up to 20 g/l, in 73.1% - above 20 g/l. At the same time, in patients with an acute course of the inflammatory process, the albumin/globulin coefficient was 1.23±0.09, ranging from 0.64 to 2.0 literature data [10]. At the same time, in patients with a chronic course, this indicator was 0.88±0.08 and ranged from 0.26 to 1.76. At the same time, in 23.1% of cases, it slightly exceeded 1.0, in 46.1% of cases, it was up to 0.5, and in the remaining 30.8% of cases, it was below 0.5. The obtained results indicate the presence of pronounced inflammatory-destructive processes in patients with chronic knee sinusitis, indicating a degradation of the knee joint cartilage (Myres S.L. et al., 1996).An increase in the concentration of acute-phase proteins: CRP, α-antitrypsin, ceruloplasmin, etc., is of particular importance. According to literature data and regulatory values of test system manufacturers, the content of CRP with CS ranges from 0 to 6 mg/l. Our studies showed that in the CS of patients with acute knee joint synovitis, this indicator increased to 65.03±12.51 ml, ranging from 12 mg/l to 240 mg/l. In 41.7% of patients, the CRO content did not exceed 50 mg/l, in 41.7% - from 51 to 100 mg/l, and in 16.7% of patients over 100 mg/l, and these were severe knee joint injuries with meniscus damage, high degree of turbidity with high leukocyte and protein content. When analyzing the CS of patients with chronic synovitis, the CRO content averaged 90.42±10.60 mg/l, ranging from 25.3 mg/l to 198 mg/l. In 30.8% of patients, the CRO content did not exceed 50 mg/l, in 23.1% - from 51 to 100 mg/l, and in 46.2% of patients over 100 mg/l and these were severe bilateral osteoarthritis of 2-4 degrees of severity, degenerative changes in the medial menisci, chondromalacia of the cartilage, Patello femoral arthrosis. The color of CS acquired a milky-pure hue with a high content of leukocytes, protein, and crystals, especially urates. According to literature data, CRP is one of the most important acute-phase reagents and its level increases in both serum and CS in joint diseases, especially in rheumatoid and reactive arthritis, microcrystalline synovitis [12]. Another important parameter characterizing the CS state is the glucose level. This is a more specific, but less sensitive indicator of joint inflammation, as the level of glucose in the CS decreases significantly in inflammatory arthropathies (Shmerling R.H. et al., 1990). According to literature data, this indicator averages 3.5 - 5.5 mmol/l. In our studies, in patients with acute knee joint synovitis, the blood glucose content in the CS was 3.91±0.15 mmol/l, ranging from 2.2 mmol/l to 4.52 mmol/l. At the same time, glucose levels up to 3.5 mmol/l were determined in 16.7% of patients and above 3.5 mmol/l in 83.3% of patients. In patients with chronic knee sinusitis, blood glucose levels averaged 4.01±0.30 mmol/l, ranging from 1.23 mmol/l to 6.24 mmol/l. At the same time, glucose levels up to 3.5 mmol/l were established in 38.5% of patients and above 3.5 mmol/l in 46.1% of patients, exceeding the upper limits of the norm in 7.7% of patients. Considering that the articular cartilage represents a vascular-free zone, anaerobic glycolysis predominates in it. If the detected decrease in blood sugar levels to 3.5 mmol/l indicates the presence of an inflammatory process with the development of degenerative processes, then 2 patients with high blood sugar levels were diagnosed with type 2 diabetes mellitus.It should be noted that the total cholesterol content in CS averages 71 g/l (1.84 mmol). In our studies, the cholesterol content in the CS of patients with acute synovitis was 1.71±0.10 mmol/l, ranging from 1.1 to 2.3 mmol/l. At the same time, in 58.3% of the examined, this indicator did not exceed 2.0 mmol/l, while in 41.7% of patients it was higher than 2.0 mmol/l. In a patient with chronic synovitis, the level of total cholesterol averaged 1.61 mmol/l, ranging from 0.9 mmol/l to 2.65 mmol/l. At the same time, in 68.2% of patients, it did not exceed 2.0 mmol/l, and in 31.8% of those examined, it was higher than 2.0 mmol/l. In our opinion, determining total cholesterol has no diagnostic value in assessing the severity of inflammatory-destructive processes in the knee joint.Studies by several scientists have shown the presence of cholesterol (3.8±0.4 mmol/l) in the CS in the form of complex esters of acids (palmitic, palmitic-oleic, stearic, oleic, arachidonic), which in the physiological temperature range (25-41°C) are thermotropic liquid crystalline compounds . The molecules of liquid crystalline cholesterol compounds are oriented according to the cartilage microrelief in the direction of sliding joint surfaces, due to which the friction coefficient in the joint decreases. They are part of the CS, are located in microbores on the surfaces of the cartilage, and form a liquid-crystalline-oriented structure consisting of many nematode layers. The distance between the layers is equal to the cross-sectional size of cholesterol derivative molecules. In the zones of actual contact of collagen fibers, the minimum thickness of the lubricating layer is S/2, where S is the pitch of the liquid crystalline compound spiral. Near the actual contact zones, the thickness of the liquid crystalline layer is also a multiple of S/2. Such a structure is similar to the structure of layered solid lubricants, but the molecular interaction of the layers is small due to their liquid-crystalline state. During friction, the displacement is localized between layers, the slight slippage of which ensures low friction in the joint. The disappearance of microrelief anisotropy on the cartilage surface prevents the formation of liquid crystalline lubricating layers, which explains the pathogenesis of cartilage destruction in diffuse connective tissue diseases.It is well known that the articular cartilage is a vascular-free tissue that receives nourishment and oxygen supply through diffusion from the synovial fluid and subchondral bone. Chondrocytes on the articular surface are exposed to approximately 6 to 10% O2, while chondrocytes in the deepest layers of the articular cartilage can only access 1-6% O2 or less «Osteoarthritis and Cartilage Europe PMC». In this regard, joint chondrocytes are capable of extracting up to 75% of their ATP requirement from anaerobic glycolysis, ensuring their adaptation to low O2 in the environment. In the development of pathological processes in the joint, the rate of absorption in the synovial membrane decreases, the permeability to the joint cavity increases, which leads to the accumulation of fluid in it. In CCS, local mediators contribute to the development of membrane-destructive or inflammatory-dystrophic changes in the lesion site, which determines the continuous recurrent course of this disease. The processes occurring in joint and paraarticular tissues can be assessed by examining the chemical composition of the joint joint. In chronic synovitis, there may be pronounced differences in the CS depending on the degree of local arthritis activity. In this regard, the study of the content of MDA and the activity of antioxidant defense enzymes (AOP) in the CS of patients with acute and chronic knee joint synovitis was of interest (Table 2). As can be seen from the table, more pronounced hyperlipoperoxidation is characteristic of patients with a chronic course of the disease. Thus, the MDA content in patients with acute synovitis was 3.91±0.42 nmol/ml and ranged from 1.13 nmol/ml to 5.48 nmol/ml. At the same time, MDA values up to 3 nmol/ml were detected in 37.6% of patients, while in 62.4% of patients it exceeded 2 nmol/ml. These were mainly patients with post-traumatic hemosynovitis. This was expected, as it occurs against a background of more pronounced intoxication and destruction of membrane structures. On the other hand, in post-traumatic etiology, the sympathetic autonomic nervous system is activated, leading to the development of the body's response to the damaging agent with increased functional activity of the macrophago-reticular system. In patients with chronic knee sinusitis, the MDA content in the CS averaged 4.92±0.53 nmol/ml, ranging from 2.05 nmol/ml to 6.71 nmol/ml. At the same time, in 26.4% of the examined, it did not exceed 3 nmol/ml, while in the remaining 73.6% of patients, these values were higher. This coincided with more pronounced inflammatory-degenerative changes in the patients' joints. Table 2. Biochemical indicators of synovial fluid in patients with acute and chronic synovitis, M±m
 |
| |
|
It should be noted that LPO processes are controlled by enzymatic and non-enzymatic AOS, whose main enzymes are superoxide dismutase (SOD) and catalase, which participate in the neutralization of active forms of oxygen and peroxide radicals. LPO and AOS are balanced, as LPO products are normal metabolites of functionally active cells. However, the activation of phagocytosis during infectious-inflammatory processes, oxidative processes in mitochondria and microsomes, and the xantioxidase system contribute to the predominance of LPO over AOZ. Therefore, many authors recommend studying the activity of AOZ enzymes.The conducted studies showed that in patients with an acute course of the pathological process, the activity of SOD in the CS was 1.92±0.21 conditional units/min.mg of protein, ranging from 0.76 conditional units/min.mg of protein to 3.28 conditional units/min.mg of protein. Higher values were characteristic of patients with traumatic hemarthrosis, which, in our opinion, is associated with the destruction of erythrocytes and their washing into synovial fluid. In 14.7% of patients, the enzyme activity did not exceed 1 conditioned unit/min.mg protein, in 65.4% - ranged from 1 to 2 conditioned units/min.mg protein, and in 19.1% - exceeded 2 conditioned units/min.mg protein. In patients with a chronic course of the pathological process, the activity of SOD in the CS was 1.54±0.16 conditional units/min.mg of protein, varying from 0.45 conditional units/min.mg of protein to 2.69 conditional units/min.mg of protein. Higher values were characteristic of patients with pronounced inflammatory-degenerative changes. In 41.4% of patients, the enzyme activity did not exceed 1 conditioned unit/min.mg protein, in 37.6% - ranged from 1 to 2 conditioned units/min.mg protein, and in 21.0% - exceeded 2 conditioned units/min.mg protein. Analysis of catalase activity in the CS of patients with synovitis showed lower values in patients with chronic course (see Table. Thus, in patients with an acute course of the pathological process, catalase activity was 0.194±0.024 μmol H2O2/min.mg protein, varying from 0.073 μmol H2O2/min.mg protein to 0.298 μmol H2O2/min.mg protein. Higher values were also characteristic of patients with traumatic hemarthrosis. In 14.7% of patients, the enzyme activity did not exceed 0.100 μmol H2O2/min.mg protein, in 65.4% - it ranged from 0.100 to 0.200 μmol H2O2/min.mg protein, and in 19.1% - it exceeded 0.200 μmol H2O2/min.mg protein. In patients with a chronic course of the pathological process, the activity of SOD in the CSF was 0.148±0.019 μmol N2O2/min.mg of protein, varying from 0.105 μmol N2O2/min.mg of protein to 0.354 μmol N2O2/min.mg of protein. Higher values were characteristic of patients with pronounced inflammatory-degenerative changes. In 41.4% of patients, enzyme activity ranged from 0.100 to 0.200 μmol H2O2/min.mg protein, in 58.6% - exceeded 0.200 μmol H2O2/min.mg protein. It should be said that chronic synovitis is a long-term process. Previous studies conducted by us in patients with chronic synovitis of the knee joint of various etiologies and the activity of the inflammatory process showed the development of imbalance in the LPO-AOS system, the severity of which depended on the activity of the inflammatory process, its primary and secondary nature, hormonal dependence, and the duration of the pathological process [13]. In patients with a secondary pathological process and hormonal dependence, depletion of the AOS enzyme systems is observed. In our opinion, this is due to the slowing of biosynthetic processes and the beginning of the formation of arthrosis in the knee joint. Due to the reduction of the periarticular space, the narrowing of gaps, the supply of nutrients and oxygen decreases, trophic processes slow down, causing joint deformities to form. According to the authors, the research results allow us to speak about the diagnostic value of studying LPO products and the activity of AOS enzymes in CS to determine the stage of the pathological process.
5. Conclusions
Thus, the development of the pathological process in the joint is accompanied by various biochemical disorders, which can be detected using standard laboratory tests. Determining other biochemical parameters in CS is currently of greater research interest and requires clarification of their diagnostic informativeness. Based on the obtained results, the following conclusions can be drawn:1. The content of total protein, albumins, and globulins in synovial fluid should not exceed 10-20 g/l, averaging 14.9±1.22 g/l. In patients with acute and chronic knee joint synovitis, the total protein content was 38.12±2.14 and 44.04±3.65 g/l, albumins 19,86±0.9 and 23.19±2.81 g/l, globulins 18.26±1.49 and 25.50±2.13 g/l, indicating the presence of pronounced inflammatory-destructive processes. 2. The content of CRP with CS ranges from 0 to 6 mg/l. In patients with acute and chronic synovitis of the knee joint, its content reached 65.03±12.51 and 90.42±10.60 mg/l, which corresponded to the presence of severe bilateral osteoarthritis of 2-4 degrees of severity, degenerative changes in the medial menisci, and chondromalacia of the cartilage.3. The content of glucose and cholesterol in CS is 3.5-5.5 mmol/l and 1.84 ml. In patients with acute and chronic knee joint synovitis, these indicators did not change significantly.4. MDA content in patients with acute and chronic synovitis was 3.91±0.42 and 4.92±0.53 nmol/ml, SOD activity - 1.92±0.21 and 1.54±0.16 conv. units/min.mg protein, catalase activity - 0.194±0.024 and 0.148±0.019 μmol H2O2/min.mg protein, the severity of their changes depended on the degree of inflammatory-degenerative changes.
References
| [1] | Gulyamov Yo.B., Inoyatova F.Kh., Karimov M.Yu. Biochemical aspects of synovitis of various etiologies // Pathology - Tashkent, 2006. – No 4. - P. 53-55. |
| [2] | Karimov M.Yu., Inoyatova F.Kh., Kholmurodov U.T., Tolochko K.P. Significance of determining the activity of antioxidant defense enzymes in synovial fluid in predicting postoperative complications in patients with hemarthrosis // Medical Journal of Uzbekistan. - 2019. - No. 1. - P. 93-98. |
| [3] | Zushi Yu.Kh., Saydalin D.M., Kurbansupiev M.D., Saydalina M.S., Alihodzhaev S.S. Knee joint arthroscopy in injuries // KazNMU Bulletin. - 2015. - No 2. - P. 305-308. |
| [4] | Murod Karimov, Feruza Inoyatova, Umid Kholmurodov & Kirill Tolochko Biochemical Aspects of Preclinical Prediction of the Severity of the Knee Joint Injuries in Acute Period Global Journal of Medical Research: H Orthopedic and Musculoskeletal System Volume 19 Issue 1 Version 1.0 Year 2019 Type: Double Blind Peer Reviewed International Research Journal Publisher: Global Journals Online ISSN: 2249-4618 & Print ISSN: 0975-5888. |
| [5] | Karimov M.Yu., Inoyatova F.Kh., Kholmurodov U.T., Tolochko K.P. A new method for predicting the severity of acute knee joint injury // Journal of Theoretical and Clinical Medicine, 2019. - No1. - P. 74-78. |
| [6] | Karimov M.Yu., Yuldashev A.Yu., Gulyamov Yo.B., Our experience in diagnosing and treating chronic knee joint synovitis syndrome. // Visnik ortopedii, travmatologii ta protezuvaniya. - Ukrainian Scientific and Practical Journal, 2010. - No.4. -P. 61-66. |
| [7] | Andreeva L.I., Kozhemyakin L.A., Kushkin A.A. Modification of the method for determining lipid peroxides in a test with thiobarbituric acid. // Laboratory. - 1989. - No.- P. 41-43. |
| [8] | Kuikka P.I., Sillanpää P., Mattila V.M., Niva M.H., Pihlajamäki H.K. Magnetic resonance imaging in acute traumatic and chronic meniscal tears of the knee: a diagnostic accuracy study in young adults // Medicine (Kaunas), - 2019. - Vol. 55, 10. P. 45-55. |
| [9] | Lyubimova L.V., Pavlova S.I., Nikolaev N.S., Lyubimov E.A., Pchelova N.N., Emelianov V.Yu. Federal State Budgetary Institution "Federal Center for Traumatology, Orthopedics and Endoprosthetics" of the Ministry of Health of the Russian Federation (Cheboksary) Federal State Budgetary Educational Institution of Higher Education "Chuvash State University named after I.N. Ulyanov 2024. |
| [10] | Matveyeva Y.L., Spirkina E.S., Gasanova A.G., Buravtsov P.P., Biryukova M.Yu., Chegurov O.K. Biochemical changes of synovial fluid in patients with osteoporosis of the knee joint of various etiology. Acta Biomedica Scientifica. 2013; (5): 60-63. (In Russ.) |
| [11] | Kotelkina, G.Yu. Struchko, L.M. Merkulova, O.Yu. Kostrova, I.S. Stomenskaya, N.Yu. Timofeeva Characteristics of Synovial Fluid in Normal Conditions and in Some Pathological Processes. Acta medica Eurasica. 2017. № 4 УДК 616.72-008.8-076.5 ББК 54.18. |
| [12] | Gulyamov Yo.B., Inoyatova F.Kh., Karimov M.Yu. Biochemical aspects of synovitis of various etiologies // Pathology - Tashkent, 2006. - No4.-P.53-55. Gulyamov Yo.B. Choosing a method of surgical treatment of chronic synovies of the knee joint // Abstract of diss. |
| [13] | Onis Singhal, Viplesh Kaur, Shivani Kalhan, Manish Kumar Singhal, Anshu Gupta, YV Machave1 Department of Pathology, Saraswathi Institute of Medical Sciences, Hapur, Uttar Pradesh, 1 Bharati Vidyapeeth University, Pune, Maharashtra, India Arthroscopic synovial biopsy in definitive diagnosis of joint diseases: An evaluation of efficacy and precision [Downloaded free from http://www.ijabmr.org on Wednesday, September 28, 2016, IP: 92.214.167.145]. |
| [14] | Christopher J. Burke mbchb, Hamza Alizai MD, Luis S Beltran MD, Ravinder R. Regatte phdfirst published: 08 January 2019 MRI of synovitis and joint fluid Published in final edited form as: J Magn Reson Imaging. 2019 Jan 8; 49(6): 1512–1527. https://pubmed.ncbi.nlm.nih.gov/30618151/. |

 Abstract
Abstract Reference
Reference Full-Text PDF
Full-Text PDF Full-text HTML
Full-text HTML